
Remember me
Between October 19, 2016, and April 29, 2019, 649 patients with rheumatic disease were enrolled across 71 sites and received treatment with CT-P13, including 142 (21.9%) with RA, 411 (63.3%) with AS, and 96 (14.8%) with PsA. Baseline demographic and clinical characteristics by indication and treatment group are summarized in Tables 1, 2, and 3. Additional details of medical history and previous and concomitant treatments are provided in Supplementary Material Tables S1–S3.
Table 1 Demographics and disease characteristics for patients with RA treated with CT-P13Table 2 Demographics and disease characteristics for patients with AS treated with CT-P13Table 3 Demographics and disease characteristics for patients with PsA treated With CT-P13Among patients with RA (N = 142), median (Q1, Q3) age was 62 (55, 68) years and 75.4% were female (Table 1). Overall, 49.3% (n = 70) of patients were naive to IFX before starting CT-P13 (IFX-naive), 48.6% (n = 69) switched from IFX originator or another IFX biosimilar to CT-P13 (IFX-switched), and 2.1% (n = 3) were previously treated with IFX (originator or biosimilar) but received another advanced treatment before switching to CT-P13 (other). At baseline, mean (± SD) DAS28 scores were 3.8 (± 1.4) and 2.9 (± 1.2) for IFX-naive and IFX-switched patients, respectively; mean (± SD) SDAI scores were 22.9 (± 18.0) and 12.7 (± 10.9), respectively. Median (Q1, Q3) baseline CRP concentrations were 5.0 (1.4, 12.0) and 3.0 (1.9, 7.5) mg/l for IFX-naive and IFX-switched patients, respectively.
Overall, 72.5% (n = 103) of all patients with RA were already on CT-P13 at inclusion, for a mean (± SD) duration of 12.88 (± 21.48) months. Among these patients, mean (± SD) DAS28 scores were 4.80 (± 1.16) and 2.62 (± 0.85) for IFX-naive and IFX-switched patients, respectively; mean (± SD) SDAI scores were 36.0 (± 19.8) and 8.3 (± 5.4), respectively; median (Q1, Q3) CRP concentrations were 10.6 (4.0, 26.0) and 3.6 (1.0, 8.0) mg/l, respectively.
Among patients with AS (N = 411), median (Q1, Q3) age was 47 (39, 56) years and 41.1% were female (Table 2). Overall, 46.0% (n = 189) of patients were IFX-naive, 48.9% (n = 201) were IFX-switched, and 5.1% (n = 21) had other treatment history. At baseline, mean (± SD) BASDAI scores were 4.18 (± 2.13) and 2.71 (± 2.03) for IFX-naive and IFX-switched patients, respectively; mean (± SD) BASFI scores were 3.70 (± 2.48) and 2.95 (± 2.36), respectively. Median (Q1, Q3) baseline CRP concentrations were 3.2 (1.0, 9.0) and 2.5 (1.0, 4.5) mg/l for IFX-naive and IFX-switched patients, respectively.
Overall, 76.6% (n = 314) of all patients with AS were already on CT-P13 at inclusion, for a mean (± SD) duration of 12.70 (± 9.5) months. Among these patients, mean (± SD) BASDAI scores were 5.54 (± 1.93) and 2.56 (± 2.14) for IFX-naive and IFX-switched patients, respectively; mean (± SD) BASFI scores were 5.24 (± 2.25) and 3.29 (± 2.60), respectively; median (Q1, Q3) CRP concentrations were 5.0 (2.1, 16.6) and 2.0 (1.0, 5.0) mg/l, respectively.
Among patients with PsA (N = 96), median (Q1, Q3) age was 55 (45, 63) years and 58.3% were female (Table 3). Overall, 45.8% (n = 44) of patients were IFX-naive, 49.0% (n = 47) were IFX-switched, and 5.2% (n = 5) had other treatment history. At baseline, mean (± SD) DAS28 scores were 3.4 (± 1.5) and 2.4 (± 0.9) for IFX-naive and IFX-switched patients, respectively; median (Q1, Q3) baseline CRP concentrations were 3.1 (1.0, 9.4) and 2.0 (1.0, 5.0) mg/l, respectively.
