
Remember me
The earliest data showing the efficacy of asfotase alfa were from animal models of HPP. A murine model with homozygous knockout of tissue-nonspecific ALP (Alpl−/−) was developed in 1997 that recapitulated the HPP phenotype seen in human infants, including weight loss and seizures [34]. Asfotase alfa treatment restored normal skeletal morphology and prevented lethal seizures in Alpl−/− mice [35]. In subsequent analyses, asfotase alfa treatment rescued craniofacial bone and root dentin mineralization, as well as defective enamel formation in teeth of Alpl−/− mice [36,37,38]. Recent preclinical studies have shown subtle advantages of initiating prenatal asfotase alfa treatment rather than starting treatment at birth [39, 40].
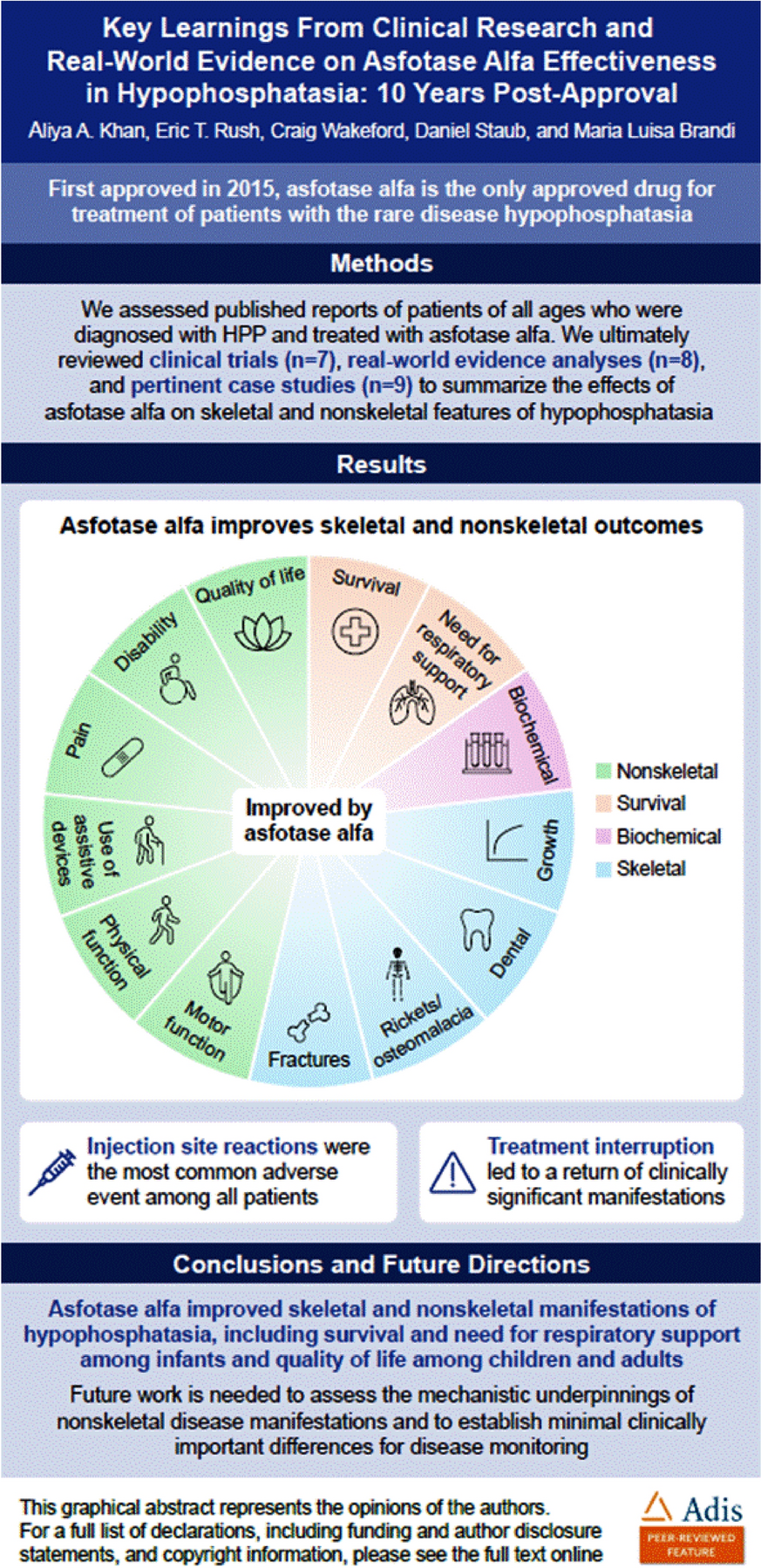
Disease assessments in patients with HPP typically include clinical and radiographic evaluations to assess for rickets, pseudofractures, or fractures (Tables 1, 2) [5, 6, 20, 29, 41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76], and laboratory data to assess alterations in serum levels of HPP biomarkers [19]. These clinical, radiographic, and biochemical endpoints are often used to evaluate ERT effectiveness in clinical trials and observational studies. Assessment of patients with HPP has historically focused on the radiologically demonstrated effects on bone pathology and, among infants with life-threatening disease, overall survival. The emergence of new assessment methods, better understanding of disease burden across all ages, and availability of ERT have prompted rethinking of how patients with HPP are diagnosed and evaluated. While increasing survival among infants remains an important treatment goal in this age group, the clinical focus has expanded to address improving nonskeletal outcomes, including physical and motor function, mobility, pain, and disability in patients with late-onset (first manifestations after 6 months of age), non–life-threatening HPP, because of their significant impact on patients’ QoL.
