
Remember me
After applying all inclusion and exclusion criteria, the final SGLT2i cohorts comprised 12,501 patients in DNHR, 22,404 in VID, 811 in J-CKD-DB-Ex, and 54,308 in Optum® EHR (Appendix C [Supplementary Material], Table C1). The final GLP-1 RA cohorts comprised 10,696 in DNHR, 8317 in VID, 219 in J-CKD-DB-Ex, and 78,934 in Optum® EHR (Appendix C, Table C2).
Baseline Demographic CharacteristicsWithin each data source, the mean ages of patients were generally similar for each medication cohort but varied across data sources, ranging from 62 to 70 years. Across data sources, the proportion of female patients ranged from 35.9 to 44.4% (SGLT2i cohorts) and from 40.0 to 51.3% (GLP-1 RA cohorts) (Table 1). Tables C3–C6 (Appendix C) summarize other baseline characteristics by data source. The proportion of patients with stage 3 CKD at baseline based on a diagnosis code or eGFR value ranged from 23.1 to 46.5% in SGLT2i cohorts and from 33.6 to 45.2% in GLP-1 RA cohorts. Laboratory data were quite complete in all data sources, except for UACR, for which 17.1 to 48.6% of participants were missing data. For eGFR at baseline, the percentage of patients with missing results was 10% or less in all cohorts (Appendix C, Tables C7–C8). Across all data sources, obesity and indicators of T2D severity (e.g., insulin use at the index date, higher HbA1c level) were more common at baseline in the GLP-1 RA cohorts than in the SGLT2i cohorts. The GLP-1 RA cohorts also tended to have worse renal function at baseline than did the SGLT2i cohorts.
Table 1 Selected baseline characteristics of SGLT2i and GLP-1 RA new users by data sourceOutcomesIn consideration of differences across data sources in healthcare setting, data type (e.g., administrative claims, EHR), and length of follow-up, primary outcomes (i.e., kidney failure, cardiovascular outcomes) and secondary outcomes (i.e., change in eGFR and serum potassium measurements) for SGLT2i and GLP-1 RA cohorts are presented separately by data source.
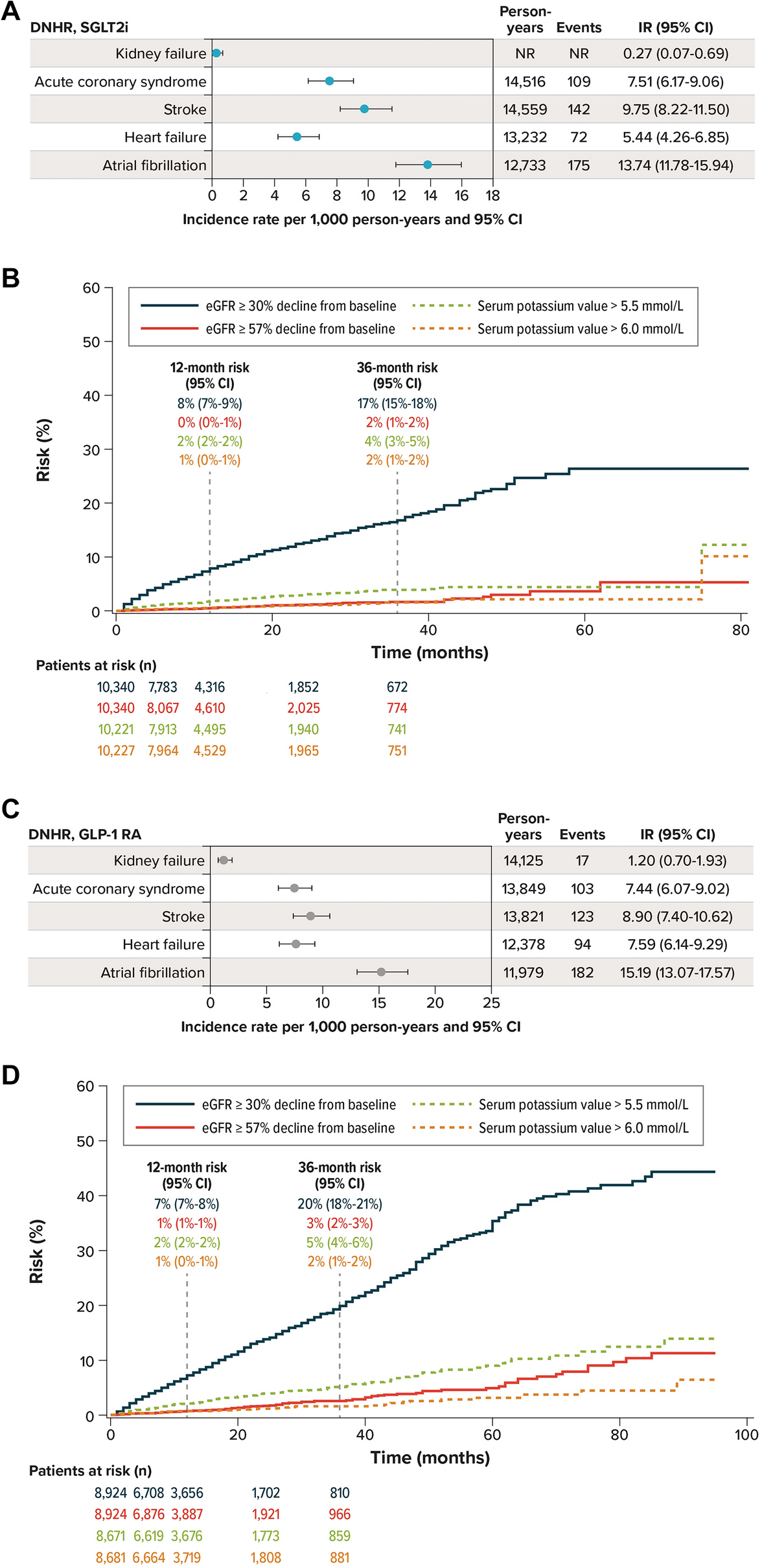
