Study Design
In this non-interventional, observational study, online web-based surveys were conducted involving treating physicians—including diabetologists and general internists—and individuals with T2D in Japan. The study was conducted in accordance with the Declaration of Helsinki and the Guidelines for Good Pharmacoepidemiology Practices. The study protocol, consent forms, and questionnaires were approved by an independent ethics committee of the Research Institute of Healthcare Data Science (approval number RI2023005). All respondents provided informed consent online, and were made aware and gave consent that their responses would be published in a medical journal. All personal information was managed by Macromill, Inc. (Tokyo, Japan), was used solely for the purposes of this study, and was not provided to the study sponsor.
Study Participants
Physicians and individuals with T2D were recruited via panels maintained by CareNet, Inc. (Tokyo, Japan) and Macromill, Inc., who also conducted the survey. Eligible physicians were those managing ≥ 50 individuals with T2D per month and who had managed ≥ 1 individual with T2D with oral semaglutide. Physicians were predominantly based at clinics or hospitals. Physicians with < 2 years of experience were excluded. Eligible individuals were aged ≥ 20 years with a diagnosis of T2D and had been receiving oral glucose-lowering therapy for ≥ 6 months. Two groups of individuals were assessed: those receiving oral semaglutide and those taking other oral glucose-lowering therapies; the latter were sex- and age-matched to those receiving oral semaglutide. Other oral glucose-lowering therapies, such as sodium–glucose cotransporter-2 inhibitors and DPP4is, have fewer dosing requirements, so including this group provides a comparator for general perception of treatment administration versus oral semaglutide.
Questionnaires
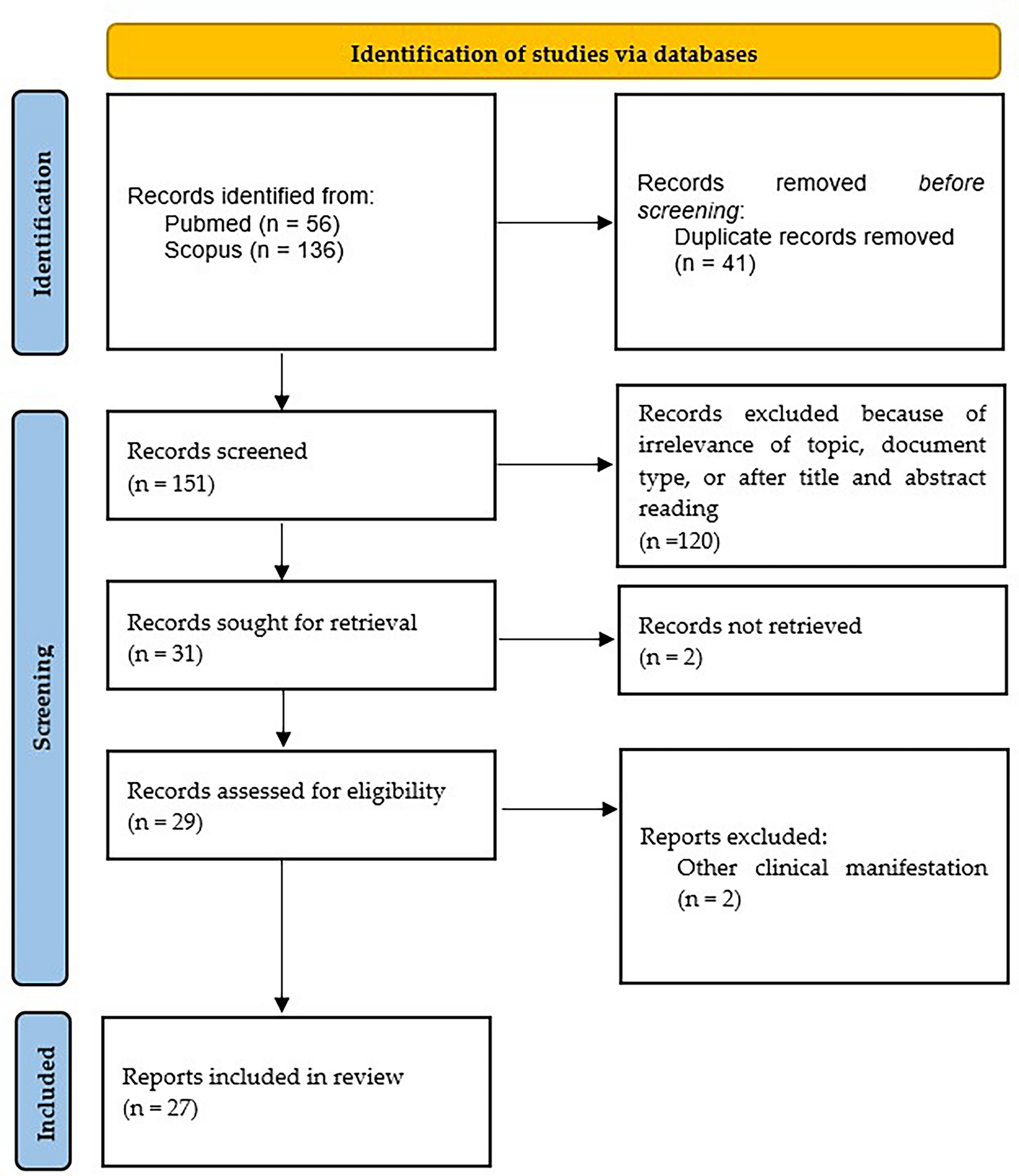
Separate questionnaires were developed for physicians and individuals with T2D under clinical guidance, and in conjunction with searches performed using PubMed and ICHUSHI online bibliographic databases. The questionnaires were validated and refined by conducting web-based cognitive interviews of a small number of each target population. All interviews and the survey (including the questionnaires) were conducted in Japanese. The (translated) questionnaires are provided in the Supplementary Material.
