Gastric high-grade intraepithelial neoplasia (GHGIN) belongs to EGC that can coexist with aggressive adenocarcinoma according to the definition in the Japanese gastric cancer treatment guidelines, and 25% of patients with GHGIN develop adenocarcinoma within 1 year (Evans and Chandrasekhara 2015; Gotoda 2007). We reviewed 130 cases of multiple EGC and GHGIN and found that the incidence (5.04%) was similar to that previously reported (4.8%-15%) (Isobe et al. 2013; Kato et al. 2013; Kim et al. 2016; Kosaka et al. 1990). The incidence of SMEGC varies according to race and region. The rate calculated in this study is consistent with the 3.8%-9% reported in Southeast Asia (Choi et al. 2011; Zhao et al. 2020; Zhu et al. 2020). Epidemiological studies have shown that SMGC is more likely to occur in elderly men, particularly in those with precancerous lesions, such as atrophic gastritis and severe intestinal metaplasia (Zhao et al. 2020; Nitta et al. 2009; Isozaki et al. 1996; Nam et al. 2018). Otusiji et al. stated that the average age of 76 patients with multiple gastric cancer (MGC) was 63.1 ± 1.6 years old, surpassing the age of patients with solitary gastric cancer (Otsuji et al. 2005). Nam et al. (2018) reviewed 59 patients with SMEGC and found that age ≥ 65 years and the moderate-to-severe endoscopic atrophic gastritis were associated with the formation of synchronous gastric epithelial neoplasia. Isobe et al. (2013) confirmed that elderly men who smoked, drank, or had a family history of gastric cancer were most likely to develop MGC. Our results are consistent with these conclusions. Summarily, it is necessary to classify elderly men with long-term smoking and drinking habits and pathology indicating mucosal atrophy and intestinal metaplasia as a high-risk group for SMEGC. Meticulous and comprehensive endoscopic screening is recommended for this demographic.
We explored the rules of endoscopic morphology and pathological types of the main and minor lesions by analysing the correlation between them to avoid a missed diagnosis of SMEGC. Our study showed that the mean diameter of the main lesion was greater than that of the minor lesion and that the minor lesion kept pace with the enlargement of the main lesion, with a strong positive correlation between the two lesions, as shown in Supplementary Fig. 2 (r = 0.658, p < 0.001). In terms of endoscopic gross type, the correlation analysis of the main and minor lesions showed consistency (kappa = 0.294, p < 0.001), in which the main lesions were dominated by the depressed type and the minor lesions were based on the elevated type. Jung Ho Kim et al. (2016) clarified that the main and minor tumours in 67.6% of cases had the same gross endoscopic type (p < 0.001), which is similar to the results of this study. Correlation analysis of the main and minor lesions in terms of histopathological type and invasion depth indicated consistency (p < 0.001), consistent with the results reported above (Kim et al. 2016).
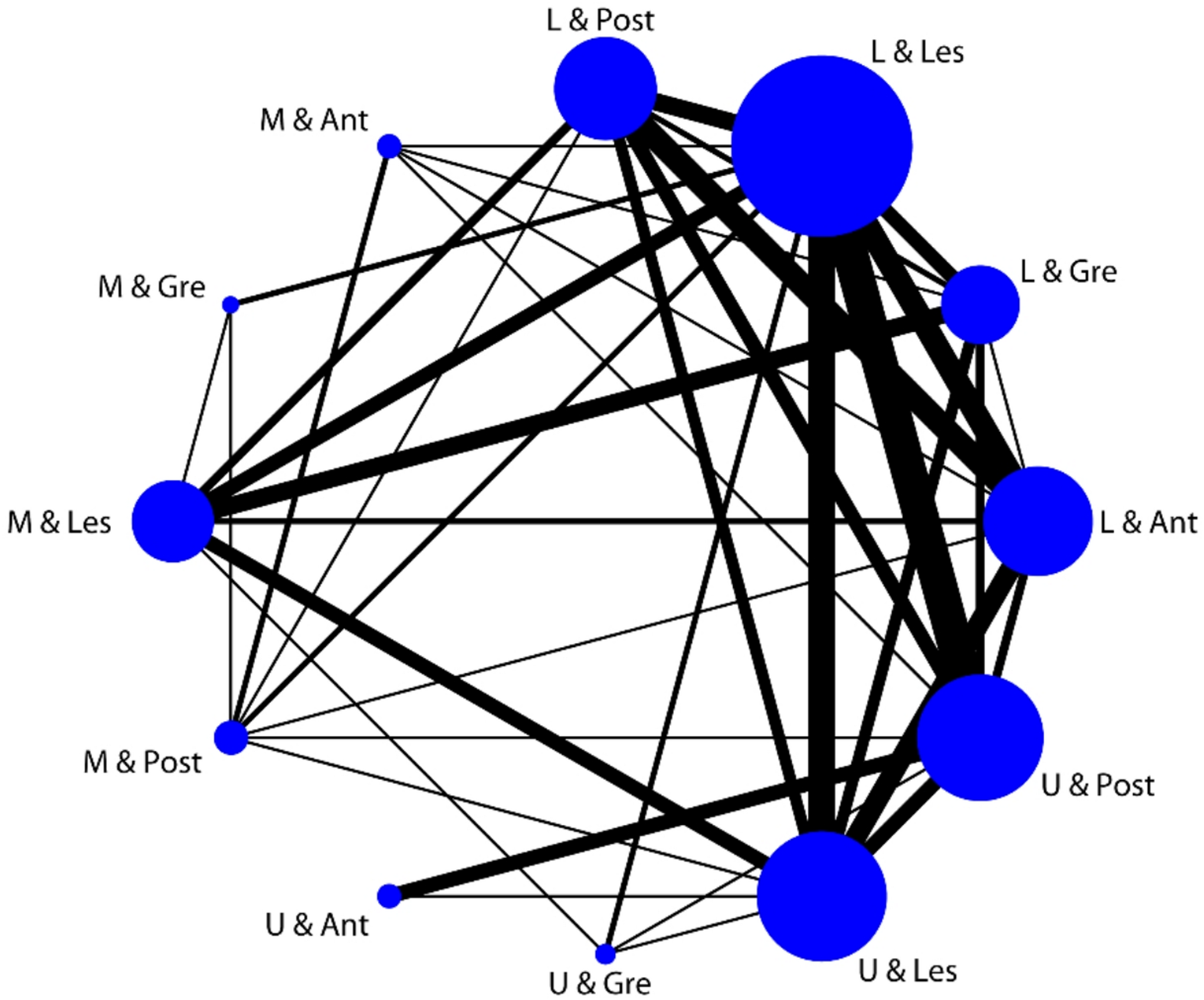
The kappa test was used to analyse the relationship between the spatial location of the main and minor lesions, and it was found that the main and minor lesions were consistent in longitudinal location (kappa = 1.141, p = 0.013). Although there was no correlation between the two lesions in the circumferential location (p > 0.05), 94 cases (72.3%) had at least one lesion located on the LC of the stomach, and 36 cases (27.7%) had two lesions located on the LC. The associative network diagram of the two lesion locations suggested that when lesions appear on the LC of the lower third of the stomach, attention should be paid to the presence of a lesion on the PW of the upper third of the stomach, and vice versa. Kitamura et al. (1997) confirmed that the tumour location was higher in MEGC than in solitary cancers (p < 0.05), and Eom et al. (2012) found that a lesion located in the UT of the stomach was a risk factor for MGC. In