
Remember me
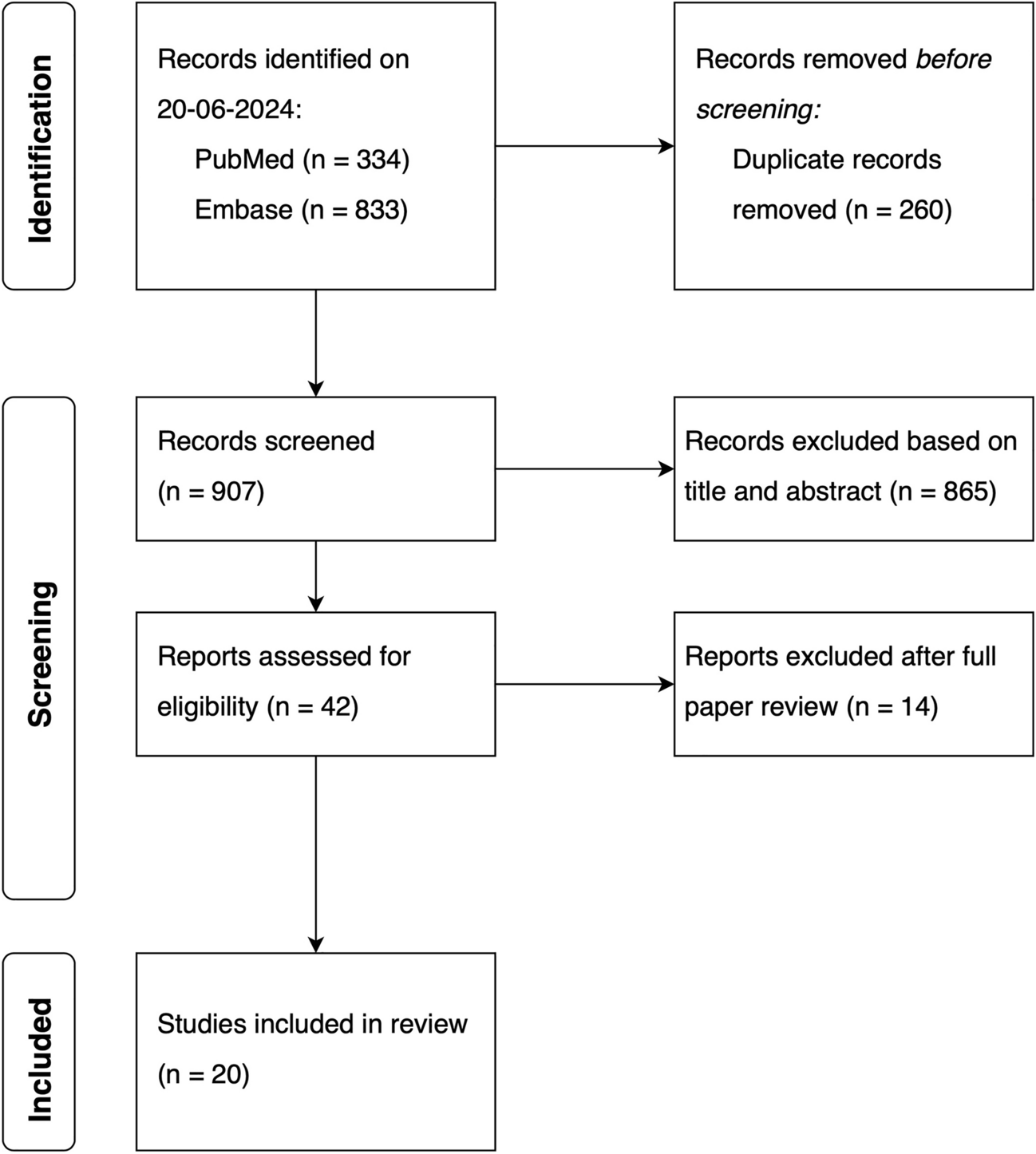


This population pharmacokinetic (PK) analysis is based on clinical data from 11 studies in adult patients with R/R BCP-ALL or R/R B-cell non-Hodgkin lymphoma (NHL) [InO either as a single agent, or combined with rituximab, or with rituximab plus chemotherapy], and one study of single-agent InO in pediatric patients with R/R BCP-ALL (Trial ITCC-059 phase IA and phase II). Details on the studies conducted in adults were described by Garrett et al. [23]. Details on the ITCC-059 trial were published by Brivio et al. and Pennesi et al. [20, 24].
