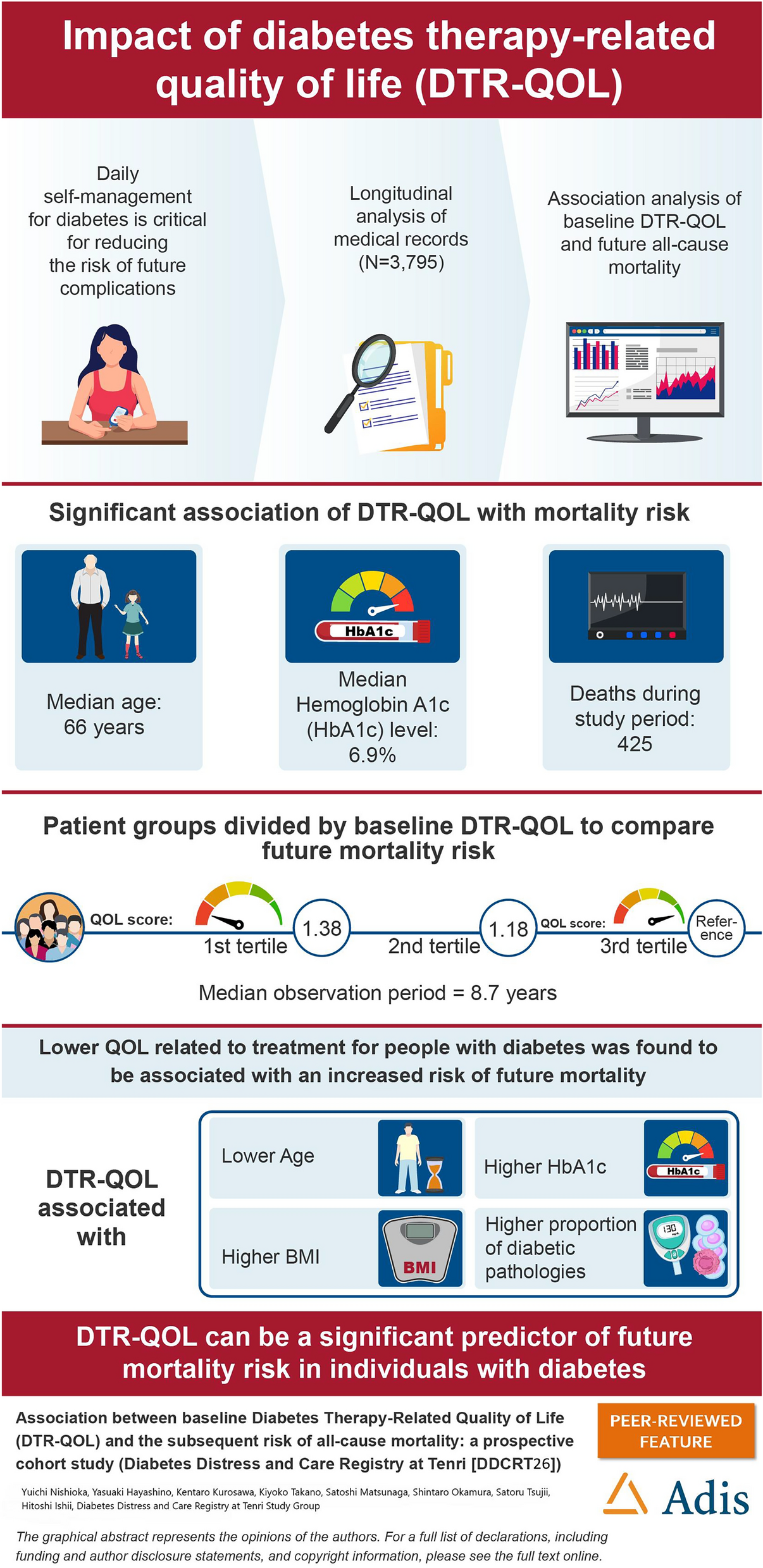
To the best of our knowledge, this is the first study to prospectively evaluate the association between diabetes-related QOL and the subsequent risk of all-cause mortality in individuals with diabetes. Compared with individuals in the third tertile DTR-QOL score group, those in the first tertile at baseline were associated with a higher risk of all-cause mortality. Our results may be valuable because we revealed that lower DTR-QOL is associated with a high mortality risk after adjusting for possible factors relevant to mortality risk, such as glycemic control or complications. The difference between the unadjusted model and the models adjusting for sex and age may be because lower DTR-QOL scores were associated with longer life expectancies (younger age and female sex) (Table 1).