our study, 55.4% of the patients also had lesions in this area, suggesting that meticulous examination of the UT of the stomach in patients with SMEGC risk is required during endoscopy to avoid omission of the lesion. Our results support the hypothesis of ‘regional carcinogenesis’, which states that all gastric mucosa has the same carcinogenic background,each part is likely to develop into gastric carcinoma,and, eventually, carcinoma develops at two or more different sites simultaneously (Yasuda et al. 2000; Lee et al. 2010; Han et al. 2015; Ha et al. 2010). The high concordance in invasion depth (100% in the submucosal layer and 84.9% in the mucosal layer) likely results from two mechanisms: First, field cancerization leads to synchronous lesions with shared molecular alterations (e.g., p53 mutations) that promote parallel progression. Second, uniform microenvironmental factors (e.g., TGF-β signaling, biomechanical stress) drive synchronous invasion across lesions. These findings challenge the notion that minor lesions progress independently, instead showing that their invasion depth is closely linked to the main lesion's progression.
In this study, we analysed the risk factors for missed lesions and missed cases and found that lesion size and type were independent risk factors. The missed lesions were significantly smaller than the detected lesions. The proportion of other lesions (neither main nor minor) in the missed-lesion group was significantly higher than that in the detected-lesion group. A study (Lee et al. 2010) found that a small lesion size was the major risk factor for endoscopic failure to recognise additional lesions, which is consistent with our findings. In addition, Han et al. (2015), Ha et al. (2010) found that a small size and flat morphology were major risk factors for missing lesions. A Japanese multicentre study (Kato et al. 2013) found many missed lesions in the UT of the stomach. Ren et al. (2013) found that the rate of missed EGCs at the gastroesophageal junction was significantly higher than that at other sites.
This study also found that the hospital grade of preoperative gastroscopy was an influencing factor of missed diagnoses. The proportion of patients in the missed group, whose preoperative endoscopic examination hospital was grade II or below, was significantly higher than that in the detected group, which may be related to the experience of the endoscopic operators. Yalamarthi et al. (2004) performed a retrospective analysis of 305 patients diagnosed with upper gastrointestinal cancer and found that, among the missed cases, endoscopist errors accounted for the majority of failures (73%). However, other studies have shown that even experienced endoscopists in university-affiliated hospitals have a diagnostic omission rate of 14.7% (Lee et al. 2010; Lee et al. 2012). Eom et al. (2012) retrospectively studied 322 patients with MGC and revealed that 95 cases (29.5%) had missed lesions, and the risk factor for missed lesions was large-sized main lesions (p < 0.001). Therefore, endoscopists should master the objective laws of main and minor tumours and consider the risk factors for missed diagnoses to effectively reduce missed SMEGC.
The limitations of this study were as follows. First, this was a single-center retrospective study with a relatively small sample size. Second, the follow-up period was short; no patients died during the follow-up period. Third, the survival rate could not be accurately assessed.
In conclusion, SMEGC has a high incidence in a specific group. The lesion size, gross endoscopic type, histopathological type, and invasion depth of the main and minor tumours were correlated, and their spatial locations followed certain rules. Even after surgical treatment, a missed diagnosis of gastric cancer can still lead to tumour recurrence and poor prognosis; however, the characteristics of SMEGC can be easily overlooked during endoscopic examination.




Comments (0)