The inclusion criteria of trial ITCC-059 were: age ≥ 1 and < 18 years, diagnosis of R/R CD22+ BCP-ALL, and provision of informed consent. See Table 1 of the Electronic Supplementary Material (ESM) for the full inclusion and exclusion criteria. Inotuzumab ozogamicin was administered as an intravenous infusion over 60 minutes in 3-week cycles in a fractionated manner with dosing on a weekly basis. In the phase I part, two dose levels were explored; at dose level 1, InO was given at 1.4 mg/m2/cycle and 1.2 mg/m2/cycle once remission was achieved; at dose level 2, InO was given at 1.8 mg/m2/cycle and 1.5 mg/m2/cycle after remission. The latter was selected as the RP2D [24]. Each InO dosing regimen was fractioned in three doses/cycle on days 1, 8, and 15 (dose level 1: 0.6, 0.4, 0.4 mg/m2, and after remission 0.4, 0.4, 0.4 mg/m2; dose level 2: 0.8, 0.5, 0.5 mg/m2, and after remission 0.5, 0.5, 0.5 mg/m2). A maximum of six cycles was permitted, except for patients proceeding to a transplant, where a maximum of two to three cycles was used. Clinical characteristics of the children were a median age of 9 years (range 1–17 years) and a median white blood cell count of 3.33 × 109 (range 0.19–132 × 109, counts), 67.9% were male. Detailed pediatric patient characteristics were reported previously [20, 24].
All studies were approved by the independent ethics committee at each participating center and were conducted in accordance with the Declaration of Helsinki and the International Conference of Harmonization Guideline for Good Clinical Practice. The data from the adult patients were provided by Pfizer. ITCC-059 was sponsored by Erasmus MC and financed by Pfizer (EudraCT Number: 2016-000227-71).
2.2 PK Sampling and Bioanalytic MethodsInotuzumab ozogamicin (as the parent drug) and unconjugated calicheamicin PK samples were collected and analyzed. The serum concentration of InO and unconjugated calicheamicin from children were quantified by validated high-performance liquid chromatography with tandem mass spectrometry. The lower limit of quantification (LLOQ) of the serum concentration of InO was 1.0 ng/mL; and 0.05 ng/mL for the serum concentration of unconjugated calicheamicin. The bioanalytical analysis method was designed for indirect measurement of N-acetyl-γ-calicheamicin dimethyl hydrazide conjugated to the antibody of InO. The same method was used for PK samples from adult patients with BCP-ALL, as described by Garrett et al. [23], where it measured the conjugated calicheamicin released from ADC and InO quantitation was based on the average drug-to-antibody ratio of the dosing formulation used to prepare calibration standards. A validated enzyme-linked immunosorbent assay method, designed to directly assess N-acetyl-γ-calicheamicin dimethyl hydrazide linked to the InO antibody, was used to measure the serum concentration of InO from adult patients with NHL [23]. The bioanalytical analysis methods were validated/revalidated by PPD (Richmond, VA, USA), and performed at laboratories designated by Pfizer.
