Over the past decade, numerous radiopharmaceuticals, including 32P, 89Sr, 223Ra, 188Re-/186Re-HEDP, 153Sm-EDTMP, 177Lu-EDTMP, and 177Lu-BPAMD, have been used to treat BM (Chakraborty et al. 2008; Liepe et al. 2003; Parlak et al. 2015; Sun et al. 2016). While these agents have demonstrated significant potential for pain palliation, most cannot be used as theranostic pairs due to the lack of corresponding diagnostic analogs, with the exception of 68Ga-/177Lu-BPAMD. Compared to 99mTc MDP SPECT, 68Ga-DOTA-IBA PET has shown superior efficacy in detecting BM. 68Ga-DOTA-IBA PET/CT can be employed for diagnosis, staging, and dynamic evaluation of therapeutic responses, providing opportunities for personalized treatment with 177Lu-DOTA-IBA (Deng et al. 2024). The 68Ga-/177Lu-DOTA-IBA combination offers a promising therapeutic approach for BM.
Fernández et al. conducted a pivotal dosimetry and safety assessment of 177Lu-DOTA-ZOL in metastatic castration-resistant prostate cancer, establishing the red marrow as the dose-limiting organ with a median maximum tolerated activity of 6 GBq (Fernándezet al. 2021). While their work validated the therapeutic potential of zoledronate-based radiopharmaceuticals, our study advances the field by introducing 177Lu-DOTA-IBA, a third-generation bisphosphonate with distinct pharmacokinetic advantages, including rapid blood clearance and higher target-to-background ratios (Qiu et al. 2023). Critically, we leveraged 68Ga-DOTA-IBA PET/CT to quantify treatment response through MTV, a novel imaging biomarker absent in prior studies. This theranostic approach combining 68Ga/177Lu-DOTA-IBA with MTV monitoring provides an actionable framework for personalized therapy adjustment, addressing the unmet need for response-guided dosing highlighted by Fernández et al. Furthermore, compared to Fernández et al.‘s cohort (100% prostate cancer), our study included diverse malignancies (lung, breast, prostate, etc.), demonstrating broader applicability. The favorable safety profile of 177Lu-DOTA-IBA (grade 3–4 hematotoxicity: 0% in our cohort vs. 33% with 177Lu-DOTA-ZOL) and its efficacy in pain palliation (82%) underscore its clinical potential for individualized BM management.
The objective of this study is to assess whether changes in MTV induced by 177Lu-DOTA-IBA therapy could serve as a predictive biomarker for OS in patients with BM. The lack of reliable biomarkers in routine clinical management of patients undergoing 177Lu-DOTA-IBA therapy remains a challenge. Previous studies have also shown variability in alkaline phosphatase (ALP) levels during 177Lu-DOTA-IBA treatment. To date, no effective imaging biomarker is routinely available for assessing treatment response. MTV has been demonstrated as a prognostic biomarker in various studies (Chardin et al. 2020; Jemaa et al. 2022; Pfannkuchen et al. 2017), and as a quantitative tool in PET/CT, it shows potential in evaluating the efficacy of 177Lu-DOTA-IBA therapy. IBA, a third-generation aminobisphosphonate, possesses anti-resorptive and anti-hypercalcemic properties. We successfully synthesized the chelating ligand DOTA-IBA complexed with DOTA. 68Ga-DOTA-IBA PET/CT can be utilized for the dynamic diagnosis, staging, and evaluation of therapeutic efficacy, enabling personalized 177Lu-DOTA-IBA radionuclide therapy. Our baseline data confirmed the prognostic value of both MTV and ALP for OS. In the bivariate analysis, baseline ALP levels exhibited a stronger correlation with OS compared to baseline MTV values, showing greater discriminatory power for OS. However, post-treatment analysis indicated that changes in MTV were more closely associated with OS. The findings suggest that treatment-induced variations in MTV could serve as a biomarker for response to 177Lu therapy. Kaplan-Meier analysis demonstrated that MTV response adds predictive value over ALP response alone in determining treatment outcomes. In our multivariable Cox proportional hazards model adjusted for the presence of visceral metastasis as a key covariate, the results demonstrated that even after adjusting for this prognostic factor, the MTV of BM remained a significant and independent predictor of OS (HR = 0.731, 95% CI = 0.26–2.07, p = 0.56). This indicates that the metabolic response of BM inherently possesses unique and independent prognostic value beyond that provided by other lesions. Our data also suggest an association between the administered dose of 177Lu-DOTA-IBA and changes in MTV. Patients receiving three or more doses of 177Lu-DOTA-IBA showed a significantly greater reduction in MTV compared to those receiving fewer doses (p = 0.035). Patients who received a higher number of injections of 177Lu-DOTA-IBA tended to experience better outcomes, including a significantly reduced risk of mortality, along with decreased pain scores and ALP levels.
