3.1 Study Selection and Data Extraction
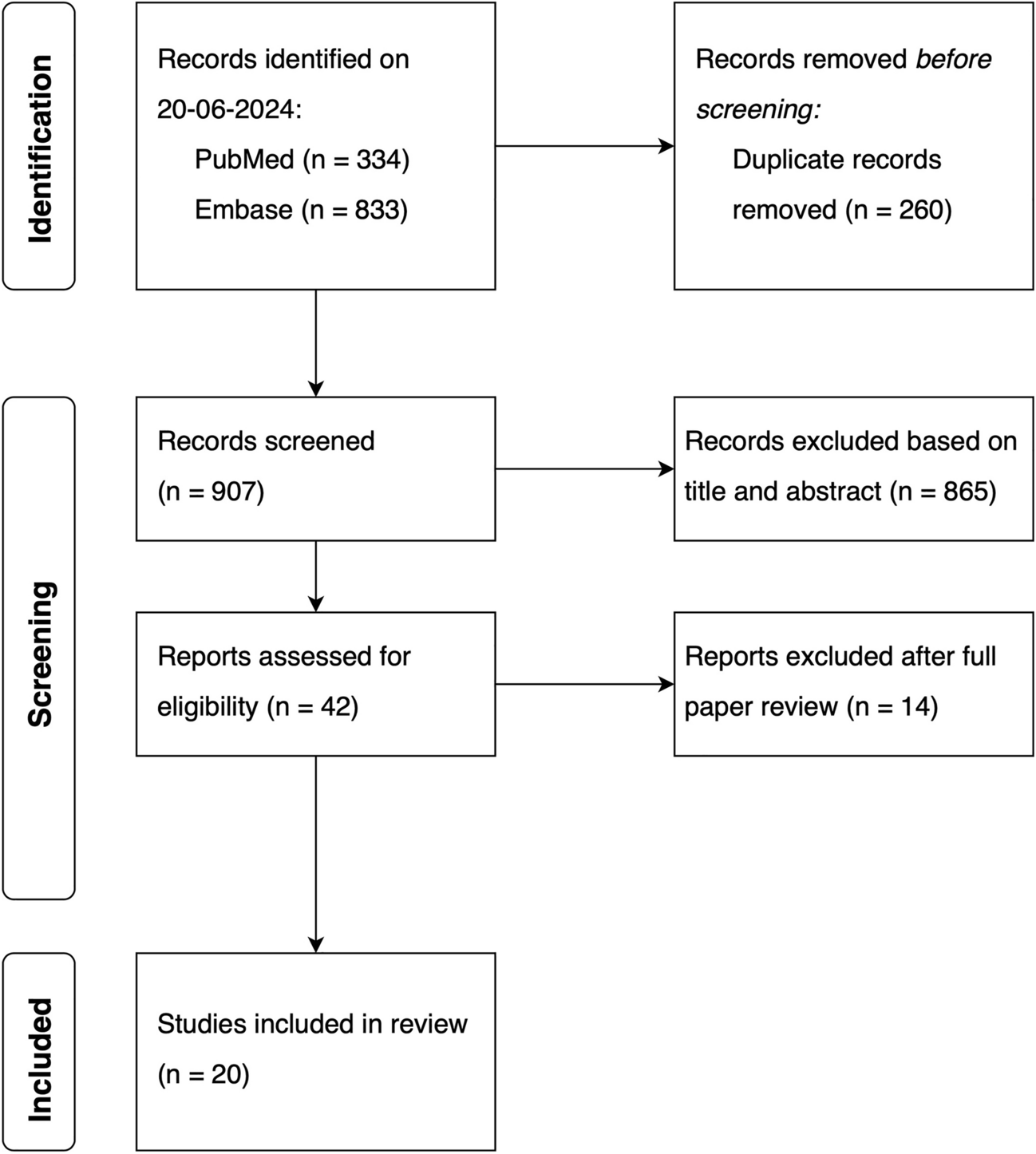
In total, 334 articles were retrieved from PubMed and 833 from Embase. After deduplication, 907 studies were screened on the basis of title and abstract, and 42 articles were read in full. Following the full paper review, 20 studies were included that focused on the PK of CFTR modulators in special CF populations. Figure 1 provides a detailed overview of the study selection.
An overview of the PK studies of CFTR-modulating drugs is presented in alphabetical order of the drug in the paragraphs below. Results are categorized according to the following flow: ADME of the CFTR modulator, adults, adults with moderate hepatic impairment, adults with pancreatic insufficiency, pregnant and breastfeeding women, and children. First, study characteristics of the individual CFTR modulator are described. Subsequently, PK and exposure parameters are discussed according to the ADME sequence. Additionally, eight studies evaluating drug–drug interactions (DDIs) following the coadministration of CFTR-modulators with CYP3A4 modulating drugs (i.e., clarithromycin, clofazimine, rifabutin, and ritonavir) are provided in the Online Supplementary Materials (Supplementary Tables S1–S3). These studies are not included in this systematic review, as they fall outside the scope of our review aim, which focuses on the PK of CFTR modulators in specific CF populations.