In this study, the population PK analysis refers to InO concentrations because all unconjugated calicheamicin serum concentrations from pediatric trial participants were below the LLOQ. The majority of unconjugated calicheamicin serum concentrations were also below the LLOQ in prior adult studies [23]. Data in adults have shown that InO exhibits both linear-dependent and time-dependent clearance components [23]. In adults, the steady state was achieved by the fourth cycle and the linear clearance component predominates over the time-dependent component. Therefore, in children, PK samples were taken during cycles 1, 2, and 3, to better characterize both the linear-dependent and time-dependent clearance of InO. In total, six blood samples were collected per patient during cycle 1 on day 1 (pre-dose and 1 hour after dose), day 8 (pre-dose), day 15 (pre-dose and 1 hour after dose), and at the end of the cycle (day 22) for trough samples; five samples were collected in cycle 2 (trough samples collected on day 28 and without the pre-dose samples on day 1) and four samples were collected in cycle 3 (trough samples collected on day 28 and without the pre-dose samples on day 1 and without the day 15 1 hour after dose samples). Details of the sampling schedule for the pharmacokinetics of InO are reported in the Appendix (Table 2 of the ESM). No pediatric patients had treatment induced anti-drug antibodies and only one had baseline positive anti-drug antibodies [20].
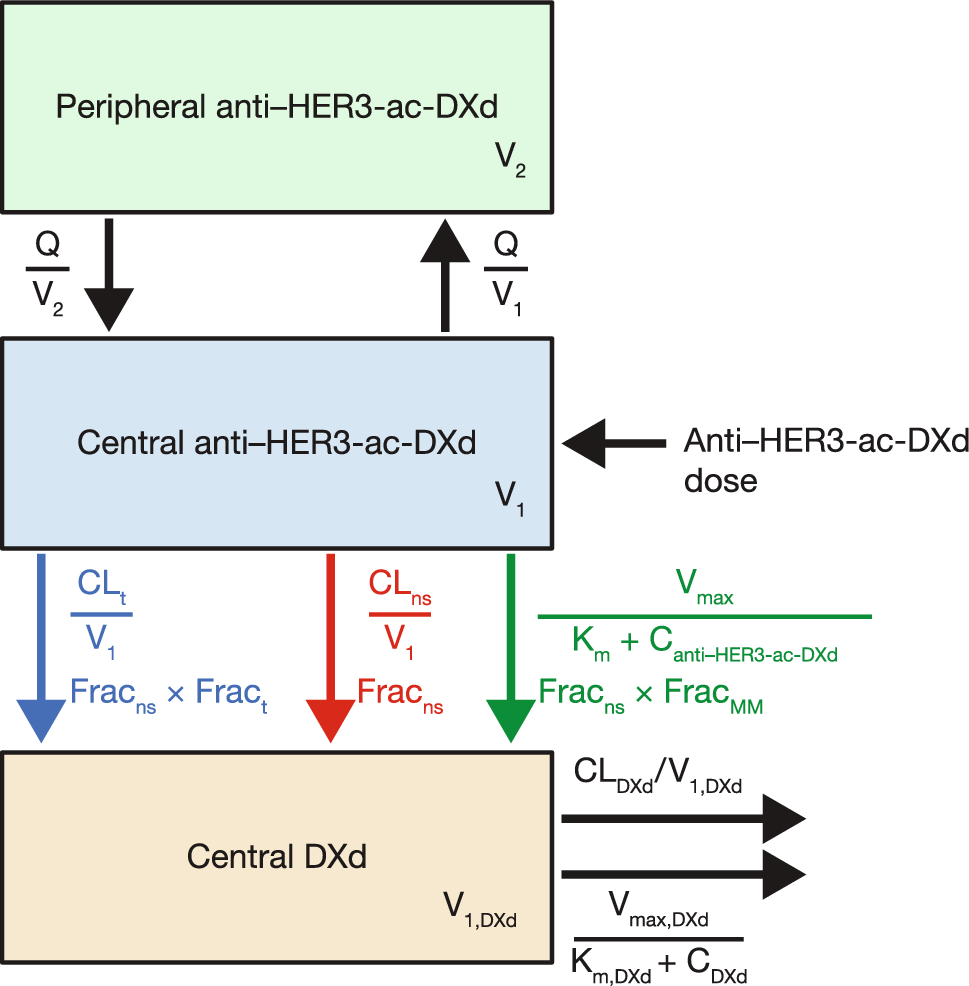
2.3 Model DevelopmentThe starting point for model development was a previously developed population PK model for adult patients with BCP-ALL and B-cell NHL based on data from 11 adult trials. This model consisted of a two-compartment model with linear (CL1, L/h) and time-dependent clearance (CLt, L/h) (Fig. 1). The two-compartment model structure aligns with the general modeling framework for the pharmacokinetics of monoclonal antibodies with target-mediated drug disposition [25, 26]. The linear InO clearance (CL1) is considered to represent the elimination of endogenous immunoglobulin G, mediated by the Fc receptors (in the skin, muscle, and liver) and salvaged by neonatal Fc receptor. The time-dependent clearance, described by \(_=_*^_* Time)}\), relates to the target-mediated drug disposition, in which the capacity decreases over time as the tumor burden (and thus antigen expression) reduces. The differential equations used to describe the PK data were:
$$\frac}A\left( 1 \right)}}}t}} = - k_ *A\left( 1 \right) - k_ *A\left( 1 \right) + k_ *A\left( 2 \right),$$
$$\frac}A\left( 2 \right)}}}t}} = k_ *A\left( 1 \right) - k_ *A\left( 2 \right),$$
where Vi represents the volume of the ith compartment, A(i) is the amount in the respective compartment, \(_\) is the elimination rate constant from the central compartment, and Q is the intercompartmental clearance translated into the distribution rate constant (k12, k21).
Fig. 1
Inotuzumab ozogamicin pharmacokinetic model structure. Total clearance (CLtotal) is the sum of linear clearance (CL1) and time-dependent clearance (CLt). CL2 initial value of time-dependent clearance, IV intravenous, kdes decay coefficient, Q intercompartment clearance, V1 volume of distribution in the central compartment, V2 volume of distribution in the peripheral compartment
