
Remember me


To the Editor: Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) show significant efficacy in patients with advanced-stage non-small cell lung cancer (NSCLC) with sensitive EGFR mutations and significantly prolong the survival of these patients. However, drug resistance emerges in most patients. Previous studies indicated that cyclin-dependent kinase 4/6 (CDK4/6) gene amplification was one of the resistance mechanisms of the EGFR-TKI osimertinib, weakening its efficacy. Treatment options for EGFR-mutant NSCLC patients with CDK4 amplification are limited to add CDK4 inhibitors.
Herein, we report two EGFR-mutant advanced NSCLC patients with co-occurring CDK4 amplification identified upon disease progression and associated with drug resistance. Both patients achieved significant and durable responses after monotherapy with afatinib, a second-generation EGFR-TKI. Informed consent has been obtained from the two patients.
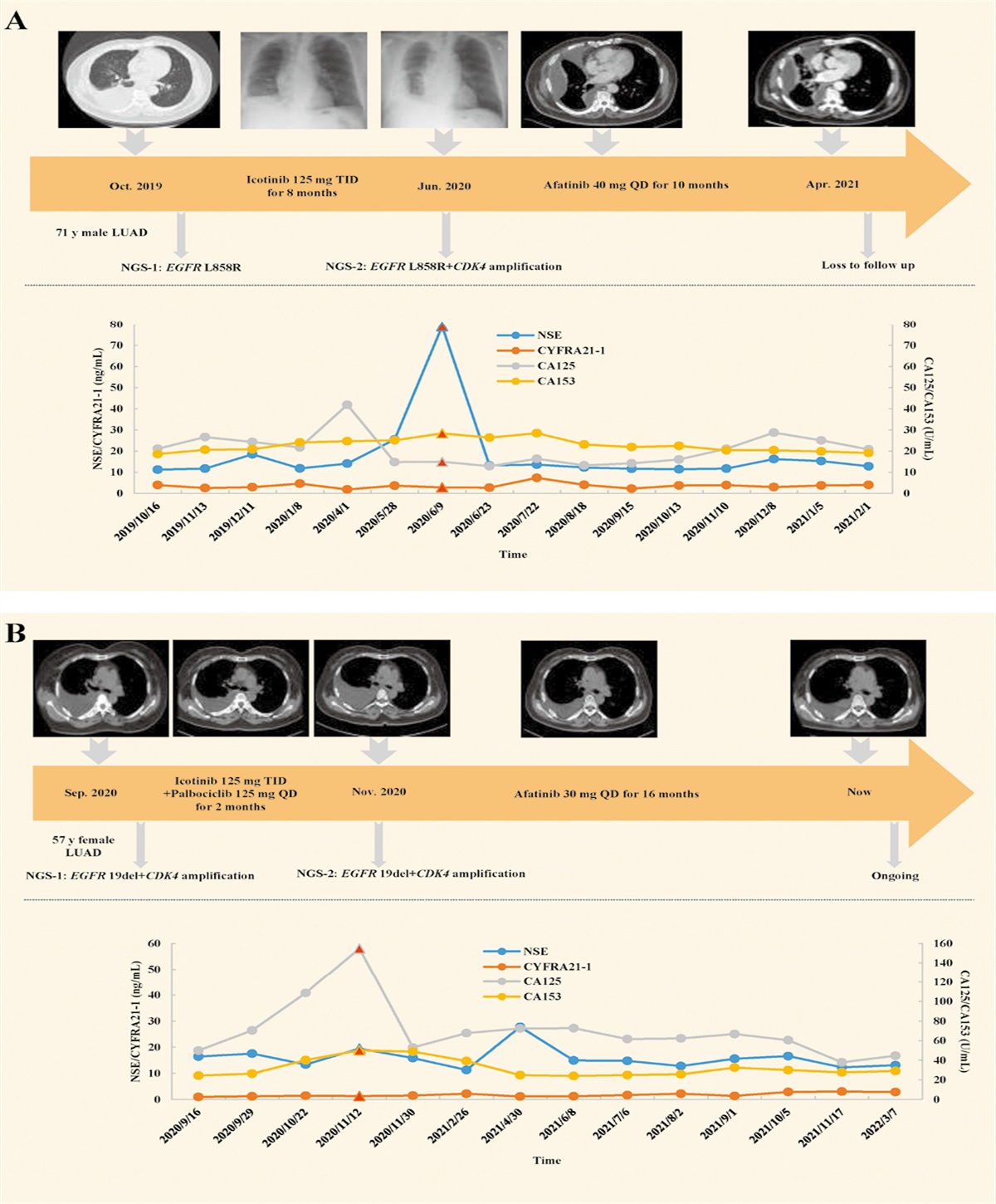
Patient #1 was a 71-year-old man who underwent chest computed tomography (CT) examination in October 2019 because of chest tightness and cough. CT scan revealed a 2.5 cm × 2.2 cm mass in the dorsal segment of the right lower lobe of the lung and multiple metastases, including intrapulmonary, pleural, and bone metastases. The patient had no comorbidities. The serum tumor markers test indicated that the cytokeratin 19 fragment (CYFRA21-1) value was slightly higher than the normal reference value. Cytopathological examination was conducted on pleural effusion and the results confirmed stage IVA lung adenocarcinoma (LUAD). Genetic testing of circulating tumor DNA (ctDNA) revealed EGFR L858R mutation (the detailed genetic testing methods and results have been provided in the Supplementary Materials [Supplementary Figure 1, https://links.lww.com/CM9/C5]).