DNHRSGLT2i CohortIn the SGLT2i cohort, the IR of kidney failure was 0.27 events per 1000 PY during follow-up of approximately 80 months. Among cardiovascular outcomes, new-onset AF was most common (IR, 13.74/1000 PY), followed by stroke (IR, 9.75/1000 PY), ACS (IR, 7.51/1000 PY), and new-onset HF (IR, 5.44/1000 PY) (Fig. 1a). In alignment, the risk of AF was higher than all other outcomes at all timepoints, while risk of stroke and ACS was similar until approximately 2 years after the index date and again by the end of follow-up (i.e., maximum of approximately 80 months). The curves for HF and ACS were nearly superimposed until approximately 60 months of follow-up (Appendix C, Figure C1a). As illustrated by the cumulative incidence curve, there were very few kidney failure events in this cohort throughout the follow-up period.
Fig. 1
Outcomes: DNHR. a Incidence rates of primary outcomes, SGLT2i cohort. b Cumulative incidence of secondary outcomes, SGLT2i cohort. c Incidence rates of primary outcomes, GLP-1 RA cohort. d Cumulative incidence of secondary outcomes, GLP-1 RA cohort. CI confidence internal, DNHR Danish National Health Registers, eGFR estimated glomerular filtration rate, GLP-1 RA glucagon-like peptide-1 receptor agonists, IR incidence rate, NR not reported, SGLT2i sodium-glucose cotransporter 2 inhibitors
The risk of eGFR declines ≥ 30% from baseline was 17% at 36 months, compared with 2% for eGFR declines ≥ 57% (Fig. 1b). Over the entire follow-up period, the risks of serum potassium values > 5.5 mmol/l and > 6.0 mmol/l were similar (36 months: 4% and 2%, respectively) (Fig. 1b).
GLP-1 RA CohortIn the GLP-1 RA cohort, the IR of kidney failure was 1.20 events per 1000 PY during follow-up of approximately 95 months. Atrial fibrillation was the most common cardiovascular outcome (IR, 15.19/1000 PY), followed by stroke (IR, 8.90/1000 PY), HF (IR, 7.59/1000 PY), and ACS (IR, 7.44/1000 PY) (Fig. 1c). The risk of AF was higher than that of all other outcomes at all timepoints, while the risk of stroke, ACS, and HF was similar. Kidney failure incidence increased until approximately 50 months of follow-up and remained lower than the cardiovascular outcomes at all timepoints (Appendix C, Fig. C1b).
