
Remember me


Liver cancer remains a global health challenge, with an incidence estimated to reach >1 million cases by 2025.[1] Hepatocellular carcinoma (HCC) is the most common form of liver cancer and accounts for ~90% of cases.[2] Notably, China, representing one-quarter of the world’s population, accounts for half of the new HCC cases and its related deaths.[3] The prognosis for HCC patients is dismal, with an estimated 5-year survival rate of 12.1%.[4] Curative treatment is feasible only when the disease is detected at an early stage, underscoring the critical importance of early HCC detection through screening to improve survival rates.[5]
Chronic hepatitis B virus (HBV) infection is the primary cause of HCC worldwide, particularly in East Asia and Africa.[6] According to the data from the China National Cancer Registry, approximately 83.2% of HCC deaths are attributed to known risk factors, with 77.7–88.0% attributed to HBV and/or hepatitis C virus (HCV) infection.[7,8] The evidence linking HBV with HCC is unquestionable.[9] HBV DNA integrates into the host cellular genome in the majority of chronic hepatitis B (CHB) patients and induces genetic damage. DNA integration in non-tumoral cells in patients with HCC suggests that genomic integration and damage precede the development of tumors. The lifetime risk of HCC among HBV carriers is estimated to be 10–25%.[10] Thus, professional societies recommend HCC surveillance in high-risk individuals, including patients with cirrhosis and subgroups of patients with CHB.[11,12]
Two national surveys for HBV epidemic were conducted in China in 1992 and 2006. Despite a one-quarter decrease in the overall prevalence of HBV infection in 2006 compared to 1992, the prevalence remained high at 7.18%.[13,14] To address the high prevalence of HBV infection and combat the increasing incidence of liver cancer, China implemented two national liver cancer screening programs, both of which targeted males aged 35–64 years and females aged 45–64 years with HBV infection, who had a higher incidence of liver cancer and were more likely to benefit from HCC screening; all the participants were required to undergo serum alpha-fetoprotein (AFP) laboratory tests and abdominal ultrasound.[15–18] Although conclusive evidence on the reduction in HCC mortality through screening is lacking, our recent multicenter prospective study confirmed that screening among HBV-infected populations significantly improved HCC survival, highlighting the “real-world” feasibility and effectiveness of HCC screening for the early detection of HCC and for improving survival.[19] One of the goals of the Healthy China 2030 program is to increase the 5-year nationwide cancer survival rate through cancer prevention and screening by 2030. Expanding the coverage of HCC screening and improving HCC survival rates are crucial for achieving this goal.
No specific surveys on the prevalence of HBV infection among the general population have been carried out since 2006. Consequently, for specific populations who are eligible for liver cancer screening, mainly males aged 35–64 years and females aged 45–64 years, the current prevalence and future trends of HBV infection are unclear. This has sparked debates regarding whether HCC screening should continue to focus on individuals with HBV infection or be expanded to the general population. We aimed to conduct a large population-based study to assess the seroepidemiology of HBV infection among Chinese individuals eligible for HCC screening to provide the latest evidence for appropriate HCC screening strategies in China.
Methods Ethical approval and informed consentThis study was approved by the Institutional Review Board of the National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (approval No. 2018103113063502). Staffs in each site have explained and obtained written informed consent from participants regarding the following items: objectives, reasons for enrollment, the methods and time period, potential benefits and risks, need of personal information and blood samples, and means for information storage.
Study design and participantsThis population-based cross-sectional study was conducted in four provinces in China (Henan, Shandong, Anhui, and Jiangsu) from January 1, 2015, to December 31, 2023, as part of the ongoing national liver cancer screening program. Twenty-one counties were selected by cluster sampling among candidate screening sites according to the sampling principle including: (1) with solid foundation of cancer registry and death registry to carry out follow-up and quality control, and (2) with experiences of carrying out scientific research or population programs related to prevention and control of chronic diseases. All participants were enrolled by active recruitment. Permanent residents aged 35–64 years for men and 45–64 years for women living in the selected counties were approached by trained staffs by means of phone-calls and personal encounter. A standardized questionnaire was used to collect basic information including sex, age, ethnicity, marital status, educational level, source of drinking water, and history of smoking and alcohol consumption. Body mass index (BMI) was determined during physical examination.
