
Remember me


To the Editor: Frailty status represents one of the core determinants for the individualization of glycated hemoglobin (HbA1c) targets in the elderly population. However, the most validated tools to quantify frailty, which are complex and involve multiple dimensions of assessment, are rarely used in the clinical practice of diabetes management. Therefore, a simple and practical metric for the evaluation of frailty is needed. Grip strength is an easily measurable, objective, and reproducible metric for assessing frailty status.[1] It is correlated with overall muscle strength and has been reported to be significantly related to important health outcomes both in the general population[2,3] and in patients with diabetes.[4] Therefore, grip strength could be a useful marker for patient stratification in diabetes management. In this context, this study aimed to examine the associations between HbA1c and all-cause mortality across categories of grip strength, as a measure of frailty status, in older adults with type 2 diabetes in the UK Biobank. The researches had applied to access the UK Biobank database with the application approval number of 82812.
Our study was restricted to the participants with type 2 diabetes who were >65 years old and had valid data on grip strength, HbA1c, and all-cause mortality from the UK Biobank study. Handgrip strength was assessed using a hydraulic hand dynamometer (Jamar J00105). The average of left- and right-hand strengths was used in the subsequent analysis. The study population was then categorized into three groups according to sex-specific tertiles of grip strength (men: ≤32.0 kg, 32.1–40.0 kg, and >40.0 kg; women: ≤18.0 kg, 18.1–24.0 kg, and >24.0 kg). The primary outcome was all-cause mortality. The secondary outcome was a composite including myocardial infarction, stroke, heart failure, and cardiovascular death. Continuous variables with a normal or non-normal distribution were presented as mean ± standard deviation (SD) or median with interquartile range, respectively, and categorical variables as percentages (%). The Cox proportional hazard models were used to investigate the associations between HbA1c categories (<6.0%, 6.0%–6.9% [reference group], 7.0%–7.9%, and ≥8.0%) and outcomes among all participants or participants across the sex-specific tertiles of grip strength. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. The restricted cubic splines nested in time-dependent Cox models were fitted to explore the patterns of associations (linear or non-linear) between HbA1c and all-cause mortality. Statistical significance was considered to be P <0.05. All statistical analyses were performed by using R statistical software (version 3.2.0, https://www.r-project.org).
Of the 6494 participants finally included in this analysis, 1799 (27.7%) died over a median follow-up period of 12.3 (11.4–13.2) years. The baseline characteristics of the study population are summarized in Supplementary Table 1, https://links.lww.com/CM9/B950. In total participants, grip strength was significantly and linearly associated with the risk of all-cause mortality, after controlling for potential confounders (data not shown).
In the lowest tertile of grip strength, compared to patients with HbA1c 6.0–6.9%, the risk of all-cause mortality was significantly heightened by 35% in those with HbA1c ≥8.0% (HR 1.35, 95% CI 1.06–1.71) but not in individuals with HbA1c 7.0–7.9% (HR 1.03, 95% CI 0.84–1.25) or HbA1c <6.0% (HR 1.01, 95% CI 0.82–1.24) [Supplementary Table 2, https://links.lww.com/CM9/B950]. In the middle tertile of grip strength, virtually identical results were noted. In contrast, in the highest tertile of grip strength, the risk of all-cause mortality decreased by 27% (HR 0.73, 95% CI 0.55–0.96) in subjects with HbA1c <6.0% compared to those with HbA1c 6.0–6.9%, while the mortality risk did not significantly increase in those with HbA1c 7.0% and above.
