
Remember me
Prediabetes is a growing global health concern. In 2021, the global prevalence of impaired glucose tolerance (IGT) among adults aged 20–79 was estimated at 9.1% (464 million individuals), projected to rise to 10.0% (638 million) by 2045. Similarly, prevalence of impaired fasting glucose (IFG) was 5.8% (298 million) in 2021, with projections reaching 6.5% (414 million) by 2045. High-income countries currently exhibit the highest prevalence rates, but the most significant relative increases are anticipated in low-income nations [1].
Obesity plays a pivotal role in the pathogenesis of prediabetes and the global obesity epidemic has been identified as a major driver of the increasing prevalence of prediabetes and type 2 diabetes (T2D). Excess adiposity, particularly visceral fat, contributes to insulin resistance, a key mechanism underlying the development of prediabetes and its progression to T2D. Pancreatic steatosis has also been claimed to mediate the impact of obesity on glucose metabolism by affecting beta-cell function [2, 3].
There is huge expectation that new medications for effective weight management can reshape metabolism, reverse prediabetes, and halt the progression to T2D.
In the SURMOUNT-1 trial [4], among 1032 participants with obesity and prediabetes observed over 176 weeks, the dual glucagon-like peptide 1 (GLP-1)/gastric inhibitory polypeptide (GIP) receptor agonist tirzepatide reduced body weight by up to 20% (with the 15-mg dose) and effectively reduced the rate of progression to diabetes to near-zero levels during the treatment period. Moreover, tirzepatide facilitated regression to normoglycaemia in most cases. Mediation analysis estimated that 38.9% of this tirzepatide effect was attributable to weight loss, suggesting that over 60% of the effect may be mediated by direct improvements in glycaemic control, likely through the activation of GLP-1 and GIP receptors on beta cells.
The rates of progression from prediabetes to diabetes were 3.9 per 1000 patient-years in the tirzepatide group (10 cases among 762 participants over 176 weeks) compared to 39.4 per 1000 patient-years in the placebo group (36 cases among 270 participants over 176 weeks), with a hazard ratio (HR) of 0.07. Interestingly, the progression rate in the placebo group was lower than that reported in a recent UK cohort (53.5 per 1000 patient-years) [5].
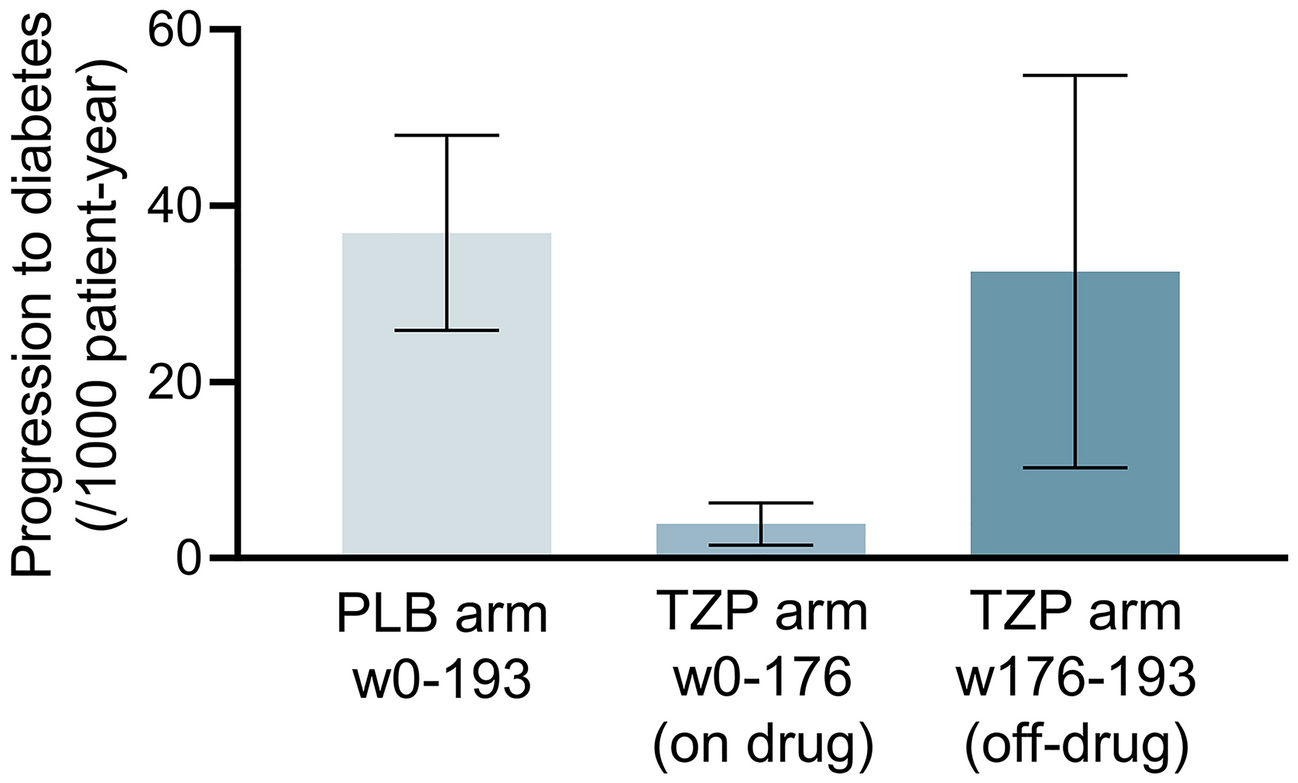
Notably, during the 17-week off-treatment period, an additional 1.1% of participants in the tirzepatide group progressed to diabetes [4], resulting in an estimated rate of 32.5 per 1000 patient-years—a rate similar to that observed in the placebo group during the entire study period (36.9 per 1000 patient-years). This indicates that nearly 90% of the protective effect of tirzepatide against diabetes progression was lost within weeks after discontinuation (Fig. 1).
Fig. 1
