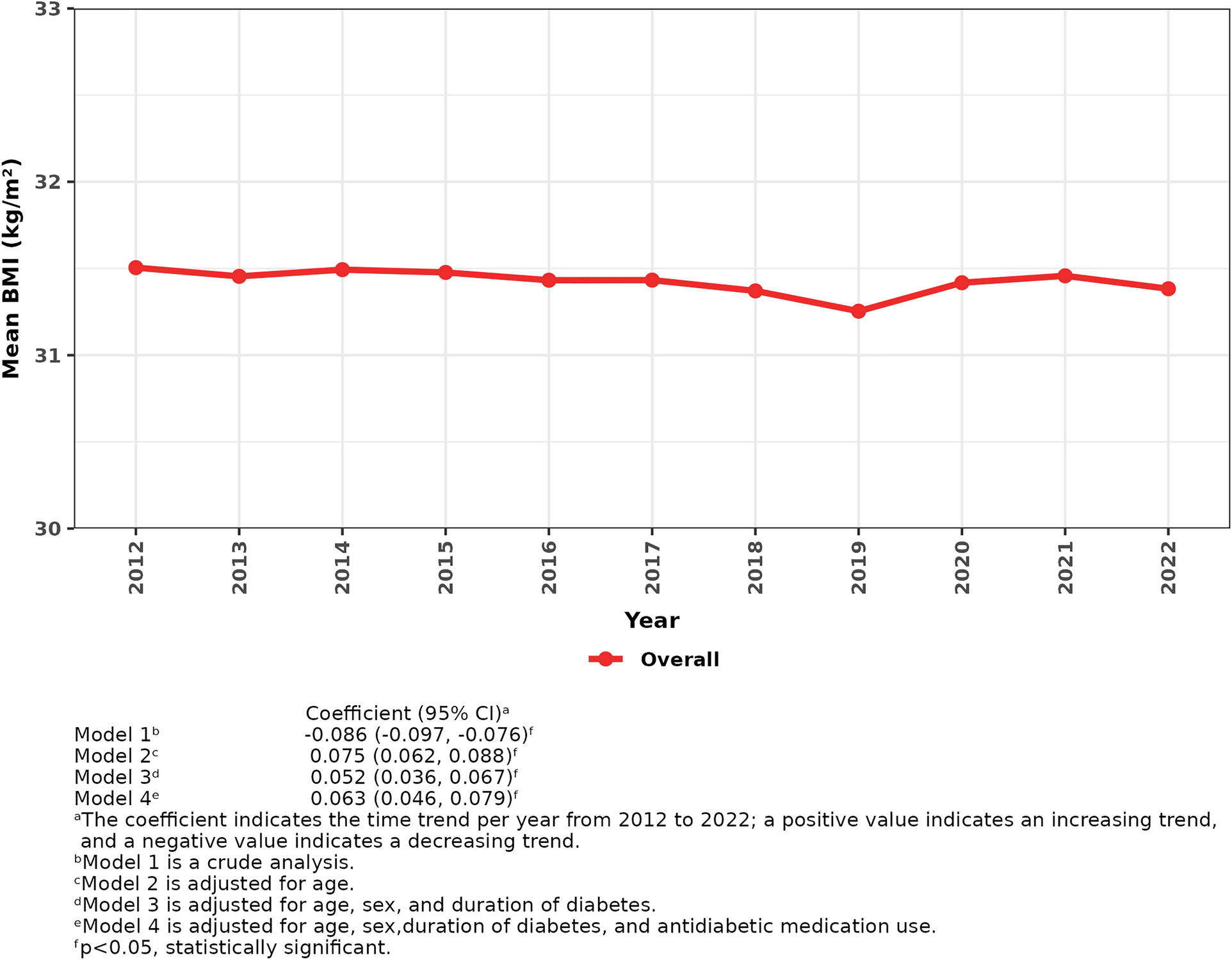
This study demonstrated a slightly declining time trend in the unadjusted BMI among the study patients, but the time trend became increased after accounting for age. Age-stratified analysis of BMI followed a comparable pattern, showing increasing time trends of BMI particularly in the younger age groups. Furthermore, patients with higher BMI values had higher HbA1c levels and were less likely to achieve the HbA1c target. However, HbA1c control improved over time in patients with the highest level of obesity, along with a greater increase in new antidiabetic medication use compared with those with underweight or normal weight.
