Data Source
This was a retrospective open cohort study using data from Discover, a real-world EHR database containing linked primary and secondary health records covering 2.7 million people across 365 primary care practices in North West London, UK [18]. Primary care records (Read codes) are available from 1 January 2004 and secondary care records, comprising International Classification of Diseases version 10 codes for hospital visits, outpatient appointments and emergency room visits, and OPCS-4 codes for procedures, are available from 1 January 2015. Discover has a similar age and sex distribution to the UK general population, but greater ethnic diversity [19].
Study Design and Population
The study period was 1 January 2007 to 31 December 2019, to exclude healthcare data from during the COVID-19 pandemic. Index date was the date of the first eligible BMI measurement during the study period and end date was the earliest of the following: date of death, date of transfer-out from healthcare practice, 8 years of follow-up or end of the study period (Fig. S1).
For inclusion in the main analysis, individuals were required to be 18 years or older, have a BMI of at least 25 kg/m2 at index date, at least one additional BMI measurement after the index date and have no evidence of intentional weight loss at any time before or during the study period. Evidence of intentional weight loss was established using clinical codes for weight-loss diet, weight-loss drug prescription, or referral to a dietician or for bariatric surgery. Individuals were required to have been registered in the Discover database for at least 6 months before index date so that sufficient baseline data were available. Individuals were divided into four groups based on BMI at index date according to the World Health Organization classification [20]: overweight (25 to < 30 kg/m2), obesity class I (30 to < 35 kg/m2), obesity class II (35 to < 40 kg/m2) and obesity class III (≥ 40 kg/m2).
Sex was captured as recorded in an individual’s EHR; individuals with missing or indeterminate sex were excluded. Other exclusion criteria were: no general practitioner or nurse practitioner visits for more than 5 years during the study period (which may indicate that an individual has left their healthcare practice), or conditions/events that could result in weight loss or gain and confound the study results, namely malignant cancer diagnosis during follow-up or up to 5 years before index date, thyroid disorder any time before index date or during follow-up, a pregnancy code up to 1 year before index date or any time during follow-up, or limb amputation during follow-up. Individuals with more than 3 years between direct BMI measurements were censored at their last recorded measurement, for consistency with a previous longitudinal analysis of BMI changes [14].
Analyses and OutcomesBMI Progression
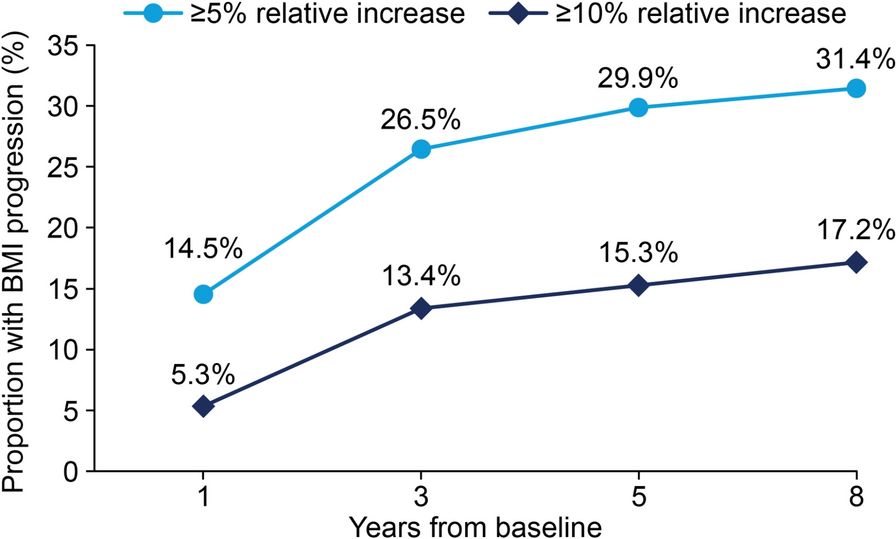
The main analysis assessed the proportion of individuals with BMI progression (i.e. increase) of ≥ 5% and ≥ 10%, at years 1, 3, 5 and 8 post-baseline. BMI measurements were recorded at the end of each annual analysis period using the measurement closest to, but within 3 months of, the anniversary date for study entry. BMI for each year was captured by assessing direct measurements, or otherwise calculated from measurements of weight and height, where possible, but if these were not available, BMI estimates were calculated assuming a linear relationship between two recorded measurements. The records were selected based on: (1) closest proximity to the time period with the missing measurement; (2) next closest measurement that was at least ± 60 days from the first.
