
Remember me
Across the ONWARDS trials, 2172 participants (1882 with T2D; 290 with T1D) were randomised to receive icodec and 2175 (1883 with T2D; 292 with T1D) were randomised to receive once-daily comparators. The number of participants hospitalised during the trial period were similar between treatment groups (icodec, n = 152 [7.0%]; once-daily comparators, n = 156 [7.2%]) (Table 1). The baseline characteristics of hospitalised participants were broadly similar between treatment groups, as were the number of hospitalisations and the median duration of hospital stay (icodec, 5.0 days; once-daily comparators, 6.0 days). The three most common reasons for hospitalisation among participants receiving icodec were COVID-19, COVID-19 pneumonia, and pneumonia; among participants receiving once-daily comparators, the three most common reasons were COVID-19, acute myocardial infarction, and COVID-19 pneumonia. Despite hospitalisation, most participants completed the end-of-trial visits without permanent trial product discontinuation (icodec, n = 129 [84.9%]; once-daily comparators, n = 141 [90.4%]). Adverse events were the most common reason for permanent trial product discontinuation at any point during the trial period in hospitalised participants (icodec, n = 17 [11.2%]; once-daily comparators, n = 10 [6.4%]) (Table 1). All 27 adverse events reported as reasons for discontinuation of the trial product were different; no clustering or trends were observed in the type of adverse events reported.
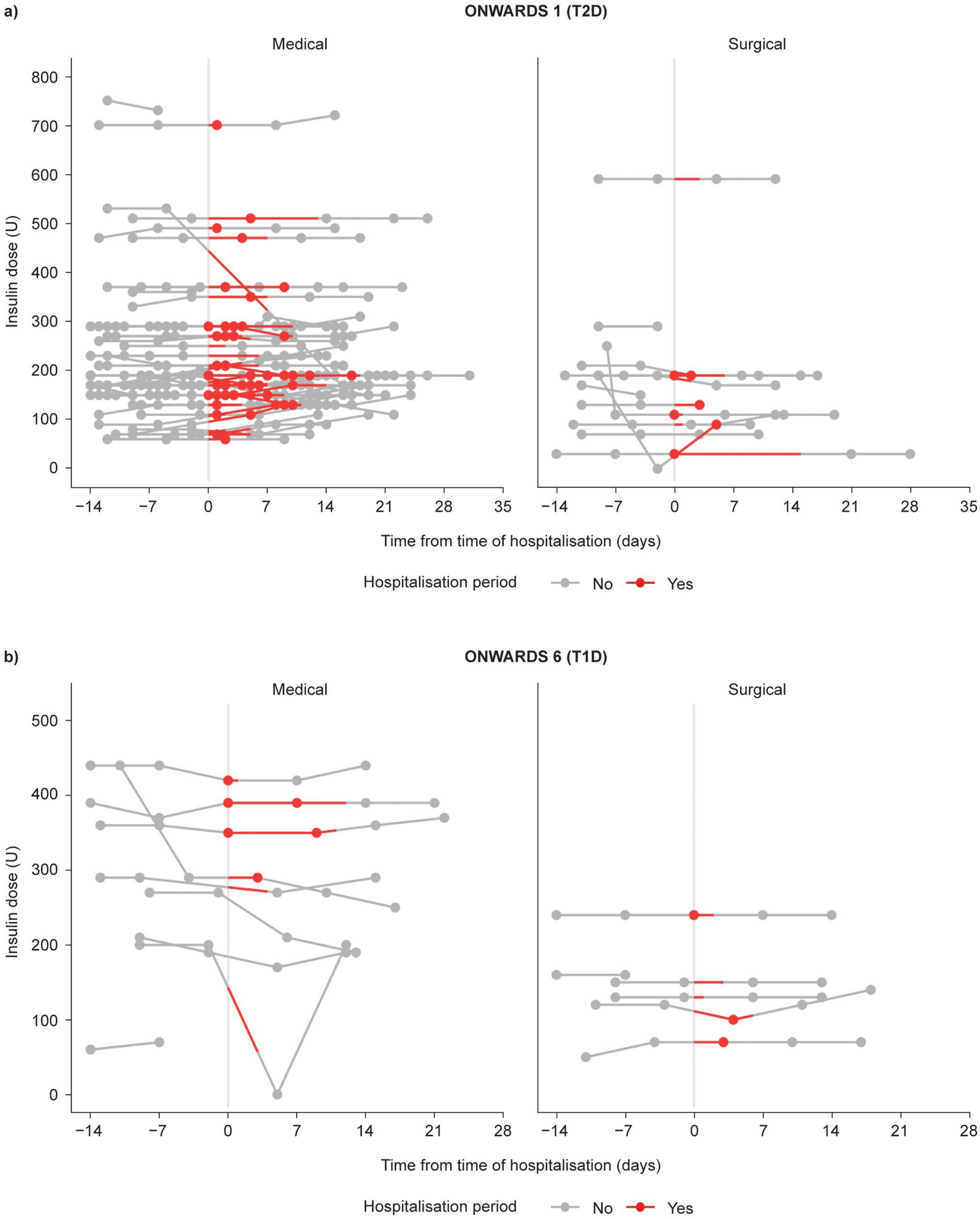
Table 1 Overview of participants who were hospitalisedIcodec Dose During HospitalisationFor participants receiving icodec who were hospitalised, the basal insulin dose remained fairly stable and uninterrupted during hospitalisation; median icodec dose was the same before hospitalisation and after discharge (190 U) (Fig. 1 and Supplementary Figure S2). In the icodec group, 82.5% of participants received icodec according to their usual schedule while in hospital. The majority (> 90%) of participants hospitalised while receiving icodec continued icodec treatment according to their usual schedule after discharge. For 176 [97.8%] of 180 hospitalisation cases in the icodec group, no additional daily basal insulin administration was reported during hospitalisation. In the once-daily comparator group, 159 [91.4%] of 174 hospitalisation cases required no additional daily basal insulin during hospitalisation. Bolus insulin was administered in 24 cases in the icodec arm (two in T1D and 22 in T2D) and 19 cases in the comparator arm (three in T1D and 16 in T2D). All those participants receiving an additional daily basal dose also received bolus insulin. One T2D hospitalisation case in the comparator arm received a pre-mixed insulin during hospitalisation (Supplementary Table S1).
