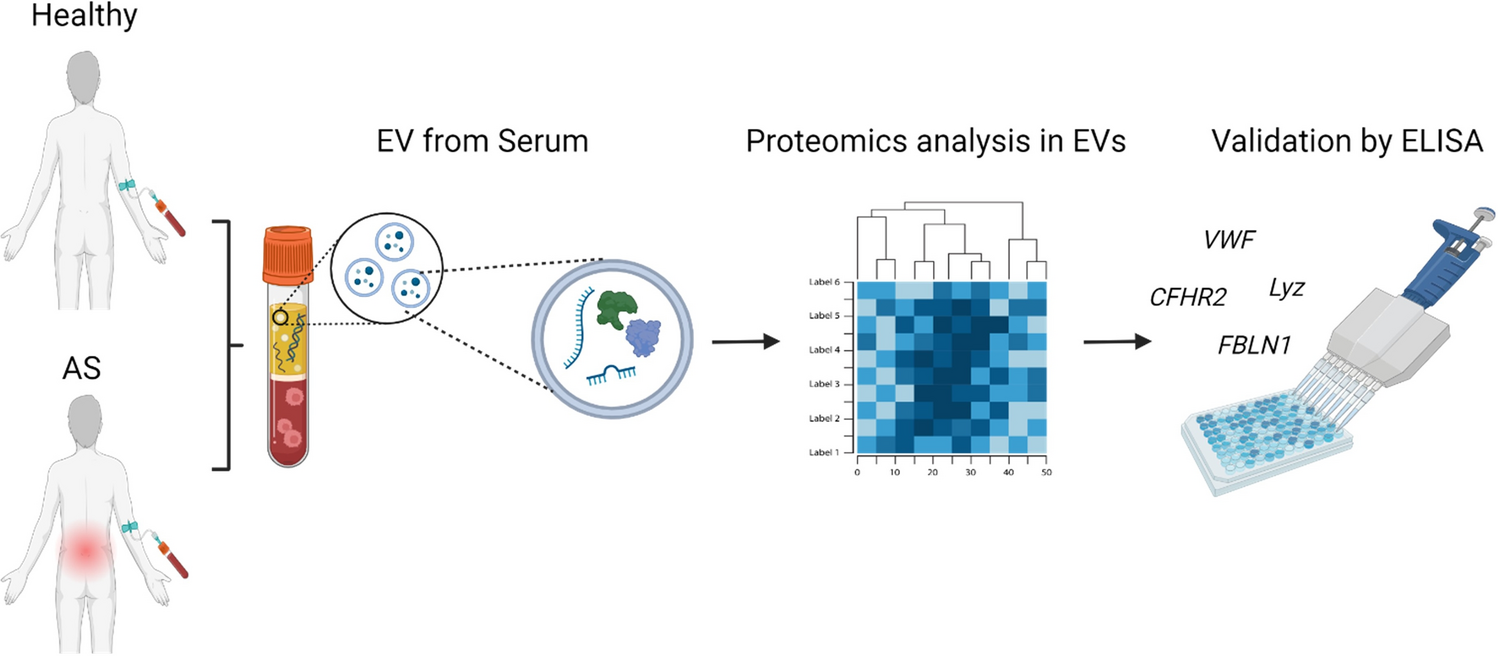
AS is a chronic progressive systemic disease that usually presents with typical spinal stiffness and is characterized by chronic inflammation of the sacroiliac joints and spine and the involvement of peripheral joints, eyes, heart, and intestines [15, 16]. Bone diseases are generally caused degeneratively via inflammatory reactions due to aging (e.g., degenerative arthritis), or by specific hormonal disorders due to acquired problems (e.g., osteoporosis, bone disease) [1, 17]. Meanwhile, it is assumed that genetic abnormalities, infection, and immune-inflammatory responses are involved in AS development, but the specific cause of the disease has not yet been revealed [18,19,20]. One of the main symptoms of AS is inflammatory back pain, which gradually begins in the lumbar or lumbosacral region and, in some cases, is intermittently accompanied by arthritis in the knees and ankles [21,22,23]. Because this pain is generally vague and undergoes repeated cycles of worsening and improving, it is difficult to distinguish from general back pain [24, 25]. Additionally, AS may feature extra-articular-related symptoms such as uveitis, psoriasis, and inflammatory bowel disease, and may in rare cases be accompanied by cardiomyopathy, aortic valve failure, and interstitial pneumonia [26,27,28,29,30]. Although the HLA-B27 gene is known to be associated with AS development, there is a need for further research to elucidate the precise etiology of the disease and to identify reliable biomarkers for its early diagnosis [31,32,33]. Recently, as new knowledge has been accumulated about this disease’s course and treatment, the issue of early diagnosis has become important as it has been shown that early treatment is effective at preventing AS progression. However, the diagnosis of AS is generally based on the patient’s symptoms, medical history, and radiological findings of the sacroiliac joint and spine. Radiological abnormalities are typically detected only in patients with advanced disease, complicating early diagnosis [34]. AS, a chronic inflammatory condition primarily affecting the spine and sacroiliac joints, presents significant diagnostic challenges [34, 35]. EVs have been reported as potential biomarkers for the diagnosis of specific diseases. In the case of AS, some studies have aimed to develop diagnostic markers based on the expression profiles of genes within EVs [36, 37]. However, considering clinical applicability, it is also valuable to investigate biomarkers based on protein expression profiles in EVs. Against this background, this study was implemented to identify novel biomarkers in EVs derived from the serum samples of AS patients, with the goal of improving the utility and timeliness of AS diagnosis.