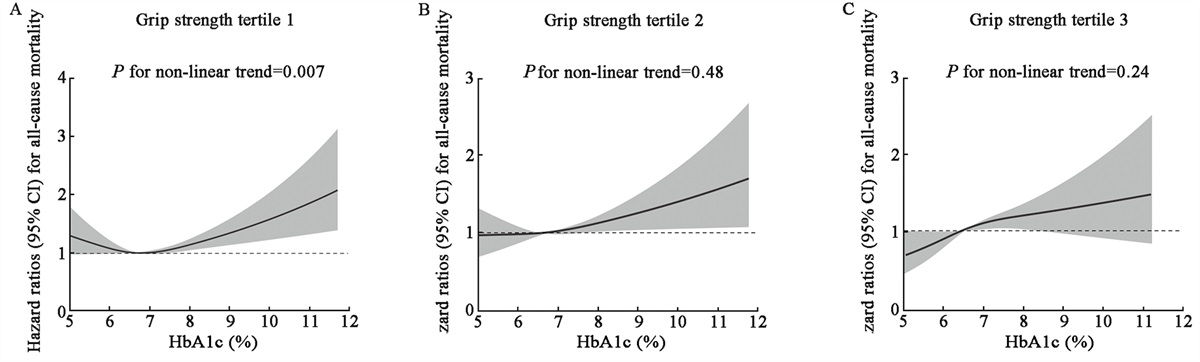
Figure 1 illustrates the results of the restricted cubic spline analyses. A U-shaped association (Pnon-linearity = 0.007) between HbA1c, as a continuous variable, and the risk of all-cause mortality in patients with the lowest tertile of grip strength was readily observed. In subjects with the middle and highest tertiles of grip strength, there was a roughly linear relationship between HbA1c and all-cause mortality (both Pnon-linearity >0.05). However, a significantly decreased risk of all-cause mortality associated with a lower HbA1c was only found in patients with the highest grip strength tertile. When the analyses were stratified by sex, BMI, and the use of sulfonylureas and/or insulin, similar findings were noted [Supplementary Figure 1, https://links.lww.com/CM9/B950].
 Figure 1:
Figure 1: Association between HbA1c and all-cause mortality in different grip strength groups using restricted cubic spline analysis. Grip strength tertile 1 (A): grip strength ≤18.0 kg in men and ≤32.0 kg in women; Grip strength tertile 2 (B): 32.1–40.0 kg in men, 18.1–24.0 kg in women; Grip strength tertile 3 (C): >40.0 kg in men, >24.0 kg in women. Adjusted for age, sex, ethnicity, Townsend deprivation index, education, employment, smoking status, drinking status, regular physical activity, healthy diet, BMI, triglycerides, total cholesterol, systolic blood pressure, diabetes duration, diabetes-related microvascular disease, history of cancer, history of cardiovascular disease, use of antihypertensive drugs, use of lipid-lowering drugs, and use of glucose-lowering drugs. BMI: Body mass index; HbA1c: Glycated hemoglobin; HR: Hazard ratio.
Additionally, in 5338 participants without a history of myocardial infarction, stroke, or heart failure, an HbA1c of <6% was significantly associated with an increased risk of incident cardiovascular outcome only in patients with the lowest tertile of grip strength, while an HbA1c of >8% was linked to a heightened risk of cardiovascular outcome only in those with the highest tertile of grip strength [Supplementary Table 3, https://links.lww.com/CM9/B950].
Frailty status is increasingly recognized by healthcare providers caring for the elderly. However, there is a lack of consensus definition and consensus assessment tools to date. As a proxy of physical frailty and sarcopenia, grip strength has gained much research interest in recent years. To date, there is scarce data about the potential modifying effect of grip strength on the relationship between HbA1c and all-cause mortality in older adults with type 2 diabetes. We found that a lower HbA1c was associated with a decreased risk of all-cause mortality only in patients with strong grip strength, while those with intermediate or weak grip strength should aim for a relatively higher HbA1c. Since frailty, assessed by grip strength in this study, is characterized by a decline in functioning across multiple physiological systems and increased vulnerability to stressors, it is reasonable to postulate that subjects with a high grip strength are more likely to be able to withstand the risks associated with intensified treatment regimens, such as severe hypoglycemia, and benefit from the lowered risk of diabetes-related outcomes secondary to the decrease in blood glucose. Of note, we conducted a subgroup analysis where patients were stratified by the use of sulfonylureas and/or insulin. Interestingly, in subjects without the use of sulfonylureas and/or insulin, in whom there is minimal risk of hypoglycemia, an apparent linear association between HbA1c and all-cause mortality was only observed in patients with the top tertile of grip strength, suggesting that other factors in addition to hypoglycemia may explain the benefits from a low HbA1c in this patient group. Furthermore, because grip strength is significantly correlated with cognitive function,[5] patients with high grip strength and therefore relatively intact cognitive function may have better self-management skills required for high-efficacy therapies, such as insulin.
