
Remember me




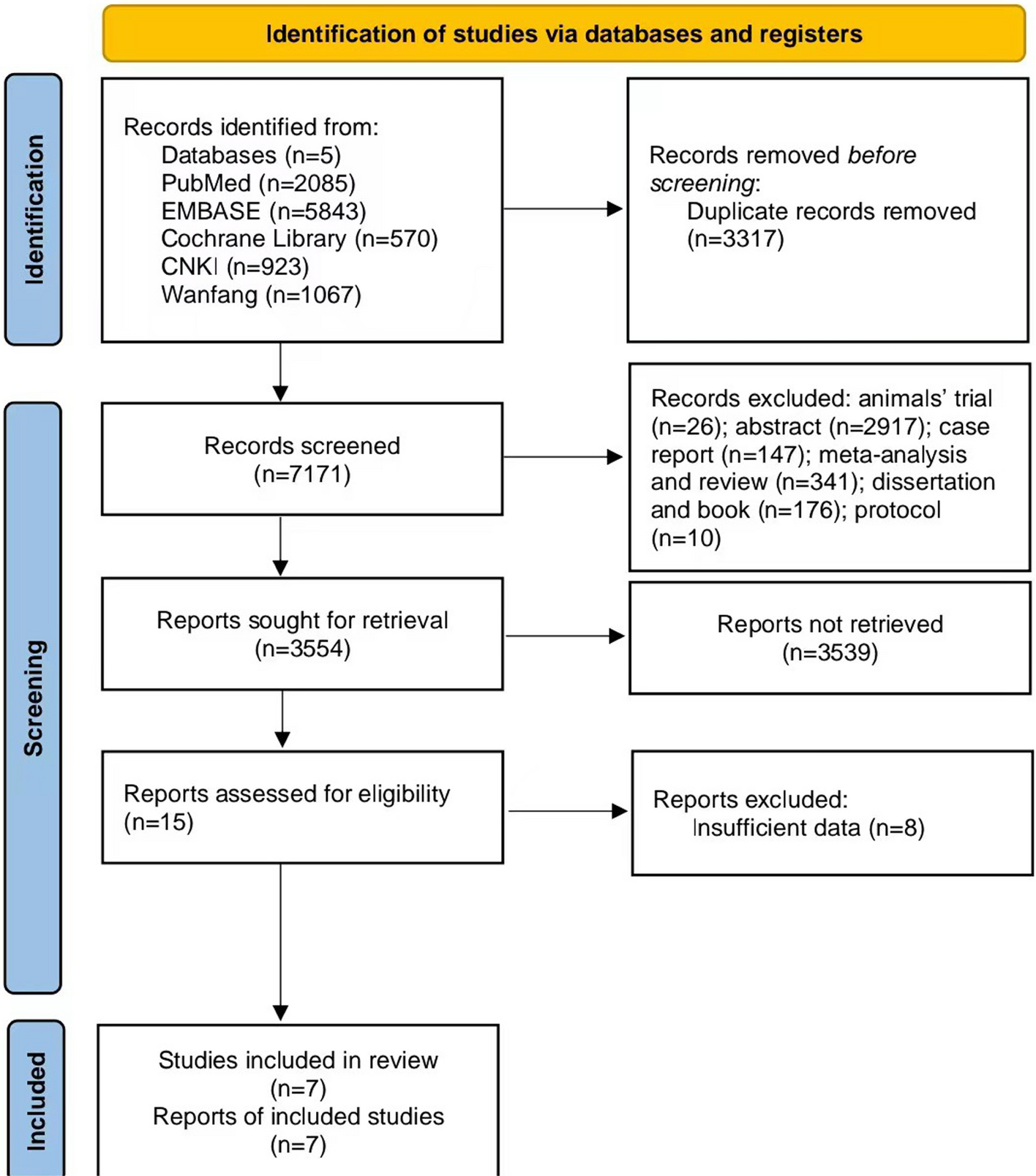
Initially, 1623 potentially relevant titles were identified from the databases. After screening the titles and abstracts, 517 duplicate records were removed. To proceed with a full-text review, 36 conference papers and abstracts were evaluated. The Inclusion/exclusion criteria were applied, excluding studies with unclear or irreproducible results. Ultimately, 17 studies on NK cell therapy efficacy in patients of AML were included in the systematic review after all screening steps were completed [2, 3, 7, 9,10,11, 16, 18, 25,26,27,28,29,30,31,32,33]. Figure 2 illustrates the screening process and exclusion reasons.