Fig. 1
Icodec administration in ONWARDS 1 (a) and ONWARDS 6 (b) from 14 days before hospitalisation to 14 days after discharge. Icodec insulin icodec, T1D type 1 diabetes, T2D type 2 diabetes, U units
Glycaemic ControlAcross trials, few SMBG measurements were recorded and documented in the trial eDiary by participants during hospitalisation. Overall, there were no large fluctuations in SMBG levels before and after the hospitalisation period, and values were comparable between treatment groups (Fig. 2). For all participants with T2D, observed SMBG levels increased slightly after discharge, before returning to levels comparable to those recorded before hospitalisation by 3–4 weeks after discharge (Fig. 2A). For participants with T1D who were receiving icodec, SMBG levels at discharge seemed comparable to those observed before hospitalisation, whereas for participants receiving once-daily comparators, SMBG levels appeared briefly increased after discharge before returning to levels comparable to those observed before hospitalisation (Fig. 2B).
Fig. 2
SMBG measurements recorded before, during, and after the hospitalisation period by participants in ONWARDS 1–5 (a) and ONWARDS 6 (b). Observed data shown as mean of all SMBG values recorded at the time point ± SEM. Horizontal grey lines at 7.2 mmol/l represent the prebreakfast SMBG target above which an increase in basal insulin dose was recommended. SMBG was assessed using a glucose meter as plasma equivalent values of capillary whole blood glucose. aGraphs present pooled data from ONWARDS 1–5. bONWARDS 1 and 4: glargine U100; ONWARDS 2, 3, and 6: degludec; ONWARDS 5: degludec, glargine U100, or glargine U300. Icodec insulin icodec, SEM standard error of the mean, SMBG self-measured blood glucose, T1D type 1 diabetes, T2D type 2 diabetes
For hospitalised participants with T2D or T1D, mean HbA1c levels remained relatively stable over the assessed time points (near hospitalisation, after discharge, and at end of trial) regardless of treatment group (Table 2).
Table 2 HbA1c levels at trial baseline, time of hospitalisation, after discharge, and at the end of the treatment period for hospitalisations that occurred during ONWARDS 1–5 (T2D) and ONWARDS 6 (T1D)Participant-Reported HypoglycaemiaIn the T2D population, the observed rate of combined clinically significant or severe hypoglycaemia in the icodec group during hospitalisation was 1.33 episodes per PYE, which was within the range of rates observed during the 4-week period before hospitalisation and after discharge (0.82–1.73 episodes per PYE) (Table 3). Similarly, in the once-daily comparator group, the observed rates of combined clinically significant or severe hypoglycaemia were low during the 4 weeks before hospitalisation, during hospitalisation, and during the 4 weeks after discharge (ranging from 0.27–0.61 episodes per PYE). During hospitalisation, one icodec participant with T2D (0.6%) reported five episodes of clinically significant hypoglycaemia, with a resultant observed rate of combined clinically significant or severe hypoglycaemia of 1.33 episodes per PYE during this period. The same participant later experienced a serious adverse event of hypoglycaemia while hospitalised but was unable to record the episode in the eDiary owing to their rapidly worsening condition; therefore, the event was not included in this analysis. Specifically, this participant had an amputation of the right foot due to a trophic ulcer, and further developed irregular tachycardia. Following transfer to an intensive care unit, the participant’s condition worsened owing to sepsis and acute kidney damage, before death. No severe hypoglycaemic episodes were reported by participants with T2D in the icodec group; in the once-daily comparator group, one severe hypoglycaemic episode was reported during hospitalisation.
Table 3 Participant-reported hypoglycaemia before, during, and after the hospitalisation period in ONWARDS 1–5 (T2D) and ONWARDS 6 (T1D)Hypoglycaemia data for hospitalised participants with T1D are also presented in Table 3. The observed rates of combined clinically significant or severe hypoglycaemia during hospitalisation were 11.66 and 4.97 episodes per PYE for icodec and OD comparators, respectively, and within the range of the rates observed during the 4 weeks before hospitalisation and the 4 weeks after discharge (icodec: 11.15–20.79 episodes per PYE; OD comparator: 2.61–5.31 episodes per PYE), with rates trending lower following discharge from hospital.