Strengths of this study include a prospective study design in a large population-based sample of elderly people with type 2 diabetes, well-characterized baseline variables, and the objective measurement of grip strength by trained staff. There are several limitations that should be noted. Firstly, many of the socio-demographic and health status variables were recorded by self-report, and there may be measurement error, misclassification, or recall bias in the study. Secondly, due to the limited sample size and number of events of other major diabetes-related outcomes in the strata defined by grip strength and HbA1c, only all-cause mortality and a composite cardiovascular disease outcome were evaluated, and our study may still be underpowered in certain analyses, especially in the testing for interaction. Finally, although the UK Biobank cohort is a population-based cohort recruited from 22 centers across the UK, it is shown that the enrolled population is generally healthier than the general population,[6] which could be reflected by the relatively young age, well-controlled HbA1c, and short diabetes duration in our study. Therefore, the generalizability of our findings remains to be determined.
In conclusion, we found that the relationship of HbA1c with the risk of all-cause mortality varied across categories of grip strength, as a simple measure for frailty, in a representative sample of elderly patients with type 2 diabetes from the UK Biobank. Grip strength could identify those who may benefit from more intensive glucose control, which needs to be validated in future studies.
AcknowledgementsWe would like to thank all the involved clinicians and students for dedicating their time and skill to the completion of this study.
FundingThis work was supported by the Program of Shanghai Academic/Technology Research Leader (No. 22XD1402300), the Shanghai “Rising Stars of Medical Talent” Youth Development Program–Outstanding Youth Medical Talents (No. SHWSRS(2021)_099), the Shanghai Research Center for Endocrine and Metabolic Diseases (No. 2022ZZ01002), the National Natural Science Foundation of China (No. 31971485), and the Shanghai Municipal Key Clinical Specialty.
Conflicts of interestNone.
References 1. Bohannon RW. Grip strength: An indispensable biomarker for older adults. Clin Interv Aging 2019;14:1681–1691. doi: 10.2147/CIA.S194543. 2. Garcia-Hermoso A, Cavero-Redondo I, Ramirez-Velez R, Ruiz JR, Ortega FB, Lee DC, et al. Muscular strength as a predictor of all-cause mortality in an apparently healthy population: A systematic review and meta-analysis of data from approximately 2 million men and women. Arch Phys Med Rehabil 2018;99:2100–2113.e5. doi: 10.1016/j.apmr.2018.01.008. 3. Wu M, Wei Y, Lv J, Guo Y, Pei P, Li J, et al; China Kadoorie Biobank Collaborative Group. Associations of muscle mass, strength, and quality with all-cause mortality in China: a population-based cohort study. Chin Med J 2022;135:1358–1368. doi: 0.1097/CM9.0000000000002193. 4. Celis-Morales CA, Petermann F, Hui L, Lyall DM, Iliodromiti S, McLaren J, et al. Associations between diabetes and both cardiovascular disease and all-cause mortality are modified by grip strength: Evidence from UK biobank, a prospective population-based cohort study. Diabetes Care 2017;40:1710–1718. doi: 10.2337/dc17-0921. 5. Chou MY, Nishita Y, Nakagawa T, Tange C, Tomida M, Shimokata H, et al. Role of gait speed and grip strength in predicting 10-year cognitive decline among community-dwelling older people. BMC Geriatr 2019;19:186. doi: 10.1186/s12877-019-1199-7. 6. Fry A, Littlejohns TJ, Sudlow C, Doherty N, Adamska L, Sprosen T, et al. Comparison of sociodemographic and health-related characteristics of UK biobank participants with those of the general population. Am J Epidemiol 2017;186:1026–1034. doi: 10.1093/aje/kwx246.
Comments (0)