
Remember me


Non-alcoholic fatty liver disease (NAFLD) is currently the most prevailing etiology of chronic liver disease.[1] NAFLD is a disease that progresses from steatosis to irreversible steatohepatitis, liver fibrosis, cirrhosis, and finally liver cancer.[2] Although less than 10% of NAFLD patients develop cirrhosis and liver cancer within 10–20 years of diagnosis, this remains a great concern for the medical community given the high prevalence of the disease.[3]
Hypertension is one of the main risk factors for cardiovascular disease, affecting an estimated 30% of the global population.[4] It is worth noting that a cross-sectional multicenter study found that compared to normotensive youth, hypertensive youth had an increased body mass index (BMI), insulin resistance (IR), and liver steatosis.[5] Therefore, the 2016 joint guidelines from the European Association for the Study of Liver (EASL), Diabetes (EASD), and Obesity (EASO) recommend that non-alcoholic steatohepatitis patients with fibrosis associated with hypertension should receive closer monitoring.[6] However, hypertension and NAFLD often co-exist in the same individual in a complex two-way relationship as they share common metabolic risk factors, such as age, obesity, and IR.[7] Existing observational studies are also subject to a few limitations, such as small sample sizes, and are usually influenced by confounding and reverse causation. Therefore, it is difficult to obtain definitive proof of an independent association between hypertension and NAFLD.[8]
The National Health and Nutrition Examination Survey (NHANES) is a continuing cross-sectional study carried out by the National Center for Health Statistics (NCHS) that aims to evaluate the nutritional status and emerging public health conditions of the American population.[9] Therefore, NHANES can provide high-quality, large-sample, and nationally representative data to evaluate the correlation between hypertension and NAFLD risk.
Mendelian randomization (MR) analyses have been recognized as a complementary approach to randomized controlled trials (RCTs) and have been widely regarded as an emerging epidemiology method that evaluates the causal effects of exposure on a particular outcome using genetic variables.[10,11] Furthermore, the results of the MR approach are less susceptible to residual confounding and reverse causality bias as the genetic variants are randomly allocated during meiosis and are not correlated with environmental factors.[12]
In this study, we combined a large-scale observational study in the NHANES 2017–2018 and a two-sample MR analysis to comprehensively assess the relationship between hypertension and NAFLD.
Methods Study population in NHANESThe data used in the current analysis are publicly available through the NHANES database (https://www.cdc.gov/nchs/nhanes/index.htm). The protocols of the NHANES study were authorized by the Research Ethics Review Board of NCHS. Informed consent was obtained from all the NHANES participants. The study was exempt from the approval of the institutional review board as it used de-identified, publicly available data.
The study's inclusion criteria comprised participants who were enrolled in the NHANES Mobile Examination Center in 2017–2018 and met the following conditions: age of 20 years or above, and authorization for elastography measurements using FibroScan 502 Touch (Echosens, Paris, France).[13] The study sample consisted of 5569 individuals who fulfilled these eligibility criteria. Exclusion criteria were as follows: (1) individuals with ineligible, not performed, or partial elastography examination status (N = 1059); (2) missing controlled attenuation parameter (CAP, which can quantify the steatosis degree) data (N = 1); (3) individuals who were infected with hepatitis B (defined by the presence of hepatitis B surface antigen) or hepatitis C (positive for hepatitis C antibodies or hepatitis C RNA) (N = 118); (4) individuals with significant alcohol consumption (individuals who drink an average of one to two or more standardized drinks per day, respectively) or missing information about alcohol consumption (N = 938); (5) taking steatogenic drugs (such as amiodarone, methotrexate, and tamoxifen) for at least 3 months before study recruitment (N = 24); and (6) missing information regarding blood pressure values (N = 285). Finally, this study consisted of 3144 participants [Supplementary Figure 1, https://links.lww.com/CM9/B606].
Definition and assessment of hypertension and NALFD in NHANESProtocols used for blood pressure measurements followed procedures established by the American Heart Association. After measuring blood pressure thrice under quiescent conditions, the average values of systolic blood pressure (SBP) and diastolic blood pressure (DBP) were calculated. The 2017 American Heart Association/American College of Cardiology (AHA/ACC) guideline recommended that individuals with an SBP ≥130 mmHg and/or DBP ≥80 mmHg should be defined as having hypertension.[14] Meanwhile, participants who answered "yes" to the question: "Ever told you had high blood pressure?" are also classified as having hypertension.