Overall, 80.2% (n = 77) of all patients with PsA were already on CT-P13 at inclusion, for a mean (± SD) duration of 12.0 (± 9.9) months. Among these patients, mean (± SD) DAS28 scores were 4.0 (± 1.1) and 2.4 (± 1.0) for IFX-naive and IFX-switched patients, respectively; median (Q1, Q3) CRP concentrations were 4.7 (2.0, 11.6) and 2.0 (0.9, 3.0) mg/l, respectively.
Ct-P13 Treatment Evolution and PersistenceAcross indications (RA, AS and PsA, respectively), 54.9% (78/142), 61.1% (251/411), and 68.8% (66/96) of patients completed the study according to protocol, and 45.1% (64/142), 38.9% (160/411), and 31.3% (30/96), were prematurely withdrawn from the study (Table S4). Of those who were prematurely withdrawn from the study and with available data, most discontinued the study because of permanent treatment discontinuation (RA: 89.1% [57/64]; AS: 84.7% [133/157]; PsA: 85.7% [24/28]), mainly because of treatment failure (RA: 64.9%; AS: 63.6%; PsA: 62.5%) and intolerance (RA: 24.6%; AS: 12.1%; PsA: 29.2%). When CT-P13 was stopped, most patients switched to another IFX treatment (IFX originator or Remsima) or biotherapy (RA: 67.9%; AS: 73.6%; PsA: 69.6%).