Table 1 Clinical endpoints assessed in patients with HPPTable 2 Summary of studies reporting clinical outcomes in HPP with asfotase alfaSurvival and Respiratory SupportSurvival was low among untreated patients who manifested signs and symptoms of HPP before 6 months of age (early-onset HPP) but was greatly improved by asfotase alfa treatment [5, 12, 76]. In a retrospective chart review of untreated patients with HPP, 73% (35/48) who developed life-threatening symptoms of HPP before 6 months of age died before reaching 14 months of age [12]. In another analysis of data from patients with life-threatening disease, survival after 1 year was 95% among patients treated with asfotase alfa compared with only 42% among historical controls (Fig. 1A) [5]. In a 5-year real-world analysis of asfotase alfa effectiveness, which included 6 patients younger than 1 year of age, all patients survived after initiating asfotase alfa treatment, highlighting the impact of treatment on survival [76].
Fig. 1
Asfotase alfa treatment improves survival and decreases need for respiratory support in infants and young children with life-threatening HPP. (A) Survival in historical controls and treated patients with life-threatening HPP, reproduced from Whyte et al. 2016, with permission [5]. (B) Respiratory support requirement; studies included children with HPP who first displayed signs and symptoms of HPP at age < 6 months [5, 6, 65, 69]. Follow-up time varies as indicated: Whyte et al. 2012—48 weeks; Whyte et al. 2016—up to 5.5 years; Kitaoka et al. 2017—up to 1.8 years; Hofmann et al. 2019—up to 6 years. a84% observed survival; 31 of 37 treated patients survived to 5 years of age
Patients with life-threatening, early-onset HPP frequently require respiratory support owing to hypomineralization of the ribs and pulmonary hypoplasia, both of which can cause respiratory failure [6, 65, 77]. Types of respiratory support include use of supplemental oxygen, continuous positive airway pressure, biphasic positive airway pressure, or tracheostomy with mechanical ventilation [5, 6, 65, 69]. Across four studies, the percentage of patients who required respiratory support before starting asfotase alfa treatment ranged from 35% to 91% (Fig. 1B) [5, 6, 65, 69]. In these studies, asfotase alfa treatment decreased dependence on respiratory support, with one study showing that only 10% of patients still needed support at last follow-up (up to 5.5 years) [5]. In two of these studies, ventilator-free survival, defined as the percentage of patients who were alive and not receiving ventilator support after asfotase alfa treatment, was achieved in 84% (38/45) and 100% (5/5) of patients [65, 69].
SeizuresVitamin B6-responsive seizures are reported in approximately 10% of all children enrolled in the Global HPP Registry, although this proportion is higher among children < 6 months of age [1, 14]. In a small analysis of historical controls who experienced seizures and did not receive ERT, none of the 10 patients survived [5]. However, survival was 77% (10/13) among patients who received asfotase alfa treatment [5]. In a case study, asfotase alfa treatment led to cessation of seizures in an infant who started treatment at post-natal day 2 [78]. The patient experienced seizures again after treatment interruption, which progressed to acute encephalopathy [78]. Seizures were again mitigated upon reinitiation of asfotase alfa treatment [78], suggesting the efficacy of asfotase alfa in preventing seizures in infants with HPP.