Fig. 2
PRISMA flowchart of literature screening and exclusion criteria for NK cell therapy in AML studies. Reason 0: Studies involving non-AML diseases, non-NK cell therapies, or animal/cell line models. Reason 1: Non-original research (letters, meeting abstracts, case reports, narrative/mini-reviews, systematic reviews/meta-analyses, editorials, books/newspapers). Reason 2: Studies with unclear results, methodological flaws, or insufficient data (unless abstract provides analyzable data). Reason 3: Non-English publications
Characteristics of the studiesTable 1 summarizes the baseline characteristics and research methodologies of the 17 clinical studies involving AML patients. Of these, six studies were in Phase I [2, 3, 7, 10, 16, 25], two were in Phase I/II [18, 26], and three were in Phase II [29, 31, 32], while six did not specify their experimental phase [9, 11, 27, 28, 30, 33]. The studies included a total of 402 patients, with an age range of 0.1 to 80 years. The most commonly used intervention was the infusion of NK cells from allogeneic or homologous donors, in some cases combined with chemotherapy or IL-2.
Table 1 Characteristics of the studies included in the systematic review studyThe route of administration was predominantly intravenous (IV), with the dosage of injections varying across studies, ranging from 5 × 106 to 3 × 109 cells per kg. Table 1 also provides additional details regarding the route of injection, NK cell dosage, and combination strategies, including the use of IL-2, IL-12, IL-15, and IL-18 to prime NK cells.
Quality assessmentThe quality assessment results revealed varying levels of bias across the 17 included studies. Out of these studies, eight demonstrated a low bias risk across most domains, suggesting high methodological quality. Seven studies showed an unclear bias risk in one or more domains, mainly due to insufficient reporting on allocation concealment and participant blinding. Two studies showed a high bias risk in multiple domains, primarily related to selective reporting and incomplete outcome data. These findings underscore the need for cautious interpretation of results, due to variability in study quality (Figs. 3 and 4).
Fig. 3 Fig. 4
Fig. 4 Clinical responses
Clinical responsesBased on the included studies, disease stabilization was observed in 23 of 97 patients across 4 studies, with a pooled prevalence of 29.04% (95% CI 13.34–52.10%; I2 = 75%) (Fig. 5A). Sensitivity meta-analysis revealed that exclusion of the study by Bachanova et al. substantially reduced heterogeneity (I2 = 24%) and increased the pooled prevalence to 41.01% (95% CI 26.57–57.24%), suggesting that this study was a major source of heterogeneity.
Fig. 5
Forest Plot Analysis of NK Cell Therapy Efficacy in AML Patients; (A) Complete response rates across 14 clinical studies, showing pooled proportion of 0.48 (95% CI 0.32–0.65) with significant heterogeneity (I2 = 76%, p < 0.01). (B) Subgroup analysis of durable remissions (four studies) demonstrating pooled proportion of 0.29 (95% CI 0.13–0.52) with similar heterogeneity patterns (I2 = 75%, p < 0.01). Weighted contributions of individual studies are indicated by gray squares and horizontal lines represent 95% confidence intervals
Complete remission (CR) was achieved in 48.22% (95% CI 31.75–65.09%) of the 254 patients across 14 studies (Fig. 5B). Although significant heterogeneity was observed in CR outcomes (I2 = 76%), sensitivity analysis indicated that no single study was responsible for this heterogeneity. These findings underscore the overall potential of NK cell therapy in achieving meaningful clinical responses, particularly in terms of complete remission.
Researchers have made significant progress in exploring other clinical responses to NK cell therapy. For example, Ahmadvand’s study reported that 2 out of 10 patients achieved CR, with 4 patients showing partial responses [2]. Similarly, Bachanova’s study with 57 patients demonstrated a CR rate of 53% in those treated with IL-2 diphtheria toxin, compared to 21% in the control group [11].
Bednarski observed a 75% response rate in 10 patients, with 50% achieving CR [3], while Sarah Cooley’s study showed CR rates of 32% in phase 1, which increased to 40% in phase 2 [26]. Curti et al. [27] noted that 3 out of 13 patients achieved stable CR, remaining relapse-free for up to 34 months. In Curti’s 2016 study, 14 out of 17 patients achieved CR, with 56% surviving without relapse by the study’s conclusion [16].
Dolstra reported CR in 8 of 10 patients, with 4 remaining disease-free [18]. Fehniger’s study of 12 patients noted that 3 achieved long-lasting CR, with remission durations ranging from 32.6 to 47.6 months [28]. Muñoz Builes demonstrated a 20% reduction in relapse risk over three years in a study involving 35 patients [31]. Rosa Nguyen’s study of 21 patients found that 14 reached CR, though 8 experienced disease relapse [32].
In Sarah Parisi’s study of 17 elderly patients, 14 achieved CR, with those receiving higher NK cell doses exhibiting better overall and relapse-free survival rates [9]. Rizwan Romee’s study of 9 patients reported that 4 reached CR or CRi, underscoring the positive impact of memory NK cells on clinical outcomes [10]. Xian Zhang’s research with 85 patients demonstrated that a combination of DC-CIK and NK therapy improved overall survival (90.5%) and relapse-free survival (65.2%) [33]. In Panagiotis D. Kottaridis’ study, 3 out of 7 patients achieved CR, with 1 reaching CR1, 2 achieving CR2, and 3 reaching CR3m [7]. Jeffrey S. Miller reported that 5 out of 43 patients achieved CR [30].