The DTR-QOL is a questionnaire developed to measure the impact of diabetes therapy on the QOL of participants. The 29 questions were divided into four domains. Domain 3 included anxiety and uneasiness about hypoglycemic symptoms, and domain 4 included satisfaction with the current therapy and confidence in continuing it. Overall, this study measured the physical and psychological burdens associated with diabetes therapy [11], which have been proven to be associated with important parameters related to diabetes therapy and its effectiveness. The total score is associated with HbA1c level, frequency and severity of hypoglycemia, weight, therapy modalities, age, subjective health, disease type, and communication with physician [11]. A simultaneous comparison of DTR-QOL and EQ-5D-5L was conducted on the same participants; EQ-5D-5L responded to the severity of various health conditions but showed no difference in HbA1c level, weight, age, and hypoglycemia. In contrast, DTR-QOL detects differences in these factors and comorbidities [28]. In randomized comparative studies of new and conventional drugs in drug therapy, and switching observation studies, HbA1c levels and other parameters were simultaneously measured and evaluated in terms of HRQOL. The results of this study indicated that QOL, measured as an impact (outcome) of daily therapy on individuals, is related to mortality. Moreover, this is independent of HbA1c level, age, sex, comorbidities, and type of therapy.
The SF36 [29] and EQ5D [23] have been widely used. Both are generic and assess physical, mental, and social functions; however, there is a difference between the profile type (PCS and MCS) and index type (utility 0–1 depending on health status). In the ZODIAC study of 1353 people with type 2 diabetes, HRQOL was measured at baseline using the RAND-36 and followed up for a mean of 5.8 years. The physical component was reported to be an independent marker of all-cause mortality. At the 10-year follow-up, the mental and lower physical components were associated with higher total and cardiovascular mortality [12]. In a study comparing patients with and without diabetes (9979, mean 7.4 years), mortality was higher among patients with diabetes and a low PCS, with the strongest relationship being observed in patients with diabetes and a low PCS. The relationship between the PCS and mortality was stronger in the high HbA1c level group, and a similar relationship was observed for MCS; however, the effect was independent of the PCS. By health dimension, physical functioning, general health perception, and vitality were commonly associated with cardiovascular disease and all-cause mortality risk [18, 22]. Furthermore, studies on patients with diabetes undergoing dialysis have reported only the physical component of the baseline SF36 [30] and only the mental component [16] as independent predictors of mortality. In surveys of the general population and those with risk factors, including diabetes, the PCS or MCS correlated with mortality in studies using the SF, with the PCS being the most frequently reported predictor of mortality [14].
People with diabetes (N = 7892) were followed for a mean of 3.7 years, and the relationship between mortality and baseline EQ5D score (utility) was found to be significant, with a mean EQ-5D score of 0.73 (SD = 0.20) for the deceased and 0.81 (SD = 0.18) (p < 0.0001) for the survivors. This relationship was maintained even after adjusting for demographic, socioeconomic, and clinical risk factors for mortality [13]. As part of the FIELD study, an analysis of 7348 people with type 2 diabetes followed up for a mean of 2.5 years also found that EQ-5D index scores were significantly associated with future vascular events, other complications, and the risk of mortality. When analyzed by dimension, the risk of future vascular events, other complications, and all-cause mortality was higher for the mobility dimension and for those who reported extreme problems, regardless of the dimension [31]. Overall, QOL values as measured by the general HRQOL scale are associated with life expectancy, although there are small differences between studies. That is, declines in physical, mental, and social functioning affected by aging, disease, and comorbidities increase mortality risk. QOL values reflect subjective assessments of physical and psychological burden and subjective health status, which cannot be measured using traditional risk factors (e.g., blood glucose levels, HbA1c levels, blood pressure, lipids, and smoking). These are more comprehensive representations of health status than individual factors [18, 32]. However, it is unclear whether the causal relationship is direct or a single factor. Nonetheless, it should be recognized that QOL values are useful markers independent of other clinical markers.
One study on diabetes-specific questionnaires and mortality is the PAID, a questionnaire that measures the emotional burden (diabetes distress) associated with diabetes, diabetes therapy (diet, hypoglycemia, etc.), and relationships with others. A follow-up of 3305 people with type 2 diabetes for an average of 6.1 years to determine the association with baseline diabetes distress (PAID) showed that diabetes distress (PAID score) was significantly associated with all-cause mortality in men [25].