3.2 Elexacaftor
In total, seven studies on elexacaftor were included in this study [25,26,27,28,29,30,31], with three studies sponsored by Vertex [25, 27, 30]. A total of four studies [26, 28, 29, 31] did not receive funding from industry sources and were conducted by academic institutions, with two studies being financial supported by Cystic Fibrosis Foundation (CFF) grants [26, 31], the Gregory Fleming James Cystic Fibrosis Research Center [26], National Institutes of Health (NIH) grants [26], and/or the University of Alabama at Birmingham (UAB) Center for Clinical and Translational Science [26]. A total of two studies did not receive any specific grant [28, 29]. All studies examined the PK of elexacaftor within triple combination therapy (ELX/TEZ/IVA). Included studies provided PK data on adults with CF, adults with and without CF who have mild/moderate hepatic impairment (Child–Pugh Class A and B), and children with CF (Tables 3 and 4).
3.2.1 Clinical Pharmacology of Elexacaftor
Elexacaftor is a small-molecule corrector of the CFTR protein, improving its processing and trafficking activity to the epithelial cell surfaces. Elexacaftor is administered in combination with tezacaftor and ivacaftor. Elexacaftor has an acid dissociation constant (pKa) of 5.04 and is classified as a Biopharmaceutics Classification System (BCS) Class 2 drug (low solubility and high permeability) owing to its low solubility (0.0192 mg/mL) in buffer solutions with a pH range of 1–8 [32, 33]. The low solubility of elexacaftor limits its absorption in the gastrointestinal tract. Therefore, ELX/TEZ/IVA should be administered with fat-containing food to enhance the absorption of elexacaftor [34, 35]. Dietary fat stimulates bile secretion, which facilitates the solubilization and uptake of elexacaftor in the gastrointestinal tract. When ELX/TEZ/IVA is administered with a fat-containing meal, the bioavailability of elexacaftor reaches approximately 80% [34, 35]. Elexacaftor, as part of triple combination therapy (ELX/TEZ/IVA), is available in two formulations: immediate-release film-coated tablets and oral granules [34]. After oral administration, the Cmax is reached within 4–12 h [35]. Elexacaftor is approximately 99% bound to albumin as its main plasma protein [35]. After oral administration, the mean Vd/F of elexacaftor is 53.7 L, and the elimination t1/2 is 29.8 h [35].
In total, 92% of the administered dose of elexacaftor is absorbed into the systemic circulation, and of the absorbed fraction, 18% is excreted in bile, while 82% is metabolized by CYP3A4 and CYP3A5 [35]. The major metabolite is M23-elexacaftor, which is considered pharmaceutically active and has similar potency to elexacaftor [35, 36]. The AUC ratio of M23-elexacaftor relative to elexacaftor ranges from 35% to 50% [35]. The primary route of elimination for elexacaftor and M23-elexacaftor is via biliary excretion. After the oral administration of 200 mg [14C]-elexacaftor in a healthy male subject, 87.3% radioactivity was found in feces, and 0.23% of radioactivity was detected in urine [35, 36]. The amount of unchanged [14C]-elexacaftor was 23% in feces and below the limit of quantification in urine, which indicates that the renal excretion of elexacaftor is negligible [35]. As elexacaftor is primarily eliminated through hepatic metabolism and biliary excretion, pwCF with hepatic impairment are likely to be exposed to higher levels of elexacaftor. Therefore, the use of ELX/TEZ/IVA is not recommended in pwCF who have moderate hepatic impairment (Child–Pugh B) and should be avoided in pwCF with severe hepatic impairment (Child–Pugh C) [12]. However, when there is a clear medicinal need and the benefits outweigh the risks, ELX/TEZ/IVA can be used with caution at a reduced dose (Table 2).
Owing to the lipophilic properties of elexacaftor, it can cross biological membranes in the body by simple diffusion. On the basis of in vitro studies, elexacaftor is a substrate for the efflux transporters P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP) [34]. Additionally, elexacaftor and M23-elexacaftor are potentially weak inhibitors of organic anion transporting polypeptide (OATP) −1B1 or −1B3 [35].
3.2.2 Adult PwCF
The PK of elexacaftor in adult pwCF was examined in one NCA study [26], one population pharmacokinetic study [30], and one PBPK modeling study [31]. Additionally, two population pharmacokinetic reports from FDA and EMA authorization documents on ELX/TEZ/IVA were consulted [34, 35]. Subjects received the adult oral daily dose of 200 mg elexacaftor as part of ELX/TEZ/IVA [26, 30, 34, 35]. However, in Hong et al., dose reduction to alternate-day dosing was simulated using PBPK modeling [31].