Covariates in the adult final model were baseline body surface area (BBSA, m2), disease type and/or analytical methods (ALL effect, NHL as the reference), and concomitant rituximab treatment (with rituximab as the reference) on CL1; BBSA on the volume of distribution in the central compartment (V1, L); BBSA on CL2; ALL effect (accounts for disease type (NHL/ALL) and/or different bioanalytical analysis methods) and baseline percentage of blasts in the peripheral blood (BLSTPB, %) on the decay coefficient (kdes) of CLt [23]. Interindividual variability (IIV) was modeled using the following equation:
$$P_ = P_ \times e^ } \right)}} ,$$
where \(_\) is the parameter estimate of the ith individual (empirical Bayes estimates/post hoc parameters), \(_\) represents the fixed population parameter estimate, and \(_\) depicts the IIV of the ith individual, which is assumed to follow a normal distribution with a mean 0 and a variance ω2. Residual unexplained variability was described by two separate additive residual errors based on log-transformed data to take different bioanalytical methods used in different disease types into account. Last, the method 3 (M3) modeling approach was applied to handle InO concentration data that were below LLOQ [27, 28]. Observations below the LLOQ were retained in the analysis and treated as censored.
The first step in model building was to re-estimate the adult model including covariate effects on the pooled dataset and to estimate the separate residual error for a pediatric population to further account for variability between trials. Subsequently, specific covariates important for the pediatric population were further investigated. The included covariates relate to body size, age, and disease. The covariate–parameter relationships to be examined are shown in Table 1. Baseline covariates assessed in the model include replacing certain covariates presented in the adult model, namely, BBSA by body weight (kg), or lean body mass (LBM, kg) [29, 30], and BLSTPB by baseline absolute blast counts in peripheral blood (BLSTABL) on kdes. The InO serum concentration was measured in the central compartment (from blood), therefore BLSTABL is considered a better covariate than bone marrow blast for describing the target-mediated clearance component of InO in the bloodstream. Further testing included age (years), hepatic impairment (BHGRADE, National Cancer Institute Organ Dysfunction Working Group criteria for hepatic impairment [31]), baseline albumin (g/dL), baseline alanine aminotransferase (U/L) on CL1; age, ALL effect, BLSTABL on CL2; and age on kdes. Noteworthy, blast in peripheral blood (BLSTPB and BLSTABL) does not apply for patients with B-cell NHL. Therefore, missing blast-related covariates were not imputed for patients with B-cell NHL and the effects were only modeled in patients with BCP-ALL. In addition, age effect was also modeled solely for patients with BCP-ALL, as patients with NHL only consisted of adults.
