
Remember me




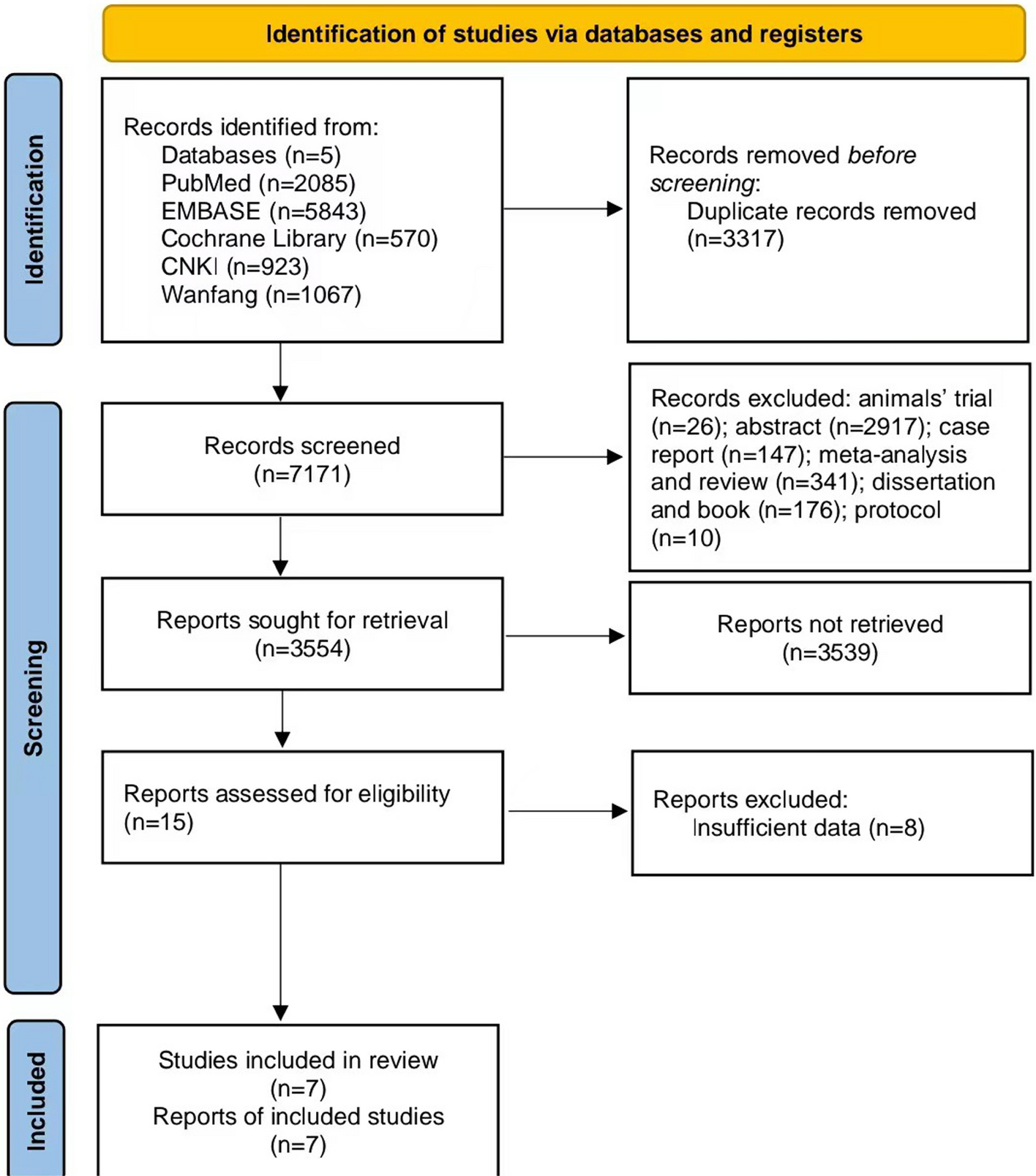
Initially, 10,488 articles were identified. Following the exclusion criteria, 6,859 articles were removed due to duplication and irrelevance, and an additional 3,617 articles were excluded based on study types (including animals’ trials, meeting abstracts, case reports, meta-analyses, reviews, dissertations, books, and protocols). According to the inclusion criteria, eight articles were further excluded due to insufficient data. As a result, seven articles [19, 23, 25,26,27,28,29] were included in this meta-analysis (Fig. 1).