The patient was initially treated with the first-generation EGFR-TKI icotinib (125 mg three times a day [TID]) starting from October 2019. Serum tumor markers were regularly reviewed during treatment, and the values were generally stable within the normal range. However, in June 2020, he experienced severe dyspnea and was incapacitated. Examination of serum tumor markers revealed that the neuron specific enolase (NSE) value reached a peak (79.06 ng/mL). Moreover, chest X-ray examination indicated massive effusion in the right pleural cavity. Pleural drainage was performed, and CDK4 amplification was detected using genetic testing of pleural effusion. Considering the genetic testing result and the patient’s economic condition, a second-generation EGFR-TKI afatinib (40 mg once daily [QD]) was initiated in June 2020. After 2 weeks of medication, the NSE value reduced remarkably to the normal reference range. Chest CT in July 2020 indicated no increment in effusion quantity. Therefore, afatinib (40 mg QD) was continued from July 2020. After four months, his symptoms dramatically improved, and chest CT showed that the metastasis lesions were smaller, with satisfying control of the primary lesion. The patient showed stable disease (SD) in radiologic evaluation, with serum tumor markers also stable during this period. The patient did not return for further treatment in April 2021 because of personal reasons [Figure 1A].
 Figure 1:
Figure 1: The therapeutic regimen and response evaluation of (A) patient #1 and (B) patient #2. Chest CT/X-ray shows the change of pleural effusion after indicated treatments. The line chart shows the trend of the values of the serum tumor markers over time. CA125: Cancer antigen 125; CA153: Cancer antigen 153; CDK4: Cyclin-dependent kinase 4; CT: Computed tomography; CYFRA21-1: Cytokeratin 19 fragment; EGFR: Epidermal growth factor receptor; LUAD: Lung adenocarcinoma; NGS: Next-generation sequencing; NSE: Neuron specific enolase; QD: Once daily; TID: Three times a day.
Patient #2 was a 57-year-old woman with no smoking history and comorbidity. In September 2020, the patient reported intermittent cough. CT examination of the chest revealed a 4.0 cm × 3.0 cm mass in the right upper lobe with a large pleural effusion and pulmonary atelectasis. Pleural drainage was performed, followed by cytopathological examination and genetic testing of pleural effusion. The results confirmed stage IVA LUAD, EGFR exon 19 deletion (19del) mutation and CDK4 amplification (the detailed genetic testing methods and results have been provided in the Supplementary Materials [Supplementary Figure 1, https://links.lww.com/CM9/C5]).
Based on the genetic testing results, a regimen of icotinib (125 mg TID) plus the CDK4 inhibitor palbociclib (125 mg QD) was administrated for 2 months starting in September 2020. Chest CT in November 2020 indicated the accumulation of more pleural effusion, and reexamination of serum tumor markers revealed that the values of cancer antigen 125 (CA125) and cancer antigen 153 (CA153) had continuously increased. Additionally, the metastasis lesion in the right middle lobe was enlarged. Following pleural drainage, genetic testing of pleural effusion detected EGFR 19del mutation and CDK4 amplification. Because of disease progression and economic burden, the patient changed to receive afatinib in November 2020. While the recommended dosage for afatinib is 40 mg daily, considering the tolerance issues of the patient, we administered the drug at a reduced dosage of 30 mg daily. After 2 weeks, the value of CA125 decreased markedly. Moreover, chest CT in January 2021 revealed that the metastasis tumor was significantly smaller, and the amount of pleural effusion was reduced. To date, this patient has continued this regimen and showed partial response (PR) in the CT examination. The tumor was under favorable control, with stable physical condition and serum tumor markers. Progression-free survival is over 16 months and continues to extend [Figure 1B].
CDK4/6 amplification was identified as one of the resistance mechanisms of osimertinib, and one study indicated that the presence of pretreatment CDK4/6 gene amplification could be used as a predictive biomarker for early drug resistance in patients with EGFR gene mutations.[1] However, few studies have focused on the treatment of patients harboring EGFR gene mutation combined with CDK4/6 gene amplification. One study reported that afatinib combined with the CDK4/6 inhibitor palbociclib could overcome secondary resistance to afatinib by inhibiting the phosphorylation of retinoblastoma (Rb) gene.[2] Here, we show that monotherapy of afatinib was effective in the treatment of EGFR-mutant NSCLC patients harboring CDK4 amplification. While patient #1 harbored CDK4 amplification, resulting in acquired resistance to icotinib, stable disease was observed after being administered afatinib. Patient #2, in which CDK4 amplification was detected at the time of diagnosis of LUAD, showed no response to icotinib plus palbociclib. The patient then received afatinib, and her symptoms improved and remained stable.