Serum samples collectionAbout 5 mL venous blood was obtained from each participant and immediately sent to the local laboratory where sera were separated and stored at –20°C prior to testing. Serum samples were tested for hepatitis B surface antigen (HBsAg) using enzyme-linked immune absorbent assay (ELISA) test kits. The presence of HBsAg was used as an indicator of chronic HBV infection. Interviews, laboratory tests, and notification of results were provided free to all participants. Test results were enveloped, sealed, and delivered personally to each participant by local community responsibility doctors.
Statistical analysisData were analyzed using R software version 4.3.2 (R Project for Statistical Computing). We used proportions (%) to describe the demographic characteristics of study participants. We calculated the prevalence of HBV infection including its associated 95% confidence interval (CI) for the entire study population. χ2 test were used to compare the prevalence rates of the HBV in different genders and age groups, and between other demographic groups. The missing baseline information can introduce bias in subgroup analysis because individuals who are HBsAg positive tend to be less likely to complete the questionnaire compared to HBsAg negative individuals. To correct for the impact of missing values, we performed multiple imputations on the missing values. We used the random forest method to impute the variables with missing values, considering the factors such as year, sex, age, ethnicity, marital status, educational level, source of drinking water, BMI, smoking, and alcohol consumption. P values of less than 0.05 were considered to be statistically significant.
ResultsFrom January 2015 to December 2023, 603,082 individuals were recruited from 21 counties in 4 provinces, and blood samples were collected for analysis. Among these individuals, 213,367 (35.4%) were enrolled in 2015–2016, 97,061 (16.1%) were enrolled in 2017–2018, 125,036 (20.7%) were enrolled in 2019–2020, and 167,618 (27.8%) were enrolled in 2021–2023. The baseline characteristics of the study participants are shown in Table 1. Of the total population, 315,183 individuals (52.3%) were male, with a mean age of 51 years (interquartile range: 45–57 years), and 287,899 individuals (47.7%) were female, with a mean age of 53 years (interquartile range: 49–58 years). Han Chinese individuals accounted for 99.4% (n = 577,338) of the whole population, and married individuals comprised the greatest percentage (95.4%) of the population. Among the study participants, only 2.6% had a high school education or above, and the majority (83.6%) had a primary or middle school education. The main source of water for most individuals (75.8%) was tap water. A high percentage of the participants had a BMI ranging from 24.0 kg/m2 to 28.0 kg/m2, accounting for 45.5% of the total population. Nearly 20% of the participants reported the history of current or past smoking and alcohol consumption, with the majority being male.
Table 1 - Sociodemographic characteristics of the screening target population of hepatocellular carcinoma by sex. Variable All (N = 603,082) Male (N = 315,183) Female (N = 287,899) Age (years) 52.0 (47.0–57.0) 51.0 (45.0–57.0) 53.0 (49.0–58.0) 35 to <45 72,880 (12.1) 72,880 (23.1) 0 (0) 45 to <55 306,657 (50.8) 138,142 (43.8) 168,515 (58.5) 55 to <65 223,545 (37.1) 104,161 (33.0) 119,384 (41.5) Ethnic origin Han 577,338 (99.4) 301,246 (99.4) 276,092 (99.4) Others 3334 (0.6) 1752 (0.6) 1582 (0.6) Marital status Unmarried 5195 (0.9) 4878 (1.6) 317 (0.1) Married 553,989 (95.4) 288,337 (95.2) 265,652 (95.7) Divorced 9695 (1.7) 5942 (2.0) 3753 (1.4) Widowed 11,793 (2.0) 3841 (1.3) 7952 (2.9) Education No schooling 79,736 (13.7) 16,984 (5.6) 62,752 (22.6) Primary school 232,515 (40.0) 105,588 (34.8) 126,927 (45.7) Middle school 253,361 (43.6) 168,757 (55.7) 84,604 (30.5) High school or above 15,060 (2.6) 11,669 (3.9) 3391 (1.2) Water source Unprocessed water 140,345 (24.2) 75,587 (24.9) 64,758 (23.3) Tap water 440,327 (75.8) 227,411 (75.1) 212,916 (76.7) BMI <18.5 (kg/m2) 4425 (0.8) 1949 (0.6) 2476 (0.9) 18.5 to <24.0 (kg/m2) 240,011 (41.3) 130,569 (43.1) 109,442 (39.4) 24.0 to <28.0 (kg/m2) 263,935 (45.5) 139,784 (46.1) 124,151 (44.7) ≥28.0 (kg/m2) 72,264 (12.4) 30,683 (10.1) 41,581 (15.0) Smoking No 462,697 (79.7) 189,208 (62.4) 273,489 (98.5) Ever 117,975 (20.3) 113,790 (37.6) 4185 (1.5) Alcohol drinking No 469,151 (80.8) 199,261 (65.8) 269,890 (97.2) Ever 111,510 (19.2) 103,731 (34.2) 7779 (2.8)Data are shown as n(%) or median (interquartile range). BMI: Body mass index. Data of 22,410 participants were missing for ethnic origin, marital status, education, per capita income per year, water source, and smoking; data of 22,447 participants were missing for BMI; and data of 22,421 participants were missing for alcohol drinking.