Estimated rates of CT-P13 treatment persistence among all patients with rheumatic diseases were 73.8% (95% CI 69.0%, 79.0) at M12 (n = 568) and 60.8% (95% CI 56.0%, 66.0%) at M24 (n = 504) after CT-P13 initiation. Treatment persistence at M24 after CT-P13 initiation was 67.4% (95% CI 60.9%, 74.7%) for IFX-switched patients (n = 258) and 52.1% (95% CI 45.1%, 60.1%) for IFX-naive patients (n = 221).
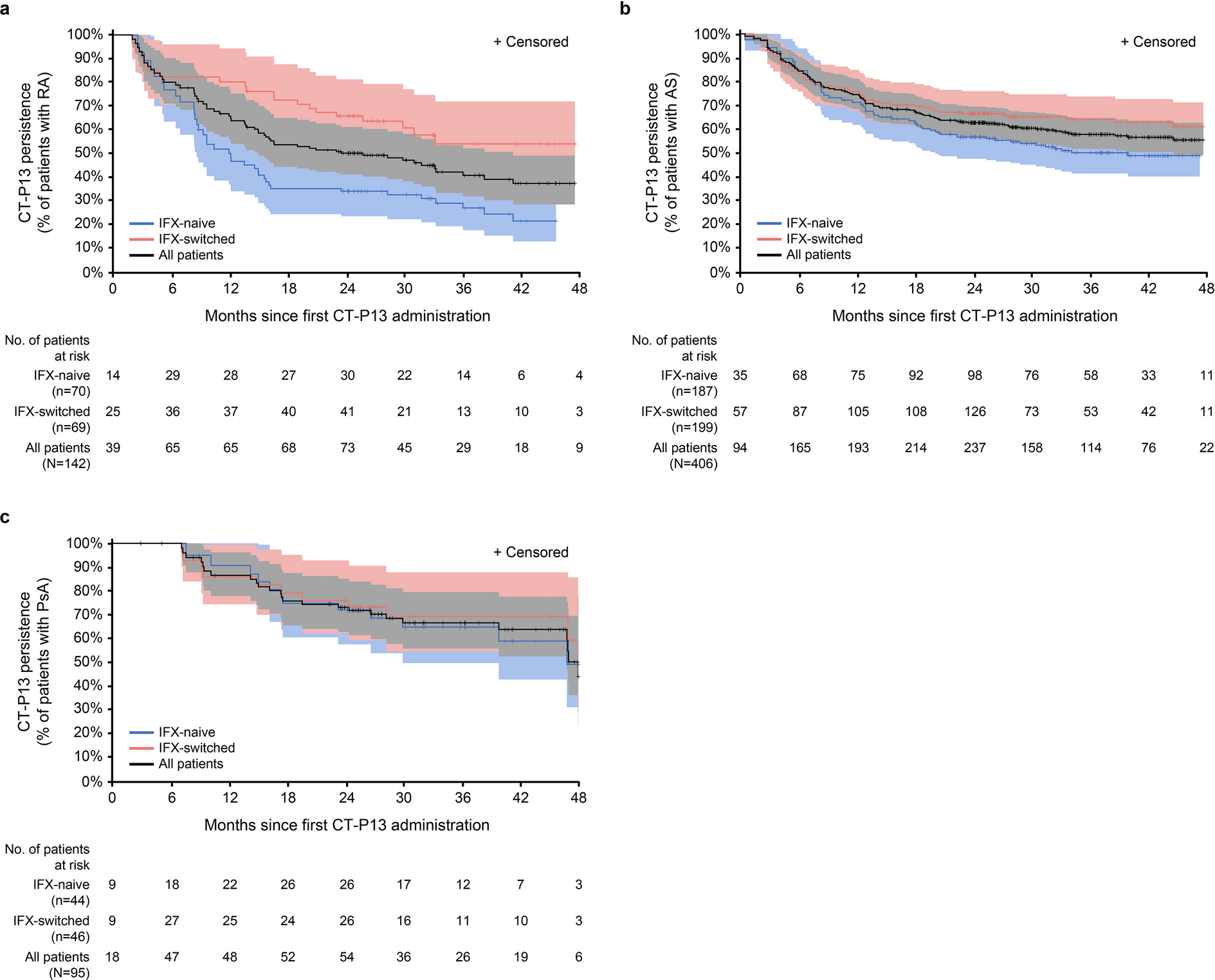
For patients with RA, estimated rates of CT-P13 treatment persistence at M12 and M24 after CT-P13 initiation were 65.4% (95% CI: 55.6%, 76.9%) and 49.6% (40.4%, 60.8%), respectively (Fig. 1a). Treatment persistence at M24 was 65.4% (95% CI: 52.8%, 81.0%) for IFX-switched patients and 33.3% (22.7%, 49.1%) for IFX-naive patients (Fig. 1a). Overall, 43.0% (61/142) of patients permanently discontinued CT-P13, including 52.9% (37/70) and 34.8% (24/69) in the IFX-naive and IFX-switched groups, respectively (Fig. S2a), mainly because of treatment failure according to physician’s assessment (IFX-naive: 38.6% [27/70]; IFX-switched: 18.8% [13/69]) and intolerance (IFX-naive: 12.9% [9/70]; IFX-switched: 8.7% [6/69]) (Fig. S2b). Of those who permanently discontinued CT-P13 and with available data (N = 60), 70% (n = 42) switched to another treatment (Fig. S2c), including a switch back to IFX originator (21.4% [9/42]) or switch to another IFX biosimilar (SB2; 4.8% [2/42]), non-IFX TNF inhibitor (TNFi; 7.1% [3/42]), or treatment/mechanism of action (66.7% [28/42]).