The DTR-QOL is a diabetes-specific questionnaire; however, it is unique in its focus on therapy-related items. Planning diabetes therapy is a complicated demand [33]. Medication regimens are often complex and cause side effects [34, 35]. Intensive therapy regimens raise the risk of hypoglycemia [34, 35]. This reduces the QOL [36]. Hypoglycemia and weight gain are also problematic [37]. Added to these are the burdens of time, timing of therapy, HbA1c and blood glucose levels, and their variability. The same is true for oral drug therapy [38]. The fact that the DTR-QOL includes such diabetes therapy-specific questions and is associated with mortality means that HRQOL as a subjective assessment of daily therapy is independent of conventional medical risk factors, such as age, HbA1c level, blood pressure, cholesterol level, and the degree of complications. The DTR-QOL is a predictor of lifetime therapy goals independent of conventional medical risk factors. The unique feature of this questionnaire, among others, is that it measures daily therapy burden, and we found that a low therapy burden, as well as a large therapy benefit, is associated with a longer life span. In terms of subdomains, at the time of this analysis, domain 1, “Burden on social activities and daily activities” was associated with mortality. Items in this domain include restrictions on important activities due to therapy, limitations on food and time freedom, worry, pain, and gastrointestinal symptoms. In particular, many questions were related to activity and time-use restrictions, which may be related to mortality. However, it is not clear whether this is a cause–effect relationship with mortality or just another marker.
In relation to therapy execution, there is evidence that the DTR-QOL is associated with insulin (total, subdomains 1–4) and exercise therapy (total, subdomains 1, 3, and 4) [39,40,41]. Therefore, a low degree of self-management may be associated with increased mortality rates. Using the DTR-QOL, it has been demonstrated that insulin therapy adherence is associated with QOL [40], and therapy adherence is associated with HbA1c levels [41]. The ITR-QOL, a pro and con type of the DTR-QOL, has demonstrated an association between QOL improvement, therapy implementation, and HbA1c improvement for insulin therapy. In this study, the baseline DTR-QOL was also proven to predict the HbA1c level at the 7-year follow-up. However, the baseline HbA1c levels were not associated with mortality. Supplementary Table 3 shows that the predictive ability for death was lost when the updated HbA1c level in 2017 was added to the model. Based on these results, it is possible that part of the association between DTR-QOL and mortality occurs through glycemic control. Additionally, the association between DTR-QOL and mortality may be mediated by comorbidities. As DTR-QOL and mortality are independent of HbA1c levels, complications, age, and therapy, other factors must also be considered. One study found that patients with higher CARE scores (perceived empathic support from their physicians) in the first year had a lower risk of all-cause mortality. In other words, the study demonstrated that the physician–patient relationship influenced mortality [42]. The DTR-QOL values were higher for those who reported good communication with their physicians regarding therapy options. This type of person-centered care may influence mortality [11]. Although a causal relationship has not yet been identified, improving daily therapy-related QOL may lead to a decrease in mortality. In other words, the application of therapy that improves and maintains daily DTR-QOL may improve future life expectancy and QOL. For example, newer formulations, such as third-generation sustained-release insulin [43], fixed-ratio combination (FRC) combinations [44], glucagon-like peptide 1 (GLP-1) receptor agonists [45], and newer ultra-rapid-acting insulins [46] have been proven to improve DTR-QOL compared with traditional formulations. These newer formulations have been proven to improve DTR-QOL compared with traditional formulations. These newer formulations may reduce mortality by improving HRQOL. The development of therapies that improve the QOL and whether they lead to a reduction in mortality should be examined for all therapies, and not just for these drug therapies.
The present study has a few limitations. First, because this was an epidemiological study, residual confounders may exist for the association between DTR-QOL and all-cause mortality risk. Second, the data on socioeconomic factors of the participants were insufficient; therefore, it is yet to be elucidated whether these factors influence the aforementioned association. Third, our dataset included less information at follow-up assessments of DTR-QOL. Specific treatment-related events during follow-up, such as weight gain, symptomatic hypoglycemia, treatment switching, prescription of comorbidities, or worsening health status, are not included. Further studies are needed to elucidate the underlying mechanisms of the observed association. Fourth, excluding people who are too severely ill to participate in the registry may have biased the sample toward healthier individuals. Finally, the data were obtained from the registry of a single diabetes center, thereby raising concerns regarding the generalizability of the results (e.g., primary care setting, region, and ethnicity).

Comments (0)