Fig. 1
Flow diagram of the search process and study selection
Study characteristicsSeven articles were included in this meta-analysis, comprising two radomized cotrolled trials (RCTs), two sing-arm non-RCTs, and three cohort studies. A total of 707 patients with AML were analyzed, with ages ranging from 61 to 90 years. Two articles investigated different VEN dose during the expansion phase to assess the efficacy and safety of VEN + DEC, including 400 mg, 800 mg, and 1200 mg. The control groups featured four different treatment regimens: VEN + azacitidine (AZA), DEC + Cytarabine + Adriamycin + Granulocyte Colony-Stimulating Factor (CAG), DEC monotherapy, and intensive chemotherapy. There were three studies in China, three in USA, and one in Korea. Detailed study characteristics are reported in Table 1.
Table 1 Study characteristics of included studiesStudy qualityStudy quality was assessed using the ROB 2.0 tool in this meta-analysis. Overall, four studies exhibited some concerns regarding the risk of bias, two studies had a low risk, and one study was classified as having a high risk of bias (Figure S1).
Complete remission (CR)Fixed effects model analysis showed that VEN + DEC group (OR 1.90, 95%CI 1.36–2.67) could significantly improve CR among the elderly patients with AML compared to the control group (Fig. 2A).
Fig. 2
Forest plot of complete remission (A), composite response rate (B), overall response rate (C), median overall survival (D)
Subgroup analysis (Figure S2 and Table 2) revealed that the VEN (400 mg) + DEC group (OR 1.99, 95%CI 1.37–2.87) significantly increased CR among the elderly patients with AML (Figure S2 and Table 2), while the VEN (800 mg) + DEC group (OR 1.25, 95%CI 0.50–3.13) and VEN (1200 mg) + DEC group (OR 7.50, 95%CI 0.46–3.13) did not show significant improvements in CR. In addition, the studies evaluating CR included both RCTs and non-RCTs. To investigate the impact of study design on the results, we conducted a subgroup analysis. The findings revealed that in the RCT subgroup, there was no significant difference in CR between the VEN + DEC group and the control group (OR 1.11, 95% CI 0.45–2.73). However, in the non-RCT subgroup, the pooled results indicated that the VEN + DEC group (OR 2.08, 95% CI 1.44–3.00) was associated with a significantly higher CR rate among elderly patients with AML (Figure S3 and Table 2).
Table 2 Subgroup analysis of complete remission (CR), composite response rate (CRR), overall response rate (ORR), and adverse events (AEs)Composite response rate (CRR)Random effects model analysis showed that VEN + DEC group could not improve CRR (OR 2.29, 95%CI 0.96–5.51) (Fig. 2B) compared to the control group. In addition, none of the dosage groups significantly increased CRR (400 mg: OR 2.43, 95%CI 0.60–9.92; 800 mg: OR 2.06, 95%CI 0.78–5.45; 1200 mg: OR 1.50, 95%CI 0.14–5.45) (Figure S4 and Table 2).
Overall response rate (ORR)Random effects model analysis indicated that VEN + DEC group could not improve ORR (OR 2.31, 95%CI 0.95–5.63) (Fig. 2C) compared to the control group. Furthermore, none of the dosage groups demonstrated significant increases in ORR (400 mg: OR 2.16, 95%CI 0.50–9.38; 800 mg: OR 2.12, 95%CI 0.78–5.75; 1200 mg: OR 3.00, 95%CI 0.25–35.33) (Figure S5 and Table 2).
Median overall survival (OS)Fixed effects model analysis showed that VEN + DEC (HR 0.55, 95%CI 0.40–0.75) (Fig. 2D) was associated with a significantly lower risk of death than the control group.
Any grade adverse events (AEs)In the included studies, AEs mainly included febrile neutropenia, decreased white blood cell (WBC) count, anemia, and pneumonia. To visually present the occurrence of different AEs, a subgroup analysis was conducted. This analysis revealed a significant difference in any grade febrile neutropenia between the VEN + DEC group and the control group (OR 1.99, 95%CI 1.18–3.35). However, there was no significant difference in any grade decreased WBC count (OR 1.46, 95%CI 0.85–2.50), anemia (OR 1.05, 95%CI 0.50–2.19), or pneumonia (OR 1.33, 95%CI 0.57–3.14) (Fig. 3A and Table 2).
Fig. 3
Forest plot of any grade adverse events (A) and grade 3/4 adverse events (B)
Grade 3/4 adverse events (AEs)Regarding grade 3/4 AEs, subgroup analysis reported that there was a significant difference in grade 3/4 febrile neutropenia between the VEN + DEC group and the control group (OR 1.99, 95%CI 1.18–3.35). However, there was no significant difference in any grade decreased WBC count (OR 1.34, 95%CI 0.66–2.70), anemia (OR 0.87, 95%CI 0.49–1.55), or pneumonia (OR 1.01, 95%CI 0.42–2.43) (Fig. 3B and Table 2).
Sensitivity analysisSensitivity analysis showed that all the pooled CR, CRR, and ORR results were stable, indicating that our findings were reliable (Figure S56-S8).
Comments (0)