This is important to note that 68Ga-DOTA-IBA uptake demonstrates heterogeneous patterns between osteoblastic and osteolytic lesions. Our prior work has demonstrated that the SUVmax of osteoblastic lesions is significantly higher than that of osteolytic lesions (7.88 versus 6.28, P < 0.001) (Liet al. 2025). For osteoblastic lesions: due to high 68Ga-DOTA-IBA uptake and excellent background contrast (tumor-to-background ratio > 3:1), changes in MTV can more sensitively reflect treatment response. For osteolytic lesions, however, MTV changes must be interpreted with caution. If treatment induces “osteolysis-to-osteoblasia” (e.g., after 177Lu-DOTA-IBA therapy), 68Ga-DOTA-IBA uptake may increase due to new bone formation, and an increase in MTV does not indicate progression. Interestingly, our prior work have shown that there are no significant differences in imaging responses among different types of BM (Xuet al. 2025). Bone scintigraphy with hydroxyapatite reflects increased osteoblastic activity; post-nuclear therapy bone scans may demonstrate a temporary increase in lesion activity (Isenseeet al. 2018). As a quantitative parameter, MTV can capture delayed responses in bone scans and stratify patients, facilitating more precise management and informing subsequent treatment decisions.
LimitationsRetrospective design and selection bias
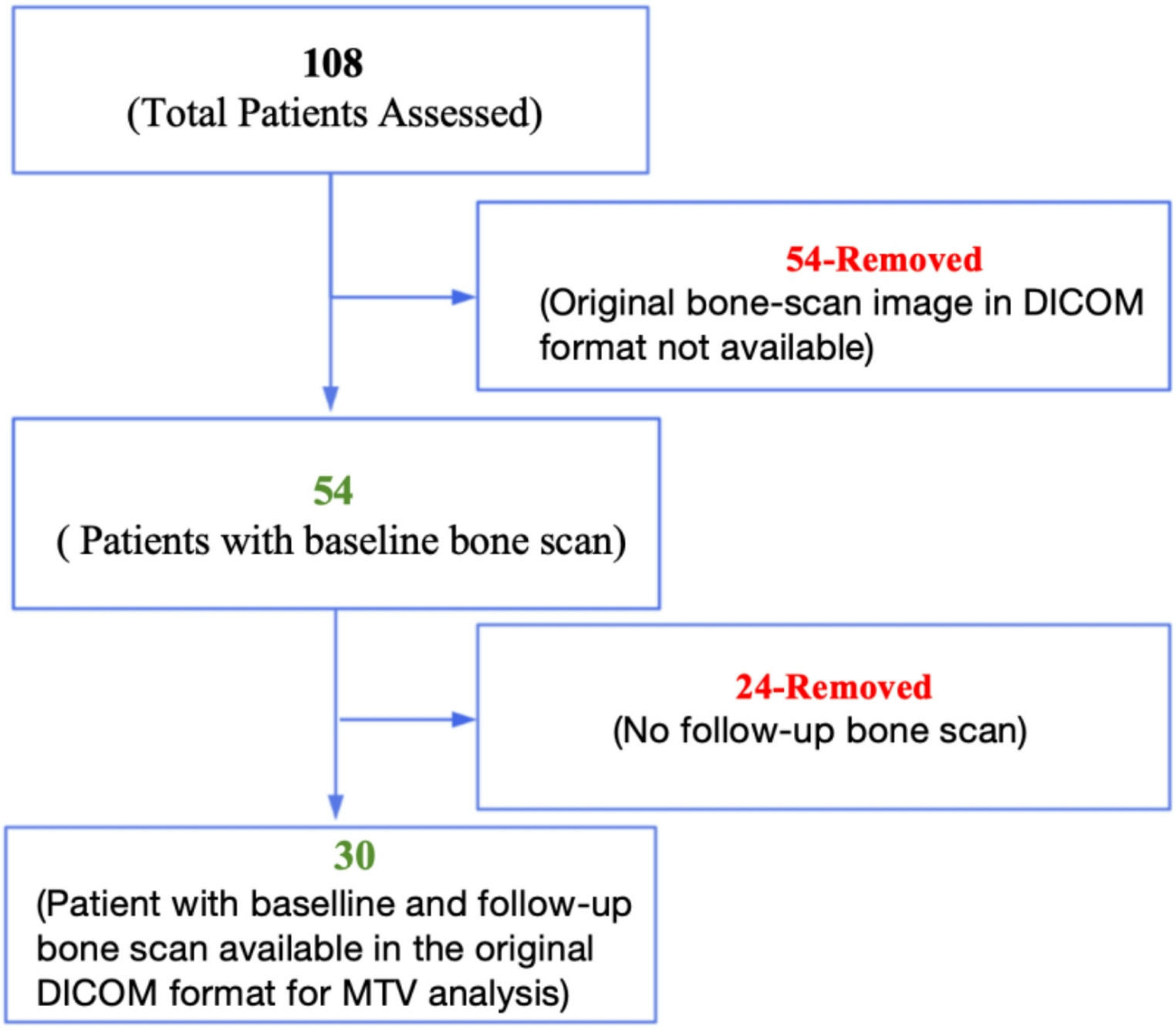
The inherent limitations of a retrospective analysis must be acknowledged. Data collection relied on pre-existing clinical records and imaging studies, which may introduce selection bias. For instance, only patients with both baseline and