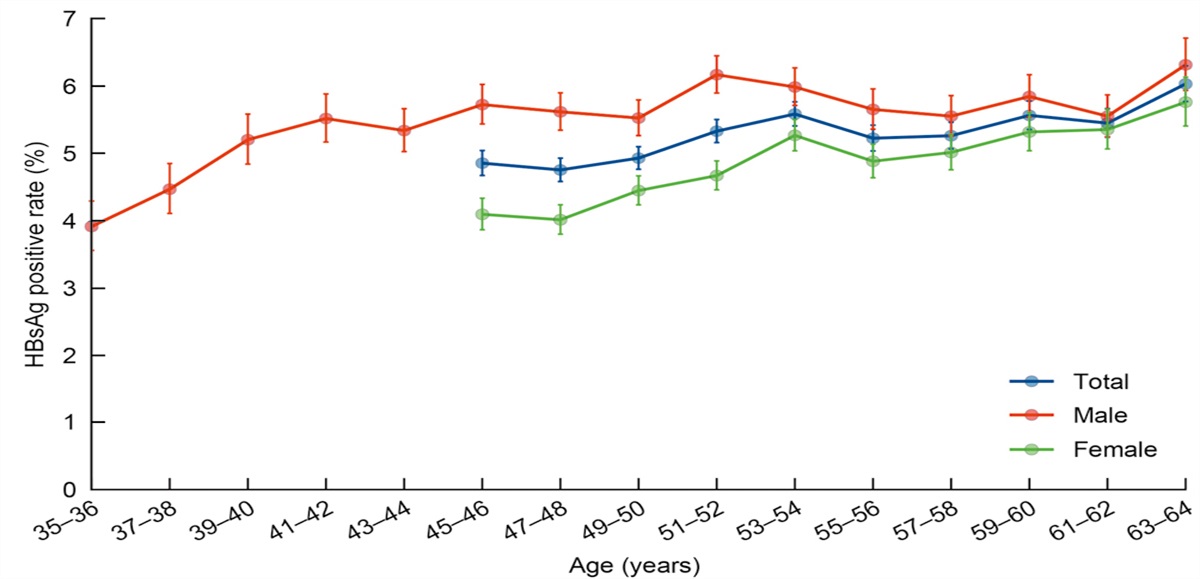
Overall, the prevalence of HBsAg in the study population was 5.23%. Table 2 shows the prevalence of HBsAg based on the selected characteristics of the study participants. Specifically, the overall prevalence of HBV infection was greater in males than in females (5.60% vs. 4.82%, χ2 = 187.52, P <0.0001). The age-specific prevalence of HBV infection revealed that the HBsAg positivity rate in males was greater than that in females in all age groups, ranging from 45 years to 64 years [Figure 1]. Compared with individuals in the other age groups, individuals in the group aged 55–64 years exhibited the highest prevalence of HBV infection, indicating that the HBsAg positivity rate was greater in aged participants than in younger participants. Additionally, the prevalence of HBsAg was calculated by sex across different birth cohorts, revealing an overall downward trend of infection rate for both sexes. Individuals born in more recent cohorts exhibited a lower prevalence of HBV infection as compared to those born earlier [Figure 2]. Figure 3 shows the trend of HBV prevalence from 2015 to 2023, revealing that while there are fluctuations in annual infection rates, the overall rate has remained remarkably stable at approximately 5%.