Respondents completed a single questionnaire to provide their demographics and to share their perceptions of the oral semaglutide dosing requirements at two time points: at baseline, i.e., before prescribing oral semaglutide (physicians) or before initiating oral semaglutide (individuals with T2D); and at the time of survey, i.e., after prescribing oral semaglutide (physicians) or receiving oral semaglutide for ≥ 6 months (individuals with T2D who went on to receive oral semaglutide). Respondents who received oral glucose-lowering medications other than semaglutide were asked to share their perceptions at baseline only. The questionnaire asked physicians to recall which oral semaglutide dosing requirements they had concerns about before prescribing oral semaglutide (baseline) and to report difficulties experienced by their patients after prescribing oral semaglutide (time of survey). All individuals with T2D who initiated semaglutide were asked to recall which oral semaglutide dosing requirements they had expected, at baseline (before initiating oral semaglutide), to be difficult to adhere to, and to report the difficulties they experienced at time of survey (after receiving oral semaglutide for ≥ 6 months). For those who received other oral glucose-lowering therapies, a description of the dosing requirements was provided without oral semaglutide being named, and individuals were asked if they envisaged any difficulties adhering to the dosing requirements if they took such a medication.
Objectives and Endpoints
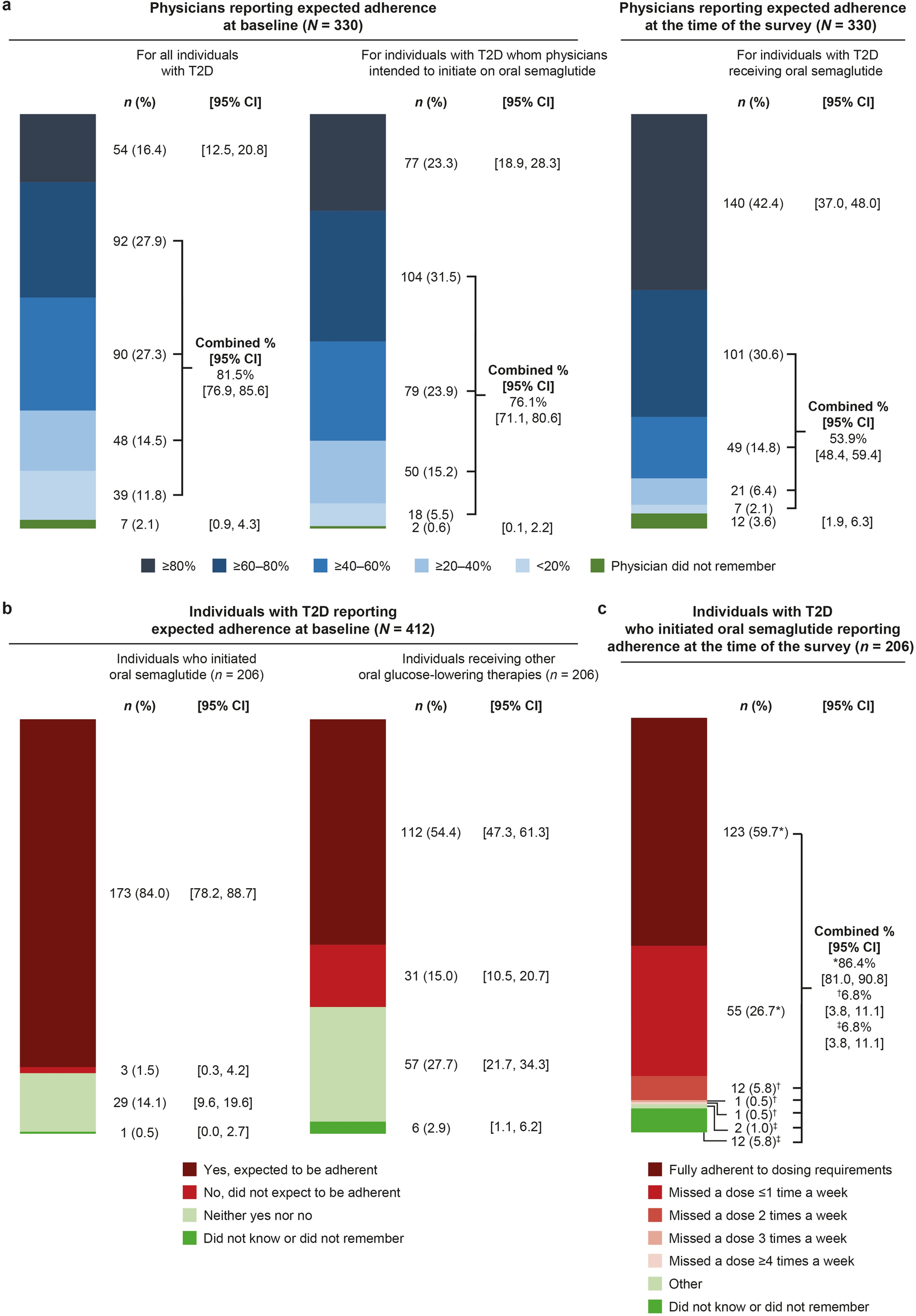
The primary objective was to identify any changes in physicians’ perceptions of dosing adherence to oral semaglutide between the two time points, baseline and the time of survey. The primary endpoint was the change from baseline to the time of survey in the percentage of physicians who considered their patients likely to adhere (at baseline; all patients with T2D) versus those whose patients were adhering (at time of survey; patients receiving oral semaglutide) to oral semaglutide dosing requirements.
Secondary endpoints were the patient-reported change in percentage of individuals that received oral semaglutide who expected to adhere to the dosing requirements (baseline) versus actual adherence to dosing requirements (at the time of survey). The patient-reported secondary endpoint also included the percentage of individuals who received oral glucose-lowering medication (other than semaglutide) who expected to adhere to the semaglutide dosing conditions (baseline). The physician-reported, secondary endpoint was a change in the percentage of physicians who expected the T2D patients to whom they intended to introduce oral semaglutide to adhere to the dosing requirements (at baseline) versus those whose patients showed actual adherence (as considered by physicians) (at the time of survey).