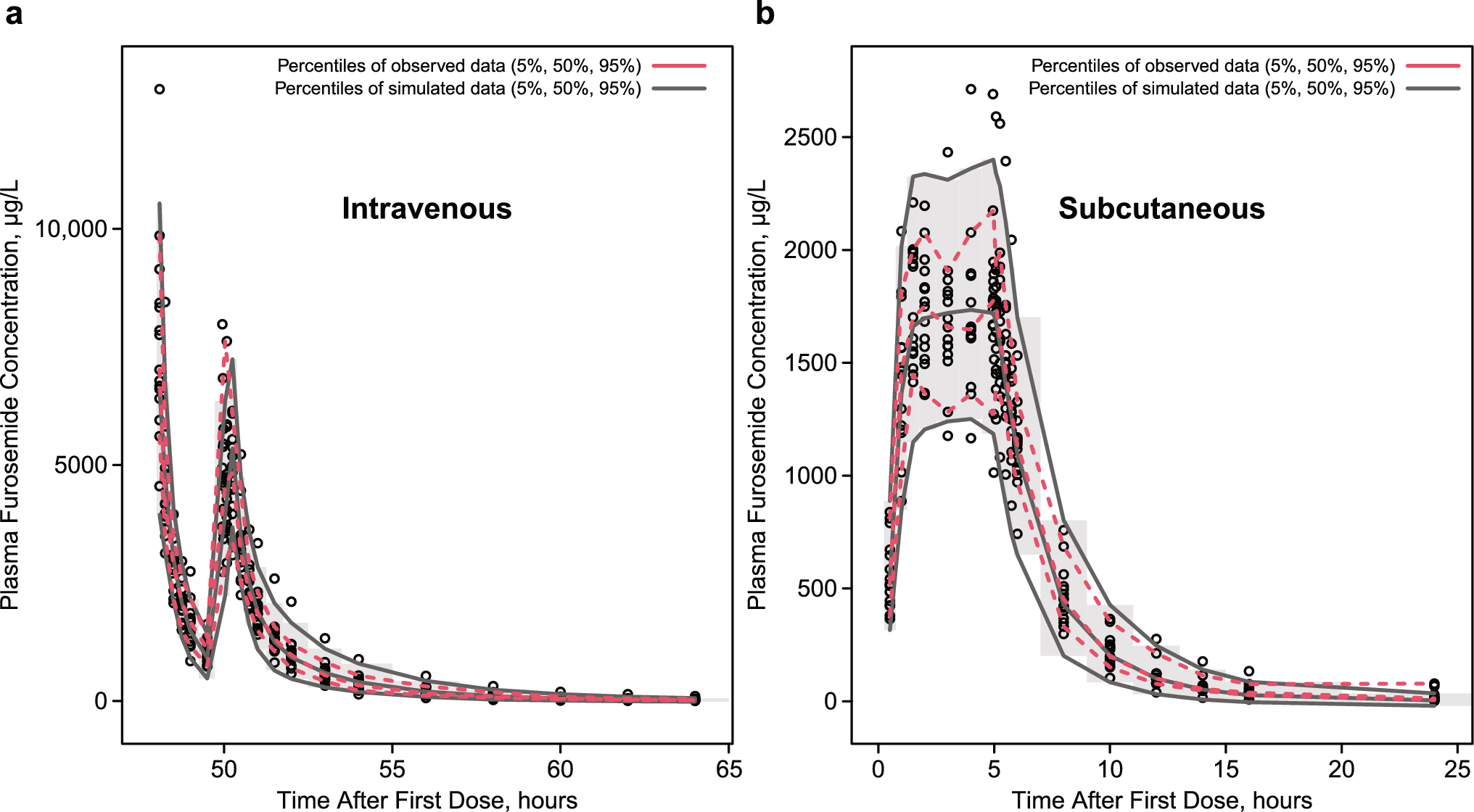
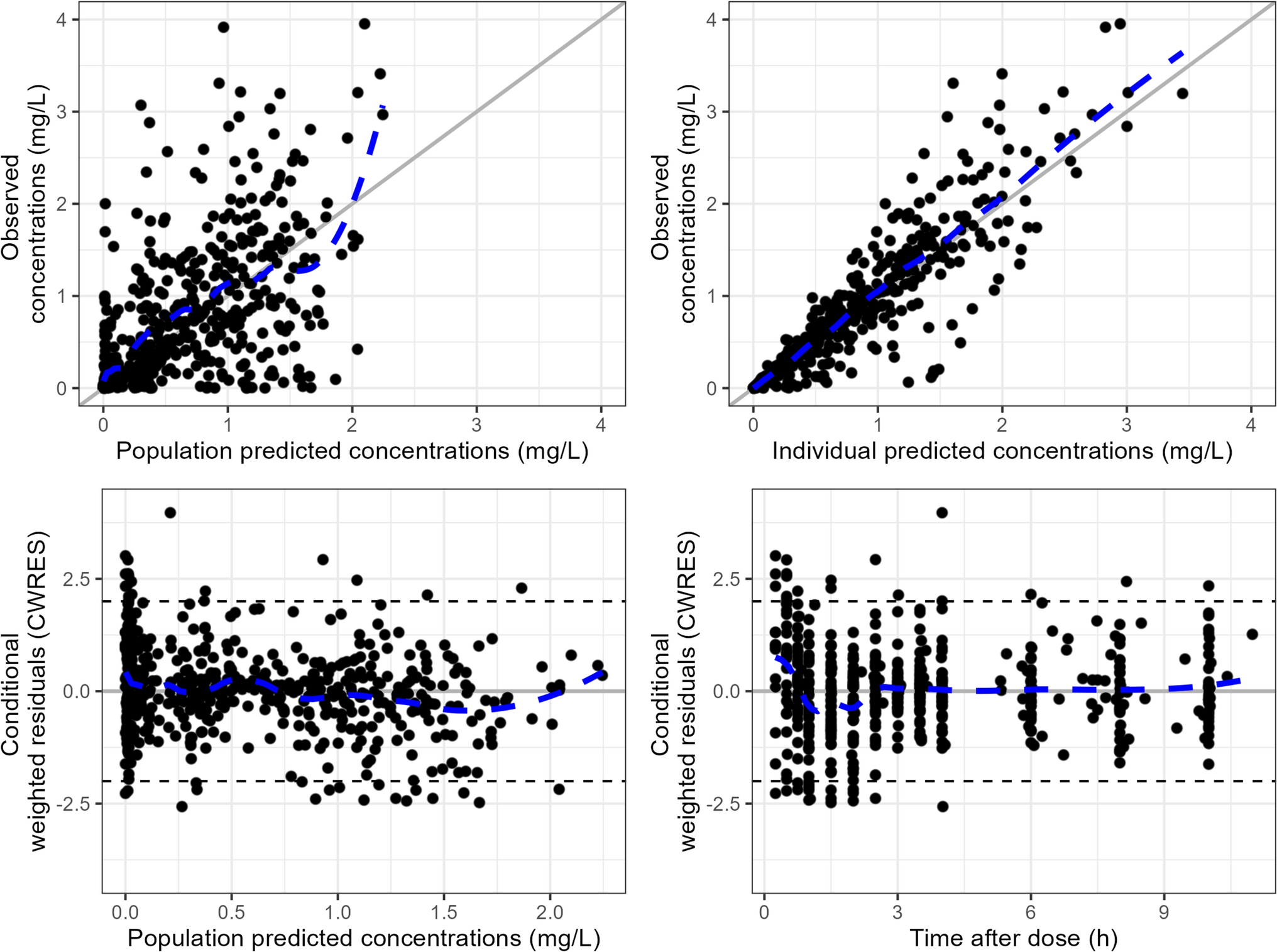
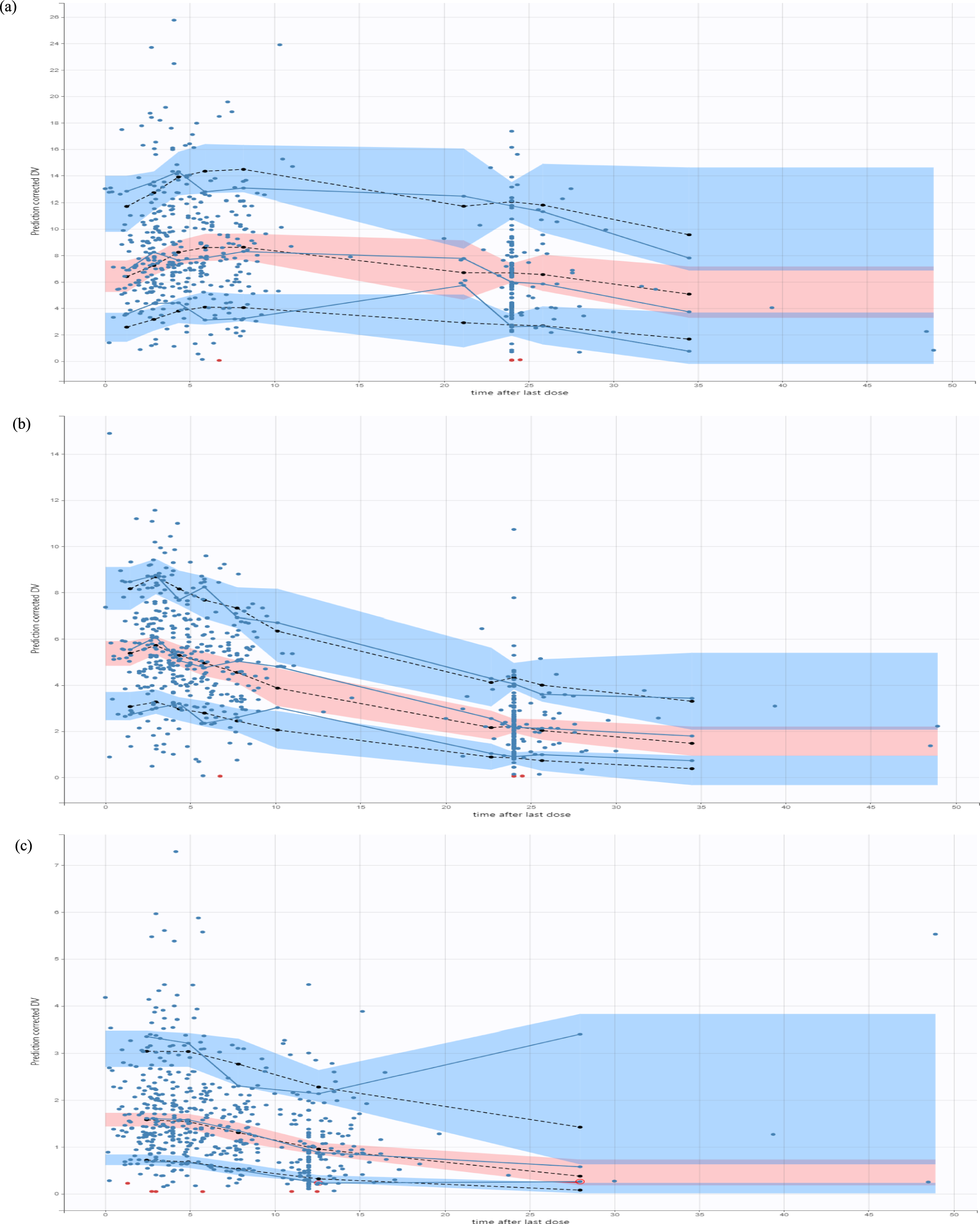
Table 1 Covariates examined in a pediatric population pharmacokinetic analysis of inotuzumab ozogamicin2.4 Model EvaluationCovariate selection was based on parameter precision, biological plausibility, and statistical significance. For hierarchically nested models, a drop of the objective function value ≥10.83, corresponding to p < 0.001 (\(^\)-distribution with 1 degree of freedom), was used to determine a significant improvement of the fit. Model performance was evaluated by goodness-of-fit diagnostic plots, and prediction and variability corrected visual predictive checks (pvcVPC) [32]. The PK parameter estimates precision was assessed using the sampling importance resampling (SIR) procedure [33].
