
Remember me
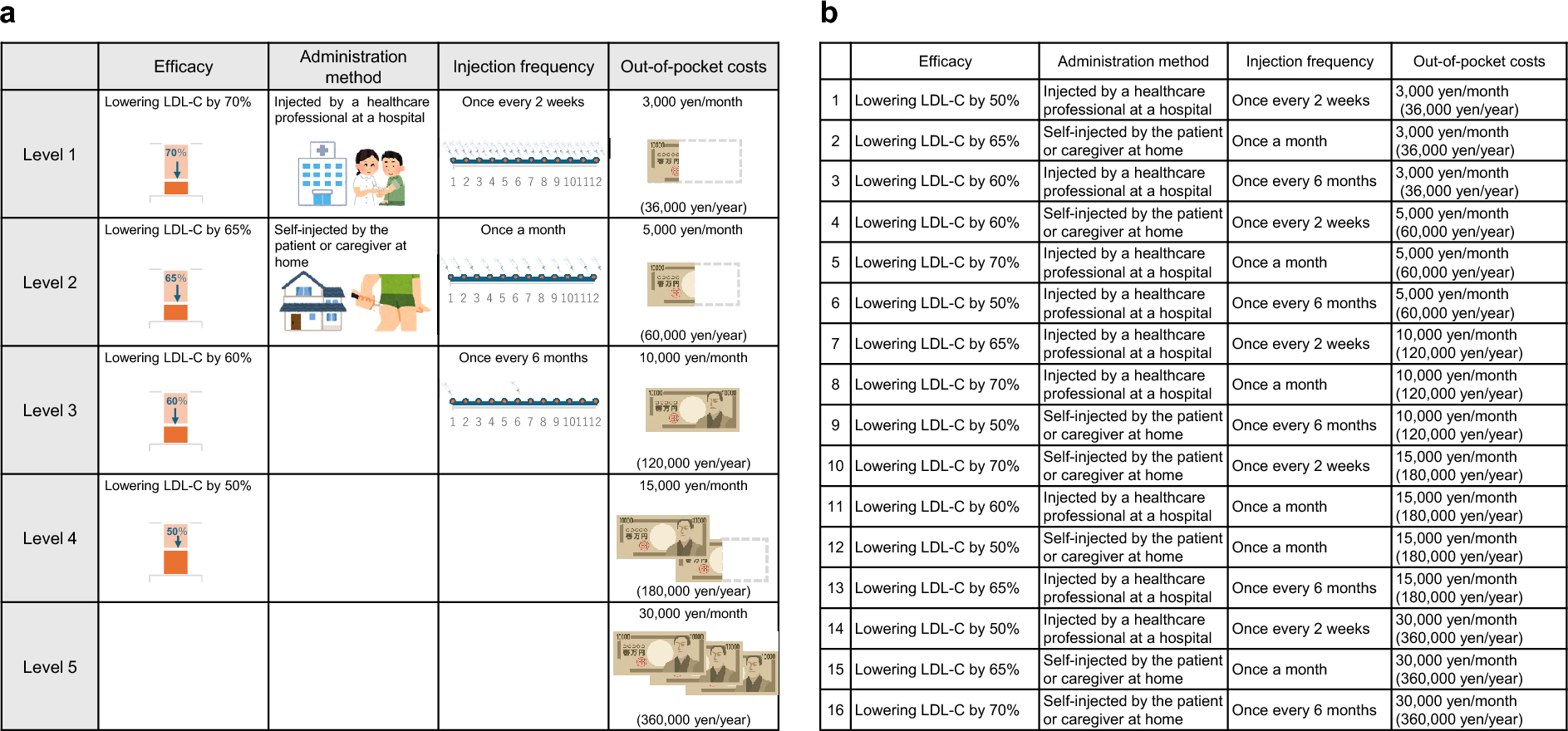
We conducted a cross-sectional survey using a DCE to assess the real-world patient preferences for injectable LLTs in Japan. We based our design on the two currently available injectable LLTs in Japan: evolocumab and inclisiran [6, 15,16,17,18]. Candidate attributes were identified through a structured review of product labels, clinical guidelines, published preference studies, and consultation with three lipid specialists. Four attributes (out-of-pocket costs, injection frequency, mode of administration, and expected LDL-C reduction) were selected based on clinical relevance and policy salience. Information on efficacy and injection frequency levels were derived from two clinical trials (ORION-15 [15] and YUKAWA-2 [16]) and a clinical consensus statement from Europe [18]. Administration method levels were defined according to their approved uses in Japan. The administration method encompasses two aspects: the location of administration and the individual responsible for administering the LLT. This approach was taken to minimize the number of attributes and decrease the response burden. Out-of-pocket cost was based on the official drug pricing in Japan. The attribute of side effects was excluded from the DCE because a previous study showed that injectable LLTs in Japan had similar side effect profiles [15, 19, 20]. Two to four mutually exclusive levels were assigned to each attribute, reflecting the range encountered in routine practice. Sixteen drug profiles were then established using a D-optimal design based on these attributes and levels (Fig. 1b).