A slightly declining time trend in the unadjusted BMI increased after adjusting for age, reflecting the aging effect and lower BMI values among the aged patients. The age impact in BMI trends was evident in the age-stratified analysis, with increasing time trends of BMI in those aged 45–64 even after controlling for sex and diabetes duration. Furthermore, the increasing time trend of BMI among all the study patients was observed after adjusting for age, sex, diabetes duration, and antidiabetic medication use. This finding aligns with the current BMI and obesity trends in the general population in Finland where increasing trends are seen especially among working age population [2]. Our findings suggest that weight management among patients with T2D, especially younger patients, is unsatisfactory and poses a challenge, given the American Heart Association’s and European Diabetes Association’s recommendation for individuals with diabetes to achieve and maintain a BMI of ≤ 25 kg/m2 [21, 22].
Consistent with our finding of an increasing time trend of age-adjusted BMI (31.3–31.5 kg/m2), a fixed cohort study in Hong Kong of patients with T2D diagnosed on or before 30 September 2010 showed that the age-adjusted mean BMI slightly increased among the patients from 2010 to 2019 (25.0–25.4 kg/m2) [9]. Importantly, these two studies suggested suboptimal weight control among patients with T2D, although the average BMI was lower in a Hong Kong Chinese study than that in this study. The BMI cutoff points for defining obesity vary between East Asians (≥ 25 kg/m2) and white patients (≥ 30 kg/m2) [16]. East Asians have a higher percentage of body fat (3–5%) compared with white patients with the same BMI [23].
Our finding of increasing time trends of BMI in those aged 45–64 aligns with the results from a study of annual patients with T2D from 2012 to 2019 in America [8]. Note that the time trend of BMI observed in the American study was unadjusted, whereas sex and diabetes duration were accounted for in our analyses. However, in our study, the increasing time trends of BMI in patients aged 45–54 and 55–64 either disappeared or shifted to a decline with further adjustment for antidiabetic medication use despite an increasing time trend of BMI among all the study patients with adjustment for age, sex, diabetes duration, and antidiabetic medication use. We observed a declining time trend of BMI among the study patients using new antidiabetic medications. However, the increased use of them seemed not to significantly affect the time trend of BMI overall. Despite being observed in trials [24, 25], the weight reduction associated with the new antidiabetic medications might not be easily seen at the patient population level. Existing studies have not considered the impact of the diabetes duration and antidiabetic medications on the time trend of BMI. Therefore, future studies are required to account for potential confounders when examining the time trend of BMI among patients with T2D, as well as across different age and antidiabetic medication groups.
Overall, higher HbA1c levels and lower percentages of patients achieving the HbA1c target were observed in the higher BMI categories between 2012 and 2022, indicating worse glycemic control associated with obesity. These findings are reasonably obvious as insulin resistance is usually present in patients with T2D and is strongly associated with obesity [26]. This further impairs glucose uptake in the liver, skeletal muscle, and adipose tissue, resulting in elevated blood glucose levels in patients with T2D and obesity. Despite slightly more new antidiabetic medication users (without insulin) across different obesity categories, their glucose control was still worse than that of those without obesity. High adherence is important to ensure the effectiveness of pharmaceutical treatment. Although the proportion of adherent patients in this study is uncertain, medication adherence among Finnish patients can be considered as good. A recent study involving 1,814,591 individuals from Finnish nationwide registries revealed that at least 80% of participants were considered as good adherers to statins, blood pressure medications, antiplatelets, breast cancer medications, and direct oral anticoagulants [27]. Also, other factors such as healthy lifestyles, especially physical activity and healthy diet, help achieve good glycemic control [28]. However, facilitating lifestyle counseling for patients with T2D is challenging, resulting in most patients primarily being treated with diabetes medications [29]. Data on lifestyle changes are unavailable in the EHRs; therefore, we could not assess the difference in lifestyle between the BMI categories. Taken together, further research accounting for medication adherence and lifestyle is required to verify our findings.
When examining time trends of HbA1c control, the HbA1c control improved among the patients with the highest level of obesity over time, after accounting for antidiabetic medication use. This improvement coincided with a greater increase in new antidiabetic medication use over time in patients with the highest level of obesity compared with those with underweight or normal weight. These findings suggest that patients with the highest levels of obesity may achieve improved glycemic control despite marked insulin resistance, possibly owing to the efficacy of newer pharmacological agents such as GLP-1 analogues and SGLT2 inhibitors. These medications act through diverse mechanisms. For example, GLP-1 analogues stimulate insulin secretion only in the presence of elevated blood glucose and suppress glucagon release by acting on incretin hormones from the gut [30]. It is widely known that GLP-1 analogues and SGLT2 inhibitors, as new antidiabetic medications, effectively regulate glucose. Following the national reimbursement reform implemented on 1 January 2017, the reimbursement rate for antidiabetic medicines other than insulins decreased from 100% to 65% [31, 32]. Additionally, for the patients to receive special reimbursement for GLP-1 analogues, they must first try other antidiabetic medications, have a BMI ≥ 30 kg/m2, and have their diabetes confirmed by the Social Insurance Institution [33].