Fig. 1
Kaplan-Meier curves of CT-P13 treatment persistence in patients with RA (a), AS (b) and PsA (c)a. aPatients who were already on CT-P13 at study inclusion were not at risk of treatment failure before entering the study (immortal time). Therefore, immortal time bias was addressed using a Kaplan-Meier method with left truncation and right censoring to analyze time to treatment failure. AS ankylosing spondylitis; IFX-naive patients who were naive to IFX at the time of CT-P13 initiation; IFX-switched patients who switched from IFX originator or another IFX biosimilar to CT-P13; PsA psoriatic arthritis; RA rheumatoid arthritis
For patients with AS, estimated rates of CT-P13 treatment persistence at M12 and M24 after CT-P13 initiation were 74.5% (95% CI 68.4%, 81.2%) and 62.7% (56.6%, 69.5%), respectively (Fig. 1b). Treatment persistence at M24 was 66.5% (95% CI 58.3%, 76.0%) for IFX-switched patients and 56.6% (47.6%, 67.4%) for IFX-naive patients (Fig. 1b). Overall, 33.1% (136/411) of patients permanently discontinued CT-P13, including 37.0% (70/189) and 29.9% (60/201) in the IFX-naive and IFX-switched groups, respectively (Fig. S3a), mainly because of treatment failure according to physician’s assessment (IFX-naive: 23.3% [44/189]; IFX-switched: 18.4% [37/201]) and intolerance (IFX-naive: 5.3% [10/189]; IFX-switched: 3.0% [6/201]) (Fig. S3b). Of those who permanently discontinued CT-P13 and with available data (N = 132), 73.5% (n = 97) switched to another treatment (Fig. S3c), including a switch back to IFX originator (29.9% [29/97]), or switch to another IFX biosimilar (SB2; 12.4% [12/97]), non-IFX TNFi (20.6% [20/97]), or treatment/mechanism of action (37.1% [36/97]).
For patients with PsA, estimated rates of CT-P13 treatment persistence at M12 and M24 after CT-P13 initiation were 86.5% (95% CI 77.8%, 96.2%) and 73.0% (62.7%, 85.1%), respectively (Fig. 1c). Treatment persistence at M24 was 75.9% (95% CI 62.2%, 92.8%) for IFX-switched patients and 72.0% (57.5%, 90.1%) for IFX-naive patients (Fig. 1c). Overall, 29.2% (28/96) of patients permanently discontinued CT-P13, including 27.3% (12/44) and 29.8% (14/47) in the IFX-naive and IFX-switched groups, respectively (Fig. S4a), mainly because of treatment failure according to physician’s assessment (IFX-naive: 22.7% [10/44]; IFX-switched: 12.8% [6/47]) and intolerance (IFX-naive: 4.5% [2/44]; IFX-switched: 10.6% [5/47]) (Fig. S4b). Of those who permanently discontinued CT-P13 and with available data (N = 27), 66.7% (n = 18) switched to another treatment (Fig. S4c), including a switch back to IFX originator (33.3% [6/18]) or switch to a non-IFX TNFi (27.8% [5/18]) or to another treatment/mechanism of action (38.9% [7/18]).
Disease Activity and Biochemical ParametersChanges in disease activity across visits are shown in Figs. 2, 3, and 4 for patients with RA, AS, and PsA, respectively. For patients with RA, mean (± SD) DAS28 and SDAI scores at M0 were 4.8 (± 1.2) and 34.3 (± 17.9), respectively, in the IFX-naive group and 2.6 (± 0.9) and 9.8 (± 7.5), respectively, in the IFX-switched group (Fig. 2a, b). In IFX-naive patients, mean DAS28 score decreased from M0 to M6 and then remained relatively stable until M24 (3.5 ± 1.3); mean SDAI decreased over time until M24 (17.0 ± 15.8). In IFX-switched patients, both mean DAS28 and SDAI scores remained stable across visits (M24: 2.4 ± 0.9 and 6.4 ± 7.9, respectively).