Table 2 - Prevalence of positive HBsAg and its risk factors among screening target population of hepatocellular carcinoma. Variables Total HBsAg positive Prevalence of HBsAg (% [95% CI]) χ 2 value P values All 603,082 31,528 5.23 (5.17–5.28) Sex 187.52 <0.0001 Male 315,183 17,660 5.60 (5.52–5.68) Female 287,899 13,868 4.82 (4.74–4.90) Age 41.73 <0.0001 35 to <45 (years) 72,880 3639 4.99 (4.84–5.15) 45 to <55 (years) 306,657 15,674 5.11 (5.03–5.19) 55 to <65 (years) 223,545 12,215 5.46 (5.37–5.56) Ethnic origin 1.76 0.180 Han 599,623 31,365 5.23 (5.17–5.29) Others 3459 163 4.71 (4.03–5.47) Marital status 143.71 <0.0001 Unmarried 5434 390 7.18 (6.50–7.90) Married 575,304 29,645 5.15 (5.10–5.21) Divorced 10,058 679 6.75 (6.27–7.26) Widowed 12,286 814 6.63 (6.19–7.08) Education 50.54 <0.0001 No schooling 82,890 4085 4.93 (4.78–5.08) Primary school 241,760 12,358 5.11 (5.02–5.20) Middle school 262,866 14,321 5.45 (5.36–5.54) High school or above 15,566 764 4.91 (4.57–5.26) Water source 108.43 <0.0001 Unprocessed water 145,517 8378 5.76 (5.64–5.88) Tap water 457,565 23,150 5.06 (5.00–5.12) BMI 30.33 <0.0001 <18.5 (kg/m2) 4595 312 6.79 (6.08–7.56) 18.5 to <24.0 (kg/m2) 249,192 13,162 5.28 (5.19–5.37) 24.0 to <28.0 (kg/m2) 274,270 14,281 5.21 (5.12–5.29) ≥28.0 (kg/m2) 75,025 3773 5.03 (4.87–5.19) Smoking 531.45 <0.0001 No 480,596 23,521 4.89 (4.83–4.96) Ever 122,486 8007 6.54 (6.40–6.68) Alcohol drinking 451.81 <0.0001 No 487,186 24,021 4.93 (4.87–4.99) Ever 115,896 7507 6.48 (6.34–6.62)BMI: Body mass index; CI: Confidence interval; HBsAg: Hepatitis B surface antigen.
 Figure 1:
Figure 1: Prevalence of positive HBsAg among the study participants by age group. HBsAg: Hepatitis B surface antigen. Whiskers show the 95% confidence interval.
 Figure 2:
Figure 2: Prevalence of positive HBsAg among the study participants by sex according to different birth cohorts. HBsAg: Hepatitis B surface antigen. Whiskers show the 95% confidence interval.
 Figure 3:
Figure 3: Trends of positive HBsAg prevalence from 2015 to 2023 by sex. HBsAg: Hepatitis B surface antigen. Whiskers show the 95% confidence interval.
HBsAg positivity was slightly greater among Han Chinese individuals than among those of other ethnicities, but the difference was not statistically significant (5.23% vs. 4.71%, χ2 = 1.76, P = 0.180), possibly due to the small number of individuals of other ethnicities included in this study. HBsAg positivity gradually decreased with increasing BMI, which was consistent with the findings of a study conducted by Chu et al.[20] Compared with other groups, the unmarried group had the highest prevalence of HBsAg positivity, and HBsAg positivity rate was lowest among individuals with a high school education or above. Among individuals using unprocessed water, the prevalence of HBsAg was greater than that of individuals using tap water (5.76% vs. 5.06%, χ2 = 108.43, P <0.0001). The HBsAg positivity rate was greater among individuals who smoked and consumed alcohol. Analyses stratified by sex were performed to exclude the potential impact of sex differences on the prevalence of HBV infection associated with smoking status and alcohol consumption. The findings revealed that among both males and females, individuals who smoked and consumed alcohol exhibited greater HBsAg positivity rates than those who did not smoke or consume alcohol [Figure 4].
 Figure 4:
Figure 4: Prevalence of positive HBsAg associated with smoking status (A) and alcohol drinking (B) by sex. HBsAg: Hepatitis B surface antigen. Whiskers show the 95% confidence interval.
DiscussionIn this study, we performed an up-to-date assessment of HBV infection and associated risk factors among populations eligible for HCC screening in China during the period of 2015–2023. We found that the overall prevalence was 5.23%.
This study revealed a greater prevalence of HBV infection among males than females, consistent with data from China’s national survey in 2006, which also reported significantly greater HBsAg positivity rate in males than in females aged 15–59 years.[13] Moreover, two extensive national surveys focusing on males and females of reproductive age also confirmed a greater prevalence of HBV infection in males than in females.[21,22] Studies have demonstrated that the androgen pathway can increase the transcription of HBV through direct binding to androgen-responsive element sites in viral enhancer I, which may explain why males are more susceptible to HBV infection than females are.[23,24] Coupled with a higher frequency of alcohol consumption and smoking among males, which have been shown to have a multiplicative effect on HBV-related HCC risk,[25] these factors may partly account for the male predominance in liver cancer incidence in China, exceeding that in females by approximately three times. These findings underscore the importance for males to prioritize protective measures against HBV infection and to prevent HCC.