At 36 months, declines in eGFR ≥ 30% from baseline had a risk of 20% compared with 3% for eGFR declines ≥ 57%, and the risks of serum potassium values > 5.5 mmol/l and > 6.0 mmol/l were 5% and 2%, respectively (Fig. 1d).
J-CKD-DB-ExSGLT2i CohortIn the SGLT2i cohort, the IR of kidney failure was 8.88 events per 1000 PY during follow-up of approximately 55 months. Among cardiovascular outcomes, new-onset HF was most common (IR, 115.50/1000 PY), followed by stroke (IR, 45.54/1000 PY), ACS (IR, 40.53/1000 PY), and AF (IR, 16.07/1000 PY) (Fig. 2a). The risk of HF, which tended to occur relatively early during follow-up, was higher than the risk of all other outcomes at each timepoint (Appendix C, Fig. C2a). Risk of stroke and ACS was similar throughout follow-up. Risk of kidney failure and AF was similar throughout follow-up without notable time trends.
Fig. 2
Outcomes: J-CKD-DB-Ex. a Incidence rates of primary outcomes, SGLT2i cohort. b Cumulative incidence of secondary outcomes, SGLT2i cohort. c Incidence rates of primary outcomes, GLP-1 RA cohort. d Cumulative incidence of secondary outcomes, GLP-1 RA cohort. CI confidence internal, eGFR estimated glomerular filtration rate, GLP-1 RA glucagon-like peptide-1 receptor agonists, IR incidence rate, J-CKD-DB-Ex Japan Chronic Kidney Disease Database Extension, SGLT2i sodium-glucose cotransporter 2 inhibitors
At 36 months, the risk of eGFR declines ≥ 30% was 27% at 36 months compared with 4% for declines ≥ 57%, and risks of serum potassium values > 5.5 mmol/l and > 6.0 mmol/l were 16% and 4%, respectively (Fig. 2b).
GLP-1 RA CohortIn the GLP-1 RA cohort, the IR of kidney failure was 21.65 events per 1000 PY during follow-up of approximately 55 months. New-onset HF was the most common cardiovascular outcome (IR, 177.21/1000 PY), followed by ACS (IR, 35.47/1000 PY), stroke (IR, 33.96/1000 PY), and AF (IR, 11.65/1000 PY) (Fig. 2c). The risk of HF deviated from that of the other outcomes in the first 3 months and remained the most common event at each timepoint, while risk of stroke, ACS, kidney failure, and AF was similar throughout the follow-up period, with overlapping curves (Appendix C, Fig. C2b).
At 36 months, the risk of eGFR declines ≥ 30% was 44%, while risk of declines ≥ 57% remained lower at 6%, and risks of serum potassium values > 5.5 mmol/l and > 6.0 mmol/l were 34% and 15%, respectively (Fig. 2d).
VIDSGLT2i CohortIn the SGLT2i cohort, the IR of kidney failure was 0.58 events per 1000 PY during follow-up of approximately 75 months. Among cardiovascular outcomes, AF was most common (IR, 18.99/1000 PY), followed by HF (IR, 10.52/1000 PY), stroke (IR, 8.23/1000 PY), and ACS (5.66/1000 PY) (Fig. 3a). The risk of AF was higher than that of all other outcomes at all timepoints and began to deviate from the other curves at approximately 20 months, while curves for stroke, ACS, and HF were similar throughout the end of follow-up (Appendix C, Fig. C3a). The cumulative incidence curve for kidney failure remained relatively flat and near 0 throughout follow-up.