2.5 Model-Based Exposure EstimationCumulative area under the concentration–time curve (AUC) for cycle 1 was estimated using the maximum a posteriori Bayesian estimation with the POSTHOC option of NONMEM. The final model with actual trial dosing records was used to estimate InO exposure for each pediatric patient. Differences in cumulative AUC at the end of cycle 1 were compared between responders and non-responders and between positive/negative-MRD status among responders, to preliminarily evaluate the exposure–efficacy relationship. Cumulative AUC at the end of cycle 1 was selected as the exposure metric for statistical tests because of the positive association between the InO average concentration (calculated as the ratio of cumulative AUC over timeframe) and the efficacy endpoint in adults with R/R BCP-ALL [34]. The Wilcoxon rank-sum test and logistic regression with cumulative AUC and covariates included in the final model were used to examine the preliminarily exposure–efficacy relationship. Hematologic response was defined as patients with < 5% blasts in the bone marrow and no circulating blasts or extramedullary disease. Minimal residual disease negativity was defined as MRD < 1 × 10-4 with real-time quantitative-polymerase chain reaction or < 0.01% with flow cytometry when the polymerase chain reaction was negative but the quantitative range was > 1 × 10-4. The relationship between pharmacodynamic parameters and the response was analyzed before and published by our group [20].
2.6 Model-Based SimulationsSimulations of the final InO population PK model were performed to simulate the expected concentration–time profile in adult and pediatric patients with BCP-ALL at a fixed dosing regimen (the approved dosing regimen for adult R/R BCP-ALL and the pediatric RP2D: 1.8 mg/m2/cycle fractionated in three weekly administrations for the first cycle of 21 days, followed by 1.5 mg/m2/cycle for up to five cycles of 28 days). The simulations were employed to assess the PK endpoints in adult and pediatric patients, such as the cumulative AUC and terminal half-life. In addition, to evaluate whether similar InO exposure can be achieved without a loading dose, the final PK model was used for simulation in adult and pediatric patients with BCP-ALL at the above-mentioned fixed dosing regimen without a loading dose on day 1 in the first cycle (1.5 mg/m2/cycle fractionated evenly in three weekly administrations for the first cycle of 21 days, followed by 1.5 mg/m2/cycle for up to five cycles of 28 days).
2.7 SoftwareNonlinear mixed-effects modeling was performed using NONMEM (version 7.5.0; ICON Development Solutions, Ellicott City, MD, USA) and Pearl-speaks-NONMEM (PsN, version 5.3.0) with stochastic approximation expectation maximization (SAEM) and importance sampling (IMP) expectation maximization as an estimation method [35,36,37]. Parameter precision was obtained by SIR as implemented in PsN [33]. Pirana (version 2.9.9) was used as a graphical user interface for NONMEM [38]. R (version 4.2.1) was used for data handling and visualization.
Comments (0)