In the present study, serum-derived EVs were isolated and characterized in both normal controls and AS patients. The isolated particles were confirmed to be EVs by TEM, NTA, and flow cytometry. MicroRNAs or proteins in EVs have been studied using bioinformatic methods. Therefore, in this study, we sought to identify potential AS diagnostic biomarkers by analyzing the expression of specific proteins in EVs derived from AS patient serum compared with those from normal control serum. The proteomic analysis results indicated that FBLN1, VWF, CFHR2, and LYZ were highly expressed in the EVs derived from AS patient serum compared with those from the normal control group.
FBLN are ECM-secreted glycoproteins, notable for their two distinct structural features: a series of calcium-binding epidermal growth factor (cbEGF)-like modules and a unique domain in the C-terminal region. To date, eight family members have been identified, categorized into long (fibulin-1, -2, -6, and -8) and short types (fibulin-3, -4, -5, and -7) [38]. The role of fibulin-1 has attracted increasing attention in a variety of human cancers. However, studies performed to date show contradictory findings regarding fibulin-1’s function across different tumor tissues. While the majority of research supports fibulin-1’s tumor-suppressive capabilities[39], further investigations are necessary to elucidate its potential association with AS. VWF is a crucial multimeric glycoprotein synthesized exclusively in endothelial cells and megakaryocytes, which plays a vital role in primary hemostasis. VWF biosynthesis involves complex post-translational modifications across different cell organelles, starting in the endoplasmic reticulum and continuing in the Golgi apparatus. This process results in the formation of multimers with over 300 glycan structures, which are essential for the recruitment of platelets at sites of vascular injury [40]. Recent studies have expanded the understanding of VWF’s role beyond hemostasis. VWF is implicated in various physiological processes, including vascular permeability, inflammation, and angiogenesis. Notably, the absence of VWF, as observed in type 3 von Willebrand disease (VWD), correlates with enhanced vascularization and severe clinical manifestations such as gastrointestinal bleeding due to vascular malformations [41]. VWD is recognized as the most common inherited bleeding disorder, presenting significant diagnostic and subclassification challenges due to the wide range of plasma VWF levels in the normal population and VWF’s diverse physiological roles [42]. A study on biomarkers related to VWF and AS reported that the expression of VWF was upregulated in AS patient serum [43]. However, studies on VWF protein in EVs and AS disease have not been reported. The CFHR protein family comprises CFHR1 to CFHR5, each of which binds to the complement component C3b. Diseases related to this family have been reported, such as atypical hemolytic uremic syndrome (aHUS), C3 glomerulopathies [C3 glomerulonephritis (C3GN), dense deposit disease, and CFHR5 nephropathy], IgA nephropathy, age-related macular degeneration, and systemic lupus erythematosus [44]. To the best of our knowledge, no studies on disease-specific biomarkers related to the CFHR protein family and AS have been reported.
LYZ, a protein produced and released by monocytes and macrophages, is prevalent in various body tissues and secretions, notably saliva [45]. It endows saliva with antibacterial properties and plays a role in antiviral defense. Studies have identified a negative correlation between the concentration of lysozyme and stress exposure. Additionally, lysozyme expression varies significantly across different diseases; it is notably present in macrophages and giant cells in sarcoidosis and Crohn’s disease granuloma, but is expressed minimally in foreign body granulomas. This variation suggests a link between lysozyme level and disease activity. In the human airways, lysozyme is a major antimicrobial factor, with its activity being reported to positively correlate with neutrophil count in bronchoalveolar lavage fluid in cystic fibrosis patients, but not with bacterial colony count. These observations indicate that certain types of cell-mediated immunity may influence lysozyme activity [46]. However, the relationship between lysozyme and AS remains unclear. The results of the pathway analysis suggest that the four additional proteins, along with the known AS biomarkers CRP, HLA-B27, ESR, and cytokines, could serve as new biomarkers closely related to the inflammatory response, platelet activation, coagulation, and extracellular matrix (ECM)-receptor interaction which are key mechanisms in AS pathogenesis (Table 3).
Table 3 Functional annotation tableHere, we observed that FBLN1, VWF, CFHR2, and LYZ were expressed at low levels in controls, but showed significantly elevated expression in patients with AS. Utilizing LC–MS/MS, we confirmed the upregulation of these proteins in the AS patient group compared with the level in the control group through ELISA. The expression levels of FBLN1, VWF, CFHR2, and LYZ were significantly elevated in the AS group. These findings suggest that FBLN1, VWF, CFHR2, and LYZ could serve as novel biomarkers for the diagnosis of AS. We also successfully isolated EVs from human serum and analyzed and compared the protein expression patterns in EVs from AS patients and controls. This analysis facilitated the identification of specific protein biomarkers potentially linked to AS. However, this study has several limitations. It represents the initial investigation into exosomal biomarkers for AS, focusing exclusively on patients with a confirmed diagnosis, specifically those in advanced stages, to ensure a clear difference between diseased and healthy individuals. Future research will explore the variation in exosomal biomarkers across different stages of AS. Moreover, it was not possible to determine whether the newly proposed proteins can be distinguished from those in other inflammatory diseases, such as rheumatoid arthritis, psoriatic arthritis, validation in a larger group is necessary before clinical application. The small sample size of 10 patients in this study makes further investigation with a larger cohort necessary. In future studies, we aim to include over 100 AS patients to validate and extend the findings on the exosomal biomarkers identified here. Despite these limitations, this research marks a pioneering step in developing exosomal biomarkers for orthopedic diseases and lays the groundwork for subsequent studies, including verification of the accuracy of these biomarkers and their potential application in clinical trials.





Comments (0)