post-treatment 68Ga-DOTA-IBA PET/CT scans were included (n = 30/54), potentially excluding those with rapid progression or early death. This could skew results toward a cohort with better prognosis, overestimating the predictive value of MTV changes. Additionally, treatment schedules (1–5 cycles of 177Lu-DOTA-IBA) and follow-up intervals were not standardized, introducing heterogeneity in response assessment.
Limited sample size and tumor heterogeneity
The final cohort (n = 30) lacked statistical power for robust subgroup analyses. Patients had diverse primary malignancies (e.g., prostate, breast, lung), each with distinct biological behaviors and metastatic patterns. Notably, 20% had liver/lung metastases (Table 1), which independently impact OS but were not adjusted for in MTV-OS analyses. The small sample precluded stratification by tumor type or metastatic burden, limiting generalizability of MTV as a universal biomarker. Future multi-center studies with larger cohorts are needed to validate MTV’s prognostic role across tumor subtypes.
Technical variability in MTV quantification
MTV measurements using the Hermes platform (OLINDA/EXM 2.0) depend on threshold-based segmentation, which may vary between observers. Although consensus readings minimized inter-observer discordance, the lack of a standardized MTV calculation protocol (e.g., fixed SUV threshold vs. adaptive methods) could affect reproducibility. This is particularly relevant for sclerotic or heterogeneous lesions, where background uptake may confound MTV accuracy.
Nevertheless, the MTV response data are unique and merit prospective validation.




Comments (0)