Fig. 3
Outcomes: VID. a Incidence rates of primary outcomes, SGLT2i cohort. b Cumulative incidence of secondary outcomes, SGLT2i cohort. c Incidence rates of primary outcomes, GLP-1 RA cohort. d Cumulative incidence of secondary outcomes, GLP-1 RA cohort. CI confidence internal, eGFR estimated glomerular filtration rate, GLP-1 RA glucagon-like peptide-1 receptor agonists, IR incidence rate, SGLT2i sodium-glucose cotransporter 2 inhibitors, VID Valencia Health System Integrated Database
At 36 months, the risk of eGFR declines ≥ 30% from baseline was 26% while risk for declines ≥ 57% was 3% (Fig. 3b). Over the entire follow-up period, the risk of serum potassium values > 5.5 mmol/l was much higher than risk of values > 6.0 mmol/l, which remained relatively low (36 months: 17% and 5%, respectively) (Fig. 3b).
GLP-1 RA CohortIn the GLP-1 RA cohort, the IR of kidney failure was 1.68 events per 1000 PY during follow-up of approximately 95 months. Among cardiovascular outcomes, AF was most common (IR, 21.93/1000 PY), followed by HF (IR, 13.76/1000 PY), stroke (IR, 9.07/1000 PY), and ACS (IR, 7.31/1000 PY) (Fig. 3c). The risk of AF was higher than all other outcomes at all timepoints; the curve for HF showed a similar pattern to that for AF, while the curves for stroke and ACS were almost identical throughout follow-up (Appendix C, Fig. C3b). The curve for kidney failure remained relatively flat and near 0.
At 36 months, risk for declines in eGFR ≥ 30% from baseline was 24% compared with 3% for declines ≥ 57%, and the risk of serum potassium values > 5.5 mmol/l was 20% compared with 7% for values > 6.0 mmol/l (Fig. 3d).
Optum® EHRSGLT2i CohortIn the SGLT2i cohort, the IR of kidney failure was 6.33 events per 1000 PY during follow-up of approximately 80 months. Among cardiovascular outcomes, AF was most common (IR, 26.28/1000 PY), followed by HF (IR, 13.01/1000 PY), ACS (IR, 9.54/1000 PY), and stroke (IR, 5.20/1000 PY) (Fig. 4a). The cumulative incidence curves for AF and HF were of similar magnitude and were higher than those for all other outcomes throughout follow-up (Appendix C, Fig. C4a). The curves for stroke and kidney failure were superimposed until 60 months of follow-up, while the curve for ACS was slightly greater than that for kidney failure at all timepoints.
Fig. 4
Outcomes: Optum® EHR. a Incidence rates of primary outcomes, SGLT2i cohort. b Cumulative incidence of secondary outcomes, SGLT2i cohort. c Incidence rates of primary outcomes, GLP-1 RA cohort. d Cumulative incidence of secondary outcomes, GLP-1 RA cohort. CI confidence internal, eGFR estimated glomerular filtration rate, GLP-1 RA glucagon-like peptide-1 receptor agonists, IR incidence rate, Optum® EHR Optum® de-identified Electronic Health Record data set, SGLT2i sodium-glucose cotransporter 2 inhibitors
At 36 months, the risks of eGFR declines ≥ 30% and ≥ 57% from baseline were 31% and 7%, respectively, and the risks of serum potassium values > 5.5 mmol/l and > 6.0 mmol/l were 10% and 3%, respectively, at 36 months (Fig. 4b).
GLP-1 RA CohortIn the GLP-1 RA cohort, the IR of kidney failure was 12.95 events per 1000 PY during follow-up of approximately 95 months. Among cardiovascular outcomes, AF (IR, 29.37/1000 PY) and HF (IR, 16.66/1000 PY) were most common, and the IR for ACS (IR, 10.21/1000 PY) was higher than that for stroke (IR, 5.41/1,000 PY) (Fig. 4c). During the follow-up period, the cumulative incidence curves for AF and HF were very similar and were higher than those for all other outcomes throughout follow-up (Appendix C, Fig. C4b). The curves for ACS and kidney failure were also similar and were higher than that for stroke throughout follow-up.
At 36 months, the risk of eGFR declines ≥ 30% from baseline was 35% at 36 months, while risk for declines ≥ 57% was 9%, and the risks of serum potassium values > 5.5 mmol/l and > 6.0 mmol/l were 12% and 4%, respectively (Fig. 4d).
Comments (0)