Exploratory objectives assessed factors related to dosing adherence to oral semaglutide. Exploratory endpoints at baseline included the percentage of respondents reporting each dosing requirement as a concern before initiating oral semaglutide (for both physicians and individuals with T2D initiating oral semaglutide) and the percentage of physicians with expected reasons for non-adherence. Exploratory endpoints at the time of survey included the percentage of respondents experiencing difficulties with oral semaglutide (for both physicians and individuals with T2D) and any changes from baseline in physicians’ resistance to prescribing oral semaglutide, along with the point at which physicians changed their resistance to prescribing oral semaglutide.
Statistical Analyses
The planned number of respondents was 300 physicians, 200 individuals with T2D receiving oral semaglutide, and 200 individuals with T2D receiving other oral glucose-lowering therapies. The sample size calculation was not based on statistical considerations but rather on the intention to include as many respondents as possible. Based on previous experience, it was thought that between 200 and 300 respondents would be feasible [16]. The 200 individuals receiving other oral glucose-lowering therapies were set in accordance with the number of individuals receiving oral semaglutide to allow age- and sex-matching of respondents.
The physician full analysis set (FAS) comprised diabetes specialists and non-specialists who had ≥ 2 years of experience, managed ≥ 50 patients with T2D per month, and managed ≥ 1 patient with oral semaglutide. The FAS for individuals with T2D comprised adults aged ≥ 20 years with T2D who were receiving oral antidiabetic therapies and who had been using oral semaglutide or other oral glucose-lowering therapies for ≥ 6 months. For the primary and secondary endpoints, comparisons between before and after initiating oral semaglutide were made using a McNemar test for the nominal variables; 95% confidence intervals were calculated. If there were ≥ 20% cells with a frequency of < 5, Fisher’s exact test was applied. For exploratory endpoints, summary statistics were calculated for each group. The frequency and percentage were calculated for nominal and ordinal variables, and summary statistics were calculated for continuous variables. As the survey was designed to prevent respondents from omitting any responses and could not be completed until all questions were answered, no missing values existed in the study dataset. Individuals who responded “neither yes nor no,” “other,” “do not know,” or “do not remember” at one or both time points were excluded from McNemar and Fisher’s tests; however, all responses were included in descriptive analyses for the primary and secondary endpoints. Statistical analyses were performed using SAS version 9.4 or R version 4.1.2 or higher.

Comments (0)