This study revealed that the HBsAg positivity rate is lowest among individuals aged 35–54 years. The analysis of the age-specific prevalence of HBV infection revealed a gradual increase in HBV positivity rates with increasing age in both males and females. The HBV vaccination program was initiated in China in 1992 and integrated into the National Expanded Program on Immunization (EPI) in 2002.[26] Free routine immunization has been provided to all infants since 2005.[13] These preventive measures in China have been successful, leading to a continuous decline in the HBsAg positivity rate in the general population.[13,14] However, since all individuals in our study were born before 1992, the age-related changes in HBsAg positivity are unlikely to be due to the HBV vaccination program. The relatively low prevalence of HBV infection among younger individuals in China may be attributed to improvements in the medical service and capacity of healthcare institutions by increasing the healthcare workforce through education regulation, financial incentives, management and social system support.[27] The birth cohort analysis in this study also supported this finding.
During the period from 2015 to 2023, the HBsAg positivity rate slightly fluctuated annually but did not exhibit a clear upward or downward trend, remaining stable at approximately 5%. Specifically, the prevalence of HBV infection among individuals aged 55–64 years was 5.46%, which was comparable to the estimates made in the meta-analysis by Liu et al,[28] revealing a prevalence of 5.6% among the population aged over 60 years in China in 2021. This suggests that our results are reasonably robust. According to the trend of HBV prevalence in our study, it is estimated that within the next decade, the HBsAg positivity rate among all individuals born before 2002 who are eligible for HCC screening will be approximately 5%. Therefore, HCC screening in China should continue to focus on individuals with HBV infection as the target population until at least 2030. Moreover, although there is currently no definitive evidence to support the cost-effectiveness of liver cancer screening in patients with HBV infection, the expected incidence of HCC among Asian male hepatitis B carriers over the age of 40 years and Asian female hepatitis B carriers over the age of 50 years was 0.4–0.6% per year and 0.3–0.6% per year, respectively, both of which exceed the threshold incidence (0.2% per year) for HCC screening efficacy.[11] Therefore, continuing liver cancer screening in age-appropriate populations with CHB is feasible.
Finally, according to the 2020 China Population Census released by the National Bureau of Statistics (2021), there are approximately 0.31 billion males aged 35–64 years and 0.20 billion females aged 45–64 years in China, with an estimated total of 26.9 million individuals with HBV infection among these age groups. Efforts should be made to increase the coverage of HCC screening to ensure that more individuals with HBV can undergo HCC screening, thus improving the five-year survival rate of patients with liver cancer in China, which aligns with the key targets of the Healthy China 2030 program. However, further robust evidence is needed to determine whether HCC screening among individuals with HBV infection could reduce liver cancer mortality, and cost-effectiveness analysis should be conducted to determine the trade-offs between the benefits and harms of HCC screening in China.
Our study should be interpreted in light of its limitations. First, all the participants were recruited by means of phone-calls and personal encounter, potentially introducing selection bias, as individuals who are reachable by phone or encountered in person may not represent the broader population. Second, due to the predominant implementation of China’s national liver cancer screening program in eastern and central provinces, our investigation focused primarily on these regions, omitting western provinces. This could potentially lead to an overestimation or underestimation of the current HBV prevalence in China. While, according to two national investigations of HBV infection among men and women of reproductive age, HBV prevalence in western provinces of China falls between that of eastern and central provinces.[21,22] Consequently, our findings may closely approximate the actual HBV prevalence rate in China. Finally, the baseline data in our study contains numerous missing values. Although we conducted multiple imputation to address these gaps, it is important to acknowledge that imputed data may result in inaccurate estimations of the association between pertinent risk factors and HBV infection.
In conclusion, the current prevalence of HBV infection remains high among individuals eligible for liver cancer screening in China. Liver cancer screening should continue by targeting the population with HBV infection until 2030. Furthermore, to achieve the Healthy China 2030 program target of improving the 5-year cancer survival rate by 15%, it is imperative for the government to increase the accessibility of liver cancer screening among individuals with HBV infection.
Comments (0)