
Remember me
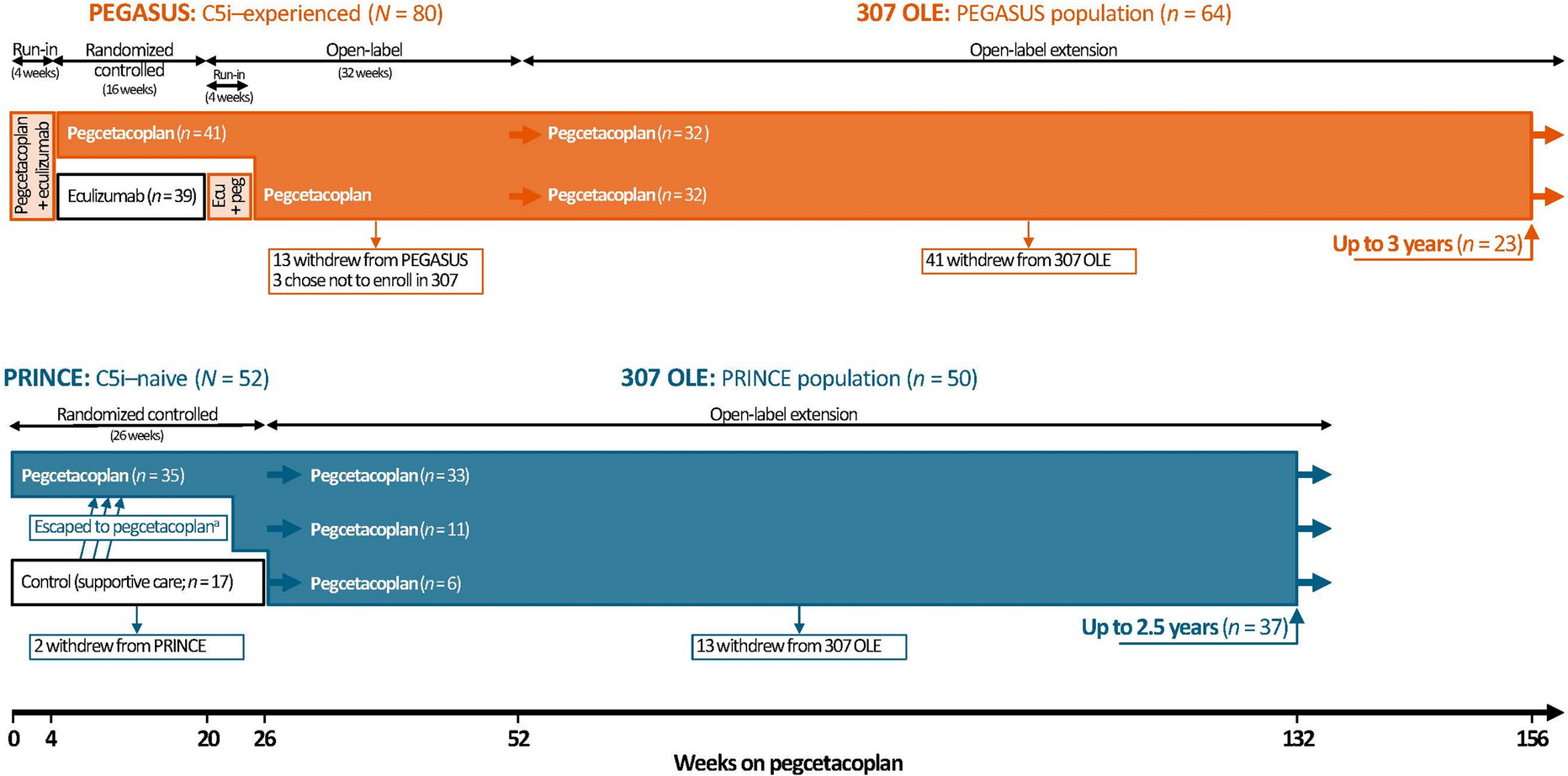
Study designs of pegcetacoplan randomized controlled trials (PEGASUS and PRINCE) and open-label extension (307 OLE) have been published [14,15,16,17]. Comparator groups started receiving pegcetacoplan at different times in PEGASUS (week 20) and PRINCE (307 OLE entry or earlier), which resulted in patients having differing durations of pegcetacoplan treatment at given time points in each trial (Fig. 1). This integrated analysis of PEGASUS, PRINCE, and 307 OLE established new baselines for all patients, at pegcetacoplan initiation for efficacy measures and beginning of pegcetacoplan monotherapy for safety evaluation.