Rates of progression from prediabetes to type 2 diabetes in SURMOUNT-1. Rates are presented as number of progressors/1000 patient-years. Three estimates are presented: for the placebo (PLB) arm during the entire observation (weeks 0–193, including off-drug period); for the tirzepatide (TZP) arm while on drug (weeks 0–176); for the TZP arm while off-drug (weeks 176–193). Bars indicate confidence intervals. No formal statistical analysis was performed, but the non-overlapping confidence intervals of the three estimates indicate significance at the conventional 5% type I error. Data are derived from the primary publication [4]
After 17 weeks off treatment, participants in the tirzepatide group had regained only 2–3% of their body weight [4], preserving more than 80% of the weight loss achieved during treatment. However, glycaemic markers showed faster reversals: HbA1c, which had declined by 0.43% (placebo-adjusted) during the treatment period, increased by 0.20% during the off-drug period; fasting glucose, which had declined by 13.4 mg/dL during treatment, rose by 8.8 mg/dL after discontinuation. Thus, an estimated 50–70% of the glycaemic benefits of tirzepatide were lost within 4 months of stopping the drug [4].
This critical analysis of the data underscores that the glycaemic effects of tirzepatide vanished more rapidly than its weight-loss effects following discontinuation. Overall, this is in line with the mediation analysis performed by the authors, showing that the effects on glycaemic and weight control are largely separated [4]. It is also consistent with a recent retrospective study showing that weight loss occurring within 5 years after T2D diagnosis and maintaining for up to 20 years has only transient effects on glucose control and does not modify the natural history of T2D [6].
In SURMOUNT-1, the protection against diabetes progression was sustained only while tirzepatide was being administered. Remarkably, even after 3 years of stable and effective weight management and normoglycaemia in most participants, the underlying dysglycaemia re-emerged rapidly after treatment cessation. This should not be surprising from a classical pathophysiological perspective. People with class 2–3 obesity in their 40s who are selected for having prediabetes will most likely have a genetic predisposition to beta-cell failure [7, 8]. Despite remarkable and persistent weight loss, their beta cells are bound to a progressive functional decline.
In summary, tirzepatide demonstrates exceptional efficacy on glycaemic and weight control. SURMOUNT-1 shows that tirzepatide can arrest the progression from prediabetes to diabetes [4], while the SURPASS studies demonstrate that tirzepatide can aid pharmacologic remission of T2D [9]. However, once the drug is stopped and the GLP-1/GIP receptors are no longer overstimulated, the clock restarts ticking as dysfunction of beta cells re-emerges.
These results are sobering regarding the possibility to fundamentally alter the path from obesity to T2D. Once more, the lesson learned is that the natural history of T2D is determined by individual predisposition and not only by excess body weight.
Comments (0)