Skeletal and Dental ParametersFracturesOver one-third of adults assessed in the Global HPP Registry have a history of recurrent and poorly healing fractures [1]. Limited evidence suggests that asfotase alfa treatment can improve fracture healing and reduce fracture incidence in patients with HPP. In a case series of 2 adults with HPP, treatment with asfotase alfa was associated with marked healing of pre-existing fractures. One of these patients had a history of a femoral pseudofracture with little evidence of healing over the course of 17 years, but experienced notable healing 11 months after initiating treatment with asfotase alfa, as evidenced by near resolution [79]. An additional case series of 2 adults with femoral fractures showed that 4–6 months of treatment with asfotase alfa promoted fracture healing [16]. Accelerated fracture consolidation with asfotase alfa was associated with improved clinical symptoms and pain-free normal motor function [79, 80]. In an observational study, 13% (3/24) of adults experienced fractures after 1 year of treatment with asfotase alfa [48]. In contrast, the prevalence of fractures among untreated adults has been shown to range from 37% to 95% [1, 73, 81, 82].
OsteomalaciaIn another study, osteomalacia was assessed by bone histomorphometry of samples obtained via transiliac bone biopsy in patients 13–66 years of age who received asfotase alfa compared with controls [68]. Mean osteoid volume per bone volume decreased by 0.8% after 1 year of treatment with asfotase alfa but increased by 0.2% after 6 months in untreated patients. Mean osteoid thickness was 109% of that reported in a healthy population at baseline and did not significantly change with asfotase alfa treatment. Baseline mean mineralization lag time in patients with HPP was 891% of that of a healthy population and was significantly decreased by 580% after 1 year of asfotase alfa treatment, suggesting improvement. The improvements in osteomalacia were accompanied by normalization of biomarkers of disease, including median reductions of 2.2 µM in serum PPi and 254.5 ng/mL in serum PLP after 6 months of asfotase alfa treatment. Median PPi concentration among all patients was 3.4 µM (normal range in adults: 1.0–5.8 µM; normal range in adolescents aged 13–18 years: < 0.8–4.8 µM) and median PLP concentration was 39.9 ng/mL (normal range in adults: 2.8–26.7 ng/mL; normal range in adolescents: 5.7–61.2 ng/mL) after 6 months of treatment.
Bone Metabolism BiomarkersAsfotase alfa treatment significantly improves biochemical markers of bone and mineral metabolism, indicating that treatment-mediated mineralization may enable bone remodeling and turnover of previously unmineralized bone. In one study measuring markers of bone turnover, including osteocalcin, procollagen type 1 N-propeptide, and tartrate-resistant acid phosphatase 5b, transient changes occurred after 3 and 6 months of treatment and reverted to near-baseline levels after 12 months [29]. Statistically significant but transient increases in parathyroid hormone were also observed at 3 and 6 months after initiating asfotase alfa [29]. Serum calcium or phosphorus are sometimes elevated in patients with HPP, although no significant change in either marker was observed over the course of up to 2 years of asfotase alfa treatment [29, 73]. In an independent analysis of adults who first had signs and symptoms of HPP in childhood, asfotase alfa treatment decreased plasma PPi in a dose-dependent manner [70]. Relative to PPi values among patients treated with 0.5 mg/kg asfotase alfa, the least squares mean changes in PPi were − 1.2 µM among patients treated with 2.0 mg/kg asfotase alfa and − 1.9 µM among those treated with 3.0 mg/kg asfotase alfa; similarly, least squares mean changes in PLP were − 29.5 ng/mL and − 34.0 ng/mL, respectively. In this study, normal ranges for PPi and PLP in adults aged > 18 years were 1.0–5.8 µM and 2.8–26.7 ng/mL, respectively [29].
RicketsNearly one-third of children with HPP present with rickets before initiating asfotase alfa treatment [14]. The Radiographic Global Impression of Change (RGI-C) is a validated 7-point scale developed for assessment of radiographic features, including rickets, in children with HPP [42]. A 2-point improvement in RGI-C score was observed as early as 6 weeks after asfotase alfa treatment initiation among children in clinical trials; results were sustained at long-term follow-up of 5–7 years (Fig. 2A) [6, 64,
Comments (0)