Fig. 1
Study designs of the PEGASUS, PRINCE, and 307 OLE clinical trials of pegcetacoplan for PNH. aPatients in the PRINCE control (supportive care) arm could escape to the pegcetacoplan arm before the end of the 26 weeks if they experienced a qualifying event of anemia or thrombosis. C5i C5 inhibitor, ecu eculizumab, OLE open-label extension, peg pegcetacoplan, PNH paroxysmal nocturnal hemoglobinuria
Ethical ApprovalAll study protocols were designed and monitored in accordance with the ethical principles of Good Clinical Practice and the Declaration of Helsinki. Trials were approved by an institutional review board or independent ethics committee at each center (Table S1); the master ethics committees were Advarra (PEGASUS) and Comite de Etica en Investigacion Biomedica IPS Centro Medico Julian Coronel (PRINCE). All patients provided written informed consent before participation. The trials were funded by Apellis Pharmaceuticals and Sobi (Swedish Orphan Biovitrum AB), who provided the investigative medications. The trials were registered under ClinicalTrials.gov NCT03500549 (PEGASUS), NCT04085601 (PRINCE), and NCT03531255 (307 OLE). The datasets generated and/or analyzed are available from the corresponding author on reasonable request.
ParticipantsThis integrated analysis included all patients aged ≥ 18 years with a confirmed diagnosis of PNH by high-sensitivity flow cytometry who were enrolled in PEGASUS or PRINCE and received ≥ 1 dose(s) of pegcetacoplan in PEGASUS, PRINCE, or 307 OLE. Patients in PEGASUS had hemoglobin < 10.5 g/dL despite receiving eculizumab [14, 15]. Patients in PRINCE had not received a C5 inhibitor in the previous 3 months and had hemoglobin concentrations less than the lower limit of normal (LLN; male, < 13.6 g/dL; female, < 12.0 g/dL) [16]. Patients completing PEGASUS or PRINCE could enter the 307 OLE if both the patient and physician wanted to continue/initiate pegcetacoplan treatment because of potential clinical benefit and acceptable tolerability.
TreatmentsPEGASUS (N = 80) was a 48-week trial that included a 4-week run-in period of concomitant eculizumab and subcutaneous (SC) infusions of pegcetacoplan (1080 mg twice weekly), a 16-week randomized controlled period of pegcetacoplan (n = 41) or eculizumab (n = 39) monotherapy, and a 32-week open-label period of continued pegcetacoplan or 4 weeks of concomitant eculizumab and pegcetacoplan followed by 28 weeks of pegcetacoplan monotherapy for those randomized to eculizumab. In PRINCE, C5 inhibitor-naive patients (N = 53) were randomized 2:1 to SC infusions of pegcetacoplan 1080 mg twice weekly (n = 35) or control (continued supportive care excluding complement inhibitors; n = 18) for 26 weeks [16]. One patient randomized to control died of respiratory failure and septic shock before PRINCE completion and did not receive pegcetacoplan; therefore, data from this patient were excluded from this analysis. Patients in the supportive care arm could escape to pegcetacoplan treatment if their hemoglobin decreased from baseline by ≥ 2 g/dL or if they experienced a qualifying event of anemia or thrombosis.
Patients who completed PEGASUS or PRINCE could then enter 307 OLE and continue SC infusions of pegcetacoplan [17]. The planned duration of 307 OLE is 4 years, with allowed transition to commercial pegcetacoplan in regions where it becomes available. The data cutoff date for this analysis was January 31, 2023.
Assessments and OutcomesPatient demographics and clinical characteristics were recorded at PEGASUS and PRINCE entry. In this integrated analysis, the efficacy and safety data over time from PEGASUS, PRINCE, and 307 OLE were assessed from newly defined baselines to week 132 (PRINCE) or week 156 (PEGASUS).