The HbA1c control remained constant over time among patients with lower levels of obesity, while it deteriorated over time among patients with underweight or normal weight after accounting for antidiabetic medication use. These findings highlight that patients with lower levels of obesity, as well as those who are underweight or of normal weight, may require greater attention regarding the intensification of glycemic control therapies. Additionally, the deterioration of HbA1c control over time among patients with underweight or normal weight may be partially because treating hyperglycemia in T2D has less strict targets for the aged patients to avoid hypoglycemia, according to the Finnish Current Care Guidelines [5]. In the aged, hypoglycemia leads to cognitive impairment, serious falls, and death [34]. Patients with underweight or normal weight in this study were older than those in the other BMI groups from 2012 to 2022 (data not shown).
The influence of BMI on HbA1c control has been investigated in previous studies. Consistent with our findings, an American study of patients with diabetes between 2009 and 2011 demonstrated that the patients with overweight or obesity had a higher probability of having HbA1c ≥ 7% (≥ 53 mmol/mol) than those with normal weight [35]. By contrast, another American study of patients with T2D between 1999 and 2006 reported a higher HbA1c level in the patients with normal weight, compared with those with overweight or obesity [36]. The inconsistent findings between these two studies are likely due to different data sources. The first one used electronic medical data from the physician practice setting, while the second one used survey data. The collection methods of survey data inherently carry limitations that may introduce sampling error, measurement error, and reporting bias, potentially leading to inaccuracy in assessing the relationship between BMI and HbA1c control. Additionally, a recent Indian study has demonstrated no difference in HbA1c levels across different BMI categories among patients with newly diagnosed T2D, measured at the time of diagnosis [13]. Inconsistent results from prior studies arise from cross-sectional design, making it challenging to establish a reliable relationship between obesity and suboptimal glycemic control. With respect to subsequent follow-up analyses, two recent retrospective studies of annual cohorts have demonstrated that patients with T2D and obesity exhibit higher HbA1c levels or are less likely to reach the HbA1c target than those with T2D and underweight or normal weight [8, 10]. Of note, this estimated association might be biased without considering diabetes duration. T2D is a progressing disease, and its duration is associated with clinical outcomes [37]. Unlike previous studies, this study incorporates potential confounders including age, sex, diabetes duration, and antidiabetic medication use when estimating the association between BMI and HbA1c control.
The inadequate control of BMI among patients with T2D observed here is a common finding [3, 38]. Making dietary and physical activity changes in T2D self-management is insufficient. A meta-analysis including 16 randomized control trials has reported that lifestyle intervention (e.g., increased physical activity, reduced caloric intake) is beneficial for weight loss in patients with T2D [39]. However, in real-life settings, the support for lifestyle changes quite often remains modest or does not exist at all [40]. New antidiabetic medications such as SGLT2 inhibitors and GLP-1 analogues support the weight management [41]. In this study, approximately 90% of patients with T2D received pharmaceutical treatments. At the beginning of the study period, approximately 15% of patients used insulin and only a few had new medications in use. However, the increase in the use of new antidiabetic medications without insulin over time did not lead to a decline in mean BMI. The effect of antidiabetic medications may only be inadequate if the patient does not simultaneously receive appropriate support for dietary and other lifestyle changes [42].
Strengths and Limitations
The large sample size and long study period enabled us to perform trend analyses and ensured the precision of the association between BMI and HbA1c control. All patients with T2D from 2012 to 2022 in the North Karelia region were included to ensure minimal selection bias. BMI measurements conducted in health services minimized recall bias. Despite these advantages, our study had some limitations. First, BMI measurements were not complete or not adequately recorded in the EHRs in the first years of the study period. Second, we could not consider the effect of self-care on both weight management and glycemic control because of lacking information on lifestyle factors in the EHRs, which are based on administrative register data. Third, adherence to antidiabetic medications cannot be determined in this study, which could result in potential bias. Finally, the analytic sample was limited to patients with T2D in one region in Finland, which may affect the generalization of our findings because of region-specific factors, including genetics, socioeconomic conditions, and environmental influences. Thus, additional studies in other population groups are recommended to generalize our results.

Comments (0)