Fig. 1
Discrete choice experiment levels and profiles. a Attributes and levels in the discrete choice experiment. b Sixteen drug profiles. USD equivalent of out-of-pocket cost levels: 19 USD/month (231 USD/year), 32 USD/month (386 USD/year), 64 USD/month (772 USD/year), 96 USD/month (1158 USD/year), and 193 USD/month (2315 USD/year). LDL-C low-density lipoprotein cholesterol, USD US dollar
Validation of Survey ContentsTo ensure that the attributes and their levels were important and relevant to patient preferences for injectable LLTs, we conducted semi-structured qualitative interviews with eight individuals (five in secondary prevention and three in primary prevention) prior to fielding the DCE. In the interview, the patients were first asked to identify the factors they prioritized when selecting an injectable LLT. They were then presented with the proposed attributes (efficacy, administration method, injection frequency, and out-of-pocket costs) and their respective levels and asked to evaluate whether these attributes and levels were important for their decision-making regarding injectable LLTs. Participants also completed draft choice tasks and provided feedback on wording, relevance, and plausibility. Their input informed minor revisions to phrasing and level boundaries, after which the final questionnaire was launched online (Fig. 1). Educational materials derived from previous studies [6, 17, 21, 22] were also confirmed through the interviews (Fig. S1).
The process of the survey development is illustrated in Fig. S2.
DCE Online SurveySurvey FlowAfter validation of the survey contents through the qualitative interviews, we conducted the DCE online survey. Flow of the DCE online survey was illustrated in Fig. S3a. First, respondents answered an initial set of DCE questions. Next, they were presented with educational materials on dyslipidemia (DL) and ASCVD risk (Fig. S1). Finally, a second set of DCE questions was presented.
Training for DCE QuestionsTo assist respondents in completing the DCE tasks, training questions were established before the first DCE block. Each attribute was explained to the respondents (Fig. S4), and a DCE question was demonstrated. After training, the respondents were asked whether they understood the meaning of each attribute and how to answer the DCE. If the respondents indicated a lack of understanding, the training could be repeated up to three times.
Design of the DCE QuestionsIn the DCE tasks, respondents were presented with two profiles per question (i.e., task) (Fig. S3b). The profile combinations (labeled “Treatment P” and “Treatment Q” in Fig. S3b) were randomly selected from the 16 predefined profiles (Fig. 1b), resulting in a total of 8 tasks per respondent in each DCE block. The task order was randomized for each respondent in the first DCE block. In the second DCE block, the same profile pairs were maintained; however, their presentation positions (left or right, as Treatment P or Treatment Q) and the order of the profile pairs were randomized for each respondent.
Contents of Educational MaterialsThe educational materials comprised five panels designed to assess the impact of education on ASCVD risk awareness and patient preferences for injectable LLTs. After completing the first block of discrete choice questions, respondents were shown a five-panel educational module presented in slideshow format (Fig. S1).
Panel 1 summarized the epidemiology and pathophysiology of DL in Japan.
Panel 2 highlighted the 3-year recurrence risk of cerebro-cardiovascular events in patients with a history of myocardial infarction (MI).
Panel 3 explained the relationship between LDL-C levels and ASCVD risk, using icon arrays to illustrate symptoms.
Panel 4 reviewed guideline LDL-C targets and residual cardiovascular risk under standard therapy.
Panel 5 described administration techniques, injection devices, and frequency.
Each panel combined plain-language text with graphics and was displayed for a minimum of 5 s; respondents could not proceed until this interval had elapsed. After viewing all panels, participants were allowed to return to the beginning and review the content again. Immediately thereafter, they completed a second block of discrete choice questions, allowing us to quantify changes in stated preferences attributable to the educational intervention.
SettingThe DCE online survey was conducted from January 29 to February 29, 2024. Potential respondents were selected from Japan nationwide using the Rakuten Insight Disease Panel, managed by Rakuten Insight Inc. This panel comprises a large cohort of individuals diagnosed with various medical conditions who have consented to participate in research studies. The panel is designed to facilitate academic, clinical, and marketing research by providing access to a diverse population of patients with different disease conditions. The panel was used in several studies to generate real-world evidence [23,24,25,26,27].