Rose et al. reported a Cmin of 3.73 µg/mL following the standard daily dose of 200 mg [26]. Additionally, this study found a Cmin of 1.75 µg/mL for adult pwCF intolerant to the standard dose, using a reduced dosing regimen based on the individually determined daily dose equivalent (DDE) [26]. Hong et al. reported a Cmin of 0.89 µg/mL following alternate-day dosing [31]. The FDA’s authorization document on ELX/TEZ/IVA reported a Cmin of 5.49 µg/mL and a Cmax of 8.77 µg/mL using 200 mg elexacaftor once daily [35]. In Zemanick et al., the AUC was 158.4 µg/mL h [30]. This is in line with AUC values reported by the EMA (168 µg/mL h) and FDA (167 µg/mL h) [34, 35]. Considering the metabolism of elexacaftor, EMA’s authorization document reported the AUC of M23-elexacaftor (64.6 µg/mL h) [34]. Overall, the AUC of elexacaftor is consistent in adult pwCF.
3.2.3 Adult PwCF with Hepatic Impairment
A total of three NCA studies were included that primarily investigated the effect of liver involvement on the PK of elexacaftor [27,28,29]. Viswanathan et al. studied the PK in adults without CF with moderate hepatic impairment (Child–Pugh Class B) in comparison with healthy subjects [27]. Both groups were administered an oral daily dose of 100 mg elexacaftor, which is half of the standard ELX/TEZ/IVA adult daily dose [27]. Vonk et al. evaluated the PK in adult pwCF with mild or moderate hepatic impairment (Child–Pugh Class A or B) [28, 29]. Notably, in these two studies, elexacaftor was gradually introduced in four dosing steps, on the basis of respiratory and gastrointestinal symptoms, therapeutic drug monitoring (TDM), and serum liver function tests [28, 29].
Following a dosing regimen of 100 mg once daily, Viswanathan et al. found a nonsignificant 1.12-fold higher (95% CI 0.915–1.37) Cmax and a 1.25-fold higher (95% CI 1.01–1.54) AUC in adults with moderate hepatic impairment without CF relative to age-matched healthy controls [27]. Concerning M23-elexacaftor, Cmax and AUC values were 1.70-fold (95% CI 1.23–2.36) and 1.73-fold (95% CI 1.27–2.35) higher in the moderate hepatic impairment population compared with matched healthy adults [27]. In Vonk et al. (February 2024) the dose-normalized AUC varied considerably among adult pwCF with mild or moderate hepatic impairment, ranging from 0.28 to 1.12 (µg/mL h)/mg [28]. Although no substantial increase in elexacaftor exposure has been reported among included studies in adults with moderate hepatic impairment without CF relative to age-matched healthy controls, the drug label recommends a 25% dose reduction for elexacaftor in pwCF with moderate hepatic impairment [12] (Table 2). However, Viswanathan et al. recommend a more substantial reduction, suggesting a dosing reduction to 50% of the standard dosing of ELX/TEZ/IVA used in pwCF with normal hepatic function [27]. The study of Vonk et al. suggests an alternative approach for pwCF with mild or moderate hepatic impairment, recommending stepwise ELX/TEZ/IVA dosing under strict TDM [28].
3.2.4 Pediatric PwCF
Developmental differences between children and adults, including total body water, structure and function of the gastrointestinal tract, glomerular filtration rate, and the ontogeny of metabolic enzymes and transporters, may alter the ADME processes of elexacaftor and its metabolite, M23-elexacaftor, in pediatric pwCF [21]. Additionally, pwCF under the age of 6 years receive ELX/TEZ/IVA in granulate form. However, elexacaftor exposure was approximately 20% lower following the administration of ELX/TEZ/IVA formulated as oral granules compared with immediate-release film-coated tablets [34]. Therefore, these formulations are not interchangeable. Furthermore, CYP3A4 expression is minimal at birth but increases rapidly, attaining approximately 50% of adult levels between 6 and 12 months of age [37]. After the age of 1 year, CYP3A4 activity can exceed that of adults, resulting in increased hepatic clearance and necessitating relatively higher doses compared with adults [37] (Table 1).
One NCA study [25] and one population pharmacokinetic study [30] were conducted in children aged 2–17 years. Additionally, two population pharmacokinetic reports from FDA and EMA authorization documents on ELX/TEZ/IVA were consulted [34, 35]. The number of children included in each study ranged from 18 to 138 [25, 30, 34, 35]. Owing to the variability in dosing



Comments (0)