Chen et al[3] reported that afatinib induced a significant increase in the G1 phase arrest and a decrease in the S phase fraction in NCI-N87 cells. Furthermore, CDK4 and cyclin D1(CCND1) were downregulated after afatinib treatment, inhibiting proliferation in tumor cells. Liu et al[4] revealed that CDK4, CDK6, and CCND1 were downregulated, while cyclin-dependent kinase inhibitor 1A (CDKN1A) and cyclin-dependent kinase inhibitor 1B (CDKN1B), two negative regulators of the cell cycle, were upregulated after afatinib treatment for afatinib-sensitive esophageal squamous cell carcinoma tumor cells, indicating that afatinib could induce cell cycle arrest. This may be the mechanism underlying the effects of afatinib on EGFR-mutant NSCLC harboring CDK4 amplification.
We used the Connectivity Map (CMap) resource, an independent bioinformatics approach that was developed in 2006 by the Broad Institute, which provides the potential to reveal the connections among drugs, genes, and diseases.[5] Using CMap analysis, we explored the connection between various EGFR and CDK inhibitors in the A549 cell line, a commonly used NSCLC cell line. Afatinib achieved the highest connectivity score (94.99) among EGFR inhibitors to knock down the CDK4 gene [Supplementary Figure 2, https://links.lww.com/CM9/C5]. From these results, we considered afatinib a potentially effective drug in NSCLC patients harboring EGFR mutation and CDK4 amplification.
To further explore the interactions between CDK4 and potential drugs, we performed molecular docking analysis using AutoDock Vina (https://vina.scripps.edu/), a new program for molecular docking and virtual screening, which was originally designed and implemented by Dr. Oleg Trott in the Molecular Graphics Lab (now CCSB) at The Scripps Research Institute. A binding energy <−7.000 kcal/mol indicates that a ligand and receptor have strong binding activity. We used AutoDock Vina to calculate the fitting of CDK4 with the CDK4 inhibitor palbociclib, as a positive control, and the results showed the docking binding energy was −9.085 kcal/mol. We also performed docking calculations for CDK4 with icotinib, erlotinib, afatinib, and osimertinib, different kinds of EGFR-TKIs. The results showed two binding sites of afatinib and CDK4, and the docking binding energy was −8.403 kcal/mol, suggesting a significant affinity; the other EGFR-TKIs showed no correlations [Supplementary Figure 3, https://links.lww.com/CM9/C5].
As previously described, the analysis results of CMap resource and AutoDock Vina could provide a theoretical basis for identifying afatinib as a potential drug for NSCLC patients harboring CDK4 amplification. In conclusion, afatinib may be a promising option with potential efficacy for NSCLC patients with EGFR mutation and CDK4 amplification. More clinical research with a large sample size is required in the future.
AcknowledgementsSupplementary Figure 2A, https://links.lww.com/CM9/C5 was created with the aid of BioRender.com. We thank Liwen Bianji, Edanz Editing China (www.liwenbianji.cn/ac), for editing the English text of a draft of this manuscript.
FundingThis study was supported by grants from China National Science Foundation (Nos. 82022048 and 82373121), the Science and Technology Planning Project of Guangzhou (No. 202206080013); and the National Key Research & Development Program (No. 2022YFC2505100).
Conflicts of interestNone.
References 1. Sitthideatphaiboon P, Teerapakpinyo C, Korphaisarn K, Leelayuwatanakul N, Pornpatrananrak N, Poungvarin N, et al. Co-occurrence CDK4/6 amplification serves as biomarkers of de novo EGFR TKI resistance in sensitizing EGFR mutation non-small cell lung cancer. Sci Rep 2022;12:2167. doi: 10.1038/s41598-022-06239-y. 2. Nie H, Zhou X, Shuzhang D, Nie C, Zhang X, Huang J. Palbociclib overcomes afatinib resistance in non-small cell lung cancer. Biomed Pharmacother 2019;109:1750–1757. doi: 10.1016/j.biopha.2018.10.170. 3. Chen Z, Liu Z, Zhang M, Huang W, Li Z, Wang S, et al. EPHA2 blockade reverses acquired resistance to afatinib induced by EPHA2-mediated MAPK pathway activation in gastric cancer cells and avatar mice. Int J Cancer 2019;145:2440–2449. doi: 10.1002/ijc.32313. 4. Liu Z, Chen Z, Wang J, Zhang M, Li Z, Wang S, et al. Mouse avatar models of esophageal squamous cell carcinoma proved the potential for EGFR-TKI afatinib and uncovered Src family kinases involved in acquired resistance. J Hematol Oncol 2018;11:109. doi: 10.1186/s13045-018-0651-z. 5. Subramanian A, Narayan R, Corsello SM, Peck DD, Natoli TE, Lu X, et al. A next generation connectivity map: L1000 platform and the first 1,000,000 profiles. Cell 2017;171:1437–1452.e1417. doi: 10.1016/j.cell.2017.10.049.
Comments (0)