Survey RespondentsIn this study, respondents aged ≥ 18 years with at least one diagnosis of DL, hypercholesterolemia, or familial hypercholesterolemia and currently receiving statin treatment were included. Respondents diagnosed with dementia or malignant tumors were excluded from the survey. The respondents were classified into two groups: a secondary prevention group (with a history of at least one MI, angina pectoris, or cerebral infarction) and a primary prevention group (with no history of MI, angina, or cerebral infarction but with DL and diabetes) (Fig. 2). Since real-world evidence showed that approximately 80% of patients receiving injectable LLTs were in secondary prevention [28], a larger sample size of secondary prevention patients than those of primary prevention patients was set in this study.
Fig. 2
Participant selection. aSecondary prevention group included eligible respondents with ≥ 1 event of myocardial infarction, angina pectoris, or cerebral infarction and those with ≥ 1 diagnosis of dyslipidemia, hypercholesterolemia, or familial hypercholesterolemia. After completing the data collection for 491 patients, additional patients using evolocumab were included, increasing the total to 500 patients. bPrimary prevention group included eligible respondents without myocardial infarction, angina pectoris, or cerebral infarction but with dyslipidemia and diabetes. cThe exclusion criteria were: participants who responded “I do not understand” three times after being shown the discrete choice experiment (DCE) explanatory questions; participants who only selected profiles displayed on the right or left side in both the first and second DCE; participants whose response times (time from starting to finishing the response) were outside the range of first quartile − 1.5 × interquartile range to third quartile + 1.5 × interquartile range
EndpointsThe primary endpoints were the RI and relative preference weight in the secondary prevention group. In this study, the RI represents the quantitative trade-offs among the attributes of injectable LLTs (i.e., efficacy, administration method, injection frequency, and out-of-pocket costs) as considered in patients’ treatment selection. The preference weights reflect relative preferences, such that differences between attribute levels (e.g., LDL-C reduction of 70%, 65%, 60%, or 50%) indicate the magnitude of change in patient preference across those levels. The secondary endpoints were the RIs and relative preference weights in the secondary prevention subpopulations, in the secondary prevention group after viewing the educational materials, and in the primary prevention group.
Data AnalysisData CleaningThe collected survey data were cleaned based on the reliability of responses to the survey questions.
Respondents were excluded if they were unable to understand how to answer the three rounds of DCE training questions. Those who consistently selected the same position across all eight DCE tasks (e.g., always choosing “Treatment P”) were also excluded. In addition, respondents who completed the DCE online survey in an implausibly short or long time (defined as falling outside the range of the first quartile − 1.5 interquartile range [IQR] or third quartile + 1.5 IQR) were excluded as outliers. The DCE online survey was designed to collect no missing data.
Determination of Sample SizeThe sample size was determined based on the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) report, which recommended a sample size of 300 respondents for DCEs [29]. The sample size for the primary endpoint in this study exceeded that recommended in the ISPOR report.
Statistical AnalysisWe conducted a conditional logistic regression analysis using the preference (selected or not selected) for each drug profile in the DCE question as the outcome variable and the effect-coded level of each profile as the explanatory variable [30]. A variable indicating the combination of two profiles was included as a layer in the regression model. The obtained partial regression coefficients were used as relative preference weights. The relative preference weights for the omitted levels in the regression model were calculated as the negative sum of all other levels in each attribute, and their 95% confidence intervals were determined using the delta method [31, 32]. The RI was calculated based on the range of preference weights for each attribute.
For subgroup analyses, the secondary prevention group was categorized by age (< 65 or ≥ 65 years), employment status (employed or unemployed), annual household income (< 4, 4 to < 8, or ≥ 8 million yen; approximately < 25,775, 25,775 to < 51,550, or ≥ 51,550 US dollars [USD]), and ASCVD history (CAD only [MI and angina pectoris], cerebral infarction only, or CAD combined with cerebral infarction). The exchange rate between yen and USD was determined at the time of writing as 152 yen per USD.
Statistical analyses were performed using BellCurve for Excel version 4.05 (Social Survey Research Information Co., Ltd., Tokyo, Japan).
Ethical ApprovalThis study was approved by the Kitamachi Clinic Ethical Review Committee of the Medical Corporation Tokeikai (approval number for qualitative interviews and DCE online survey: BGQ09833; approval date for conducting qualitative interviews: November 15, 2023; approval date for conducting DCE online survey: January 17, 2024). The study complied with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects (Ministry of Health, Labour and Welfare of Japan). All respondents provided consent to participate before data collection.
Comments (0)