BMI progression was further characterized in subgroups based on demographic factors and the presence of ORCs in EHRs. Demographic groups were based on age (18–29 years and 10-year age bands from 30–39 years up to 70–79 years); sex (men, women); and ethnicity (Asian, Black, White, Mixed or Other). The 30 ORCs included are shown in Supplementary Material, Table S1. The proportions of individuals with BMI progression in separate subgroups defined by overweight/obesity class plus demographic factors and ORCs were also assessed.
Comparison of Groups With and Without BMI Progression
As a secondary analysis, the development of ORCs, estimates of HCRU and associated costs were assessed in groups with and without BMI progression. For this analysis, individuals were positively ranked within each BMI category by their relative change in BMI between baseline and 8 years post-baseline, with the top 20% of individuals in each BMI category retained, which resulted in the mean increase in BMI within each baseline BMI subgroup being at least 5.0 kg/m2. Individuals were ranked by the degree of progression, with the following subgroups defined: no progression (5% decrease to 5% increase), 5 to < 10% progression and ≥ 10% progression. Individuals with a BMI reduction of 5% or more were not eligible for inclusion. The analysis of individuals with and without BMI progression was carried out in an overall population with overweight or obesity, and in separate overweight and obesity groups.
For assessment of the relationship between extent of BMI progression and development of concomitant conditions, we focused on a subgroup of ORCs, owing to the close link between risk of these conditions and increasing obesity class, and for alignment with the specific ORCs included in previous analyses, which showed that these ORCs tended to be more prevalent in groups with successively higher BMI, increased in prevalence over time, and were often associated with higher costs in successively higher BMI groups [11, 12]. The following ORCs were included: asthma, atherosclerotic cardiovascular disease, back pain, CKD, dyslipidaemia, gastro-oesophageal reflux disease, gout, heart failure, hypertension, knee osteoarthritis, OSA, polycystic ovary syndrome (PCOS), prediabetes, psoriasis, T2D and urinary incontinence. Increases from baseline in the prevalence of ≥ 1, ≥ 2 and ≥ 3 ORCs were also assessed.
Mean annual total direct healthcare costs over 8 years, comprising all costs of primary care (general practitioner or nurse practitioner appointments), inpatient admissions, outpatient appointments, prescriptions and emergency room visits, were also assessed in the BMI progression groups, as were average annual number of HCRU events (primary care appointments, inpatient admissions, outpatient appointments and emergency room visits). Primary care costs were derived from the Personal Social Services Research Unit (2020) [21], and secondary care costs were derived from the Secondary Uses Service, produced by National Health Service (NHS) Digital [22]. Prescription costs were calculated using net ingredient costs obtained from the national report on the net ingredient cost of all prescriptions dispensed in England in 2019 [23]. Costs were adjusted to 2019 costs in pound sterling using UK Consumer Price Index inflation data from the Office for National Statistics.
Statistical Analyses
Baseline characteristics are presented as mean (standard deviation [SD]) for continuous variables, and as number and percentage for categorical variables. The rate of BMI progression overall and by subgroups during each cross-section was measured by the proportion of individuals whose BMI increased from baseline by the prespecified criteria outlined previously. HCRU and costs are presented as means and associated 95% confidence intervals.
Ethical Approval
This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. The study was a retrospective analysis using only secondary de-identified data, and therefore informed consent, consent to publication and approval by an ethics committee were not required. Access to the Discover dataset is managed by Imperial College Health Partners with the North West London Information Governance Committee approving applications (SDRAG). The current analysis was conducted under approved application ID 183, which conferred approval to access and use Discover data.

Comments (0)