During hospitalisation, two participants with T1D in the icodec group reported two episodes of clinically significant hypoglycaemia, and one participant with T1D in the once-daily comparator group reported one such hypoglycaemic episode.
Of those participants receiving icodec who were hospitalised, four severe hypoglycaemic episodes were reported in three participants with T1D during hospitalisation; in the once-daily comparator group, one participant reported one severe hypoglycaemic episode during hospitalisation (Table 3). For all participants with T1D in both treatment groups who reported an episode of severe hypoglycaemia during hospitalisation, severe hypoglycaemia occurred on the day of admission and was either the main reason, or a secondary reason for hospitalisation; per the clinical trial reports, all episodes were managed similarly according to usual standard of care with administration of oral carbohydrates, glucagon or intravenous glucose, irrespective of treatment group. No severe hypoglycaemic episodes were reported either 4 weeks before or 4 weeks after the hospitalisation period in any hospitalised participant with T1D in either treatment group.
Case VignettesWe present three cases on participants (two with T2D and one with T1D) from the icodec treatment group who were hospitalised during the trial, to illustrate icodec use during and around hospitalisation.
Case 1: This individual with T2D had a history of atrial fibrillation. The patient started treatment with icodec 70 U as part of the phase 3a icodec clinical trial development programme. At trial screening, the participant was receiving dulaglutide, gliclazide, metformin, and pioglitazone. During the trial treatment period, the patient was hospitalised for 6 days after presentation of persistent chest discomfort and subsequent confirmation of acute non-ST segment elevation myocardial infarction. An angiogram and percutaneous coronary intervention were performed without incident during hospitalisation. The patient received icodec 70 U 2 days before hospitalisation, and 70 U again 7 days after the previous dose and after discharge; the patient did not receive an icodec dose during hospitalisation. During hospitalisation, prebreakfast SMBG values remained steady at ~ 7 mmol/l (~ 126 mg/dl). The patient recovered and was discharged without incident.
Case 2: This patient living with long-standing T2D had several comorbidities, including dyslipidaemia, cataracts, hypertension, and osteoarthritis. The patient presented with worsening knee degenerative joint disease and was hospitalised for a scheduled total knee arthroplasty. At the time of surgery, they were receiving icodec 200 U as part of a basal-bolus regimen in the phase 3a icodec clinical trial development programme. The patient received icodec 200 U 1 day before hospitalisation, and 200 U again 7 days after the previous dose, when they had been discharged (i.e. icodec dose was not changed or interrupted). Concomitant medications included aspart and semaglutide. On the day of hospitalisation, the patient’s prebreakfast SMBG value was stable and similar to the days leading up to hospitalisation at ~ 6 mmol/l (~ 106 mg/dl). The morning after admission, the prebreakfast SMBG value increased to ~ 11 mmol/l (~ 196 mg/dl) before decreasing to ~ 5 mmol/l (~ 90 mg/dl) after discharge. The prebreakfast SMBG value increased steadily in the 7 days after discharge to ~ 7 mmol/l (~ 126 mg/dl). The procedure was reported as being without incident; the patient was discharged the day after hospital admission.
Case 3: At the time of hospitalisation, this individual with T1D was receiving icodec 350 U along with insulin aspart for mealtime coverage as part of a basal-bolus regimen in the phase 3a icodec clinical trial development programme. The previous basal insulin was daily insulin degludec. The patient had several comorbidities, including microvascular disease, obesity, myasthenia gravis and non-alcoholic fatty liver disease. During the trial, the patient was hospitalised for 11 days with COVID-19, confirmed by PCR test. On the day of hospitalisation, the patient was examined using computerised tomography which showed bilateral viral COVID-19 pneumonia. While hospitalised, the patient was treated with acetylcysteine, omeprazole ceftriaxone, dexamethasone, enoxaparin sodium, and favipiravir. Treatment with icodec remained unchanged during the period of hospitalisation. The patient was discharged with resolved pneumonia. Following administration of 350 U of icodec on the day of admission, the patient received another dose of 350 U 9 days later, during their hospital stay, and another 360 U 6 days after the previous dose, following discharge (i.e. icodec dose was not changed or interrupted during hospitalisation). During hospitalisation, bolus insulin was maintained as insulin aspart 4–10 U for breakfast, 3–13 U for lunch and 4–13 U for dinner, which are within similar ranges as before and after the hospital stay. During hospitalisation, two correction bolus doses were administered (2 U and 4 U separately) on two separate days following breakfast. Pre-breakfast SMBG fluctuated between 5–13.4 mmol/l during hospitalisation, which is similar to the levels measured before and after hospitalisation. Other reported SMBG values ranged between 4–20 mmol/l during the hospital stay. No level 2 or level 3 hypoglycaemia events were reported during the hospitalisation period.
Comments (0)