Longitudinal efficacy measures included hemoglobin and LDH concentrations, absolute reticulocyte counts (ARCs), indirect bilirubin concentrations, and Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue scores. Efficacy baseline measures were determined at the time of the first pegcetacoplan dose. For PEGASUS and PRINCE patients randomized to pegcetacoplan, baseline values were the average of up to 4 measurements taken within up to 12 weeks before pegcetacoplan initiation. For PEGASUS patients randomized to eculizumab, baseline values were the last measurement before pegcetacoplan initiation in the second run-in period at week 17 (or earlier, if week-17 measurement missing). For PRINCE patients randomized to control, baseline values were the last measurement before receiving the first pegcetacoplan dose; these were adjusted further if the last measurement was within 28 days after a blood transfusion by taking the average of local and central laboratory concentrations within 28 days before pegcetacoplan initiation. Patients who had a transfusion were excluded from hemoglobin concentration analysis for 60 days after the transfusion.
Efficacy measures were reported at the newly defined baseline and at weeks 2, 4, 6, 8, 10, 12, 16, 20, 24, and every 12 weeks thereafter up to 132 weeks for PRINCE patients and 156 weeks for PEGASUS patients. Normal ranges for laboratory measures were defined by the central laboratory. Local laboratory values were adjusted to the normal range of the central laboratory. Scores for FACIT-Fatigue range from 0 to 52, with higher scores indicating less fatigue; a score of 43.6 was previously reported as the general population norm [18,19,20]. Treatment adherence was defined as the total number of pegcetacoplan injections from the first dose to week 132 (PRINCE) or week 156 (PEGASUS), divided by the total number of expected injections during that time, adjusted to reflect the actual dosing frequency.
Safety outcomes, including annual transfusion avoidance (i.e., not requiring transfusion during pegcetacoplan monotherapy), were evaluated from the start of pegcetacoplan monotherapy only. Investigators’ transfusion decisions were informed by standards of care, local practice guidelines, and patient needs. Adverse events and treatment-emergent adverse events (TEAEs) were classified by System Organ Class and Preferred Term (Medical Dictionary for Regulatory Activities Version 23.0). TEAEs included adverse events starting (or worsening in severity if starting earlier) on or after the first dose of pegcetacoplan monotherapy and excluded events occurring > 8 weeks following the final dose. Pegcetacoplan-relatedness and severity were determined by investigators.
After receiving training, patients self-administered pegcetacoplan subcutaneously using an ambulatory syringe pump and were instructed to notify investigators or study personnel of injection site reactions or self-administration issues, which were recorded post hoc as adverse events (see Sharma et al. for methodology [21]). For the current analysis, events of clinically significant and laboratory-confirmed breakthrough hemolysis were defined post hoc as investigator-reported TEAEs of hemolysis with all of the following: LDH > 2 × ULN, any prior LDH < 1.5 × ULN, and a ≥ 2-g/dL hemoglobin decline from the median hemoglobin concentration of all prior measurements while on pegcetacoplan. Patients with acute hemolysis (i.e., LDH > 2 × ULN and ≥ 1 new or worsening sign/symptom of hemolysis warranting acute intervention) transitioned to a substudy where they could receive intensive pegcetacoplan dosing. For details of intensive dosing, refer to Griffin et al. and Peffault de Latour et al. [22, 23]. The current analysis included data related to the incident acute hemolysis event but excluded data after the start of intensive dosing.
Statistical AnalysesEfficacy and safety analyses were performed in the intention-to-treat population, which included all patients who received ≥ 1 dose of pegcetacoplan. Patient characteristics at PRINCE or PEGASUS entry, as well as hemoglobin, LDH, ARC, indirect bilirubin, and FACIT-Fatigue values at the newly defined baseline and over time were presented by parent study population [14, 16]. Red blood cell transfusion avoidance was evaluated for each population using a Kaplan–Meier analysis. In the long-term safety analysis, safety events, including post hoc injection site reactions and clinically significant breakthrough hemolysis, were tabulated from pegcetacoplan monotherapy initiation through 2.5 (PRINCE) and 3 (PEGASUS) years. Efficacy and safety outcomes were summarized using descriptive statistics.
Comments (0)