Fig. 2
Changes in DAS28 (a) and SDAI (b) scores and in CRP concentrations (c) across visits for patients with RA treated with CT-P13. CRP C-reactive protein; DAS28 disease activity score-28; IFX infliximab; RA rheumatoid arthritis; SD standard deviation; SDAI simplified disease activity index
Fig. 3
Changes in BASDAI (a) and BASFI (b) scores and CRP concentration (c) across visits for patients with AS treated with CT-P13. AS ankylosing spondylitis; CRP C-reactive protein; BASDAI Bath Ankylosing Spondylitis Disease Activity Index; BASFI Bath Ankylosing Spondylitis Functional Index; IFX infliximab; SD standard deviation
Fig. 4
Changes in DAS28 score (a) and CRP concentration (b) across visits for patients with PsA treated with CT-P13. CRP C-reactive protein; DAS28 disease activity score-28; IFX infliximab; PsA psoriatic arthritis; SD standard deviation
For patients with AS, mean BASDAI and BASFI scores at M0 were 5.6 (± 1.9) and 5.2 (± 2.3), respectively, in the IFX-naive group and 2.7 (± 2.1) and 3.2 (± 2.5), respectively, in the IFX-switched group (Fig. 3a, b). In IFX-naive patients, mean BASDAI score decreased over time until M24 (3.2 ± 2.2); mean BASFI decreased from M0 to M6 and then remained relatively stable until M24 (3.4 ± 2.4). In IFX-switched patients, both mean BASDAI and BASFI scores remained stable across visits (M24: 2.7 ± 1.8 and 3.4 ± 2.7, respectively).
For patients with PsA, mean DAS28 score at M0 was 4.2 (± 1.1) and 2.2 (± 0.9) in the IFX-naive and IFX-switched groups, respectively (Fig. 4a). In IFX-naive patients, mean DAS28 score decreased from M0 to M6 and then remained relatively stable until M24 (2.8 ± 1.6); DAS28 score remained stable across visits for IFX-switched patients (M24: 2.9 ± 1.0).
Regardless of the indication, CRP concentration decreased from M0 to the end of follow-up in IFX-naive patients. Conversely, there was no change in CRP concentration throughout follow-up in IFX-switched patients (Figs. 2c, 3c and 4b).
SafetyAn overview of safety by indication and treatment group is provided in Table 4. Overall, 56.4% (366/649) of patients reported at least one AE, 11.9% (77/649) reported SAEs, and 24.5% (159/649) reported AESIs with possible relationship to CT-P13. The incidences of AEs and SAEs were 58.1% and 10.6%, respectively, in the IFX-naive group and 55.8% and 12.6%, respectively, in the IFX-switched group. The most frequently reported specific AEs were infections (severe infections, tuberculosis, opportunistic infections, hepatitis B) in 7.7% (11/142), 4.9% (20/411), and 5.2% (5/96) of patients with RA, AS, and PsA, respectively, and adverse reactions due to perfusion (acute and delayed hypersensitivity reactions) in 3.5% (5/142), 2.9% (12/411), and 1.0% (1/96) of patients, respectively.
Table 4 Safety overview for patients with RA, AS or PsA treated with CT-P13Infection AESI of herpes zoster were reported in 1.4% (2/142), 0.2% (1/411), and 0% (0/96) of patients with RA, AS, and PsA, respectively. Congestive heart failure AESIs were reported in 0.7% (1/142), 0% (0/411), and 0% (0/96) of patients with RA, AS, and PsA, respectively. Malignant pathology, leukemia, and lymphoma AESIs were reported in 2.1% (3/142), 0.7% (3/411), and 0% (0/96) of patients with RA, AS, and PsA, respectively. Thrombotic events AESI were reported in 0% (0/70), 0.7% (3/411), and 0% (0/96) of patients with RA, AS, and PsA, respectively. COVID-19 infection was reported in 0.2% (1/411) of patients with AS and in 0% of patients with RA and PsA.
In general, concomitant corticosteroid therapy decreased with time in patients with RA (Fig. S5), especially in naïve patients (from 45% at M6 to 30% at M12), while it remained relatively stable in switched patients (22% at M6 and 17% at M24). In patients with AS, concomitant corticosteroid therapy was maintained (14% at M6 and M24 in naive patients and 8% and 7%, respectively, in switched patients). In patients with PsA, corticosteroid therapy remained stable in naïve patients (14% at M6 and 11% at M24) but decreased with time in switched patients (16% at M6 and 6% at M24).
Comments (0)