Immune responsesThe analysis of immune response outcomes across 14 studies involving 222 patients demonstrated significant variability but encouraging results. Using a random-effects model, the pooled prevalence of immune responses was 69.34% (95% CI [49.18–84.09%; I2 = 81%]) (Fig. 6). The sensitivity analysis indicated that no single study was responsible for this heterogeneity.
Fig. 6
Forest Plot Analysis of NK Cell Therapy Efficacy in AML Patients (prevalence of immune responses)
Immune responses related to NK cell therapy also demonstrated significant positive outcomes in AML patients. Ahmadvand et al. reported increased NK cell cytotoxic activity and interferon‐gamma (IFN‐γ) production [2]. Similarly, Bachanova et al. observed NK cell chimerism in 27% of patients treated with IL-2 diphtheria toxin, indicating a positive effect on NK cell function [11]. Bednarski et al. reported that NK cells persisted in patients for several months, maintaining their anti-leukemic activity [3]. Sarah Cooley observed NK cell expansion in 36% (Phase I) and 27% (Phase II) of patients [26]. Curti (2011) detected the presence of NK cells in 14 patients’ peripheral blood, demonstrating their anti-leukemic potential [27]. Curti (2016) further confirmed NK cell chimerism in patients, demonstrating sustained activity against leukemia [16].
Dolstra observed NK cells in the peripheral blood of 7 patients, with these cells effectively sustaining their anti-leukemic function [18].Fehniger reported microchimeric of NK cells on day 7 in 10 patients, with 3 patients maintaining this up to day 14 [28]. Mario Muñoz Builes noted that chemotherapy enhanced the expression of NK cell ligands and reduced immune suppression, improving NK cell function [31]. Rosa Nguyen reported that 17 out of 21 patients experienced increased NK cell chimerism [32]. Sarah Parisi’s study demonstrated that patients receiving higher doses of NK cells had better immune responses and fewer regulatory T cells [9]. Rizwan Romee reported that memory NK cells exhibited higher cytotoxic activity and increased IFN‐γ production [10].
In Xian Zhang’s study, the combination of DC-CIK and NK therapies significantly improved immune responses and increased the proportion of specific T cells [33]. Panagiotis D. Kottaridis highlighted increased levels of activated NK cells and anti-leukemic immune responses [7]. Jeffrey S. Miller noted cytokine production and positive immune responses in patients [30].
Adverse eventsNo severe adverse events were consistently reported across the studies. Minor reactions, such as fever and injection site inflammation, were the most frequently observed adverse events. Overall, the safety profile of NK cell therapy appears to be acceptable, with no life-threatening events linked directly to the vaccine.
Adverse events related to NK cell therapy varied but were generally manageable. In Ahmadvand’s study, four patients reported side effects like fever, chills, and cytokine release syndrome (CRS), all of which were well-managed [2]. Bachanova reported no serious adverse events, with only mild reactions observed in patients [11]. Bednarski documented serious side effects, such as neutropenia and thrombocytopenia, which required clinical [3]. Cooley noted that 56% of patients treated with IL-15 experienced CRS [26].
In Curti’s 2011 study, mild side effects, such as fever and bacterial infections, were observed, but no severe events were reported [27]. Curti (2016) similarly identified bacterial infections and neutropenia-related complications, though no serious adverse events were noted [16]. Dolstra reported six patients experiencing febrile neutropenia, which was successfully managed [18]. Fehniger’s study noted mild side effects like fatigue and neutropenia, which were observed in 42% of patients [28].
Mario Muñoz Builes reported adverse events including CRS, GVHD, and mild reactions in some patients [31]. In Rosa Nguyen’s study, neutropenia and thrombocytopenia were observed in most patients, but no severe adverse events occurred [32].
Sarah Parisi reported bacterial infections and injection site reactions in some patients [9]. Rizwan Romee observed no severe adverse events, with mild reactions like fever and chills being the most common [10]. Xian Zhang recorded adverse events such as fever and transient hypoxemia, with no severe cases reported [33]. Panagiotis D. Kottaridis mentioned neutropenia, respiratory infections, and neutropenia-related complications [7]. S. Miller reported anemia and neutropenia as common side effects in patients [30]. Immunological and clinical responses, as well as reported adverse events of the studies included in this systematic review, are summarized in (Table 2).
Table 2 Immunological and clinical responses/ Adverse events of studies included in the systematic reviewPublication biasEgger’s test indicated the publication presence bias in CR (p value = 0.044), the outcome with the most studies. The Trim-and-fill analysis suggested that adding three studies would adjust the pooled prevalence [95% CI] of CR to 36.94% [20.92–56.47%].
Comments (0)