NAFLD is traditionally diagnosed by either imaging or histological pathways to determine the presence of hepatic steatosis. NHANES staff used the FibroScan 502 Touch device to evaluate participants for vibration-controlled transient elastography (VCTE) from 2017 to 2018. The FibroScan 502 Touch device can be used to measure the ultrasound attenuation related to the degree of NAFLD and record the CAP as the indicator for levels of fat in the liver. The CAP value is positively associated with the severity of NAFLD. We utilized a cutoff value of 285 dB/m for CAP as the marker for NAFLD status. This cutoff value, which exhibits an 80% sensitivity and 77% specificity, has been developed and validated in the United States population for detecting hepatic steatosis in individuals.[15]
Other covariates used in NHANESTo control the potential confounding effects, the following demographic characteristics were adjusted: sex, age, race, educational levels, BMI, waist circumference, smoking and diabetes status, total cholesterol, triglycerides, high-density lipoprotein (HDL)-cholesterol, glycosylated hemoglobin (HbA1c), and physical activity. We selected these confounders based on their associations with the outcomes of interest or a change in effects estimate of more than 10%. The smoking status of participants was categorized into never, former, and current smokers. It is distinguished on the condition of whether they have smoked less than 100 cigarettes during their lifetime and whether they do so now. Diabetes was defined as a history of previous diabetes, HbA1c level ≥6.5%, or fasting blood glucose level ≥126 mg/dL. Physical activity was classified into low (<600 min/week), moderate (≥600 min/week and <8000 min/week), and high levels (≥8000 min/week) according to the metabolic equivalent of the task.
Genome-wide association study (GWAS) sources and single nucleotide polymorphisms (SNPs) selectionThe genetic variants strongly related to hypertension were derived from the MRC Integrative Epidemiology Unit (MRC-IEU) consortium, which enrolled 462,933 Europeans (119,731 cases and 343,202 controls) in total. Data for SBP and DBP were collected from a meta-analysis of GWAS, which included 757,601 participants from the UK Biobank and the International Consortium of Blood Pressure (ICBP) consortium.[16] Moreover, we obtained a summary of data for genetic associations with NAFLD from the FinnGen GWAS, which enrolled 894 cases and 217,898 controls. NAFLD used in the Finngen cohort referred to the fatty replacement of the hepatic parenchyma that was not related to alcohol use and was diagnosed according to the International Classification of Diseases (ICD)-10 K76.0 (both hospital discharge and cause of death). These GWAS data were downloaded from the Integrative Epidemiology Unit (IEU) OpenGWAS database (https://gwas.mrcieu.ac.uk/).[17] All studies were reviewed and approved by local institutional review boards, and all participants provided informed consent.
To identify the genetic variations that can be used for the estimation of causal effects between exposures (hypertension, SBP, and DBP, respectively) and NAFLD, the genome-wide significance level was set at P <5×10-8 to screen the genetic variant that strongly associated with the exposure. Furthermore, we excluded those SNPs with linkage disequilibrium (r2 <0.001, 10,000 kb). Then, the PhenoScanner database was used to check each SNP to eliminate the SNPs that were significantly related to the potential confounders and other NALFD-related characteristics. Finally, 144, 286, and 302 SNPs for hypertension, SBP, and DBP, respectively, were extracted for the subsequent causality analysis [Supplementary Table 1, https://links.lww.com/CM9/B606]. Considering the effect of metabolic factors on NAFLD, we excluded potential confounders including BMI, waist circumference, other cardiovascular diseases, diabetes, dyslipidemia, drinking, and smoking.[18] Details information about data downloading and screening are displayed in Table 1.
Table 1 - Characteristics of GWAS enrolled in the MR study. Items GWAS ID Consortium Sample size No. of strongly related SNPs No. of enrolled SNPs Population Hypertension ukb-b-14057 MRC-IEU 462,933 225 144 Europeans SBP ieu-b-38 ICBP 757,601 461 286 Europeans DBP ieu-b-39 ICBP 757,601 460 302 Europeans NAFLD finn-b-NAFLD FinnGen 218,792 – – EuropeansDBP: Diastolic blood pressure; GWAS: Genome-wide association study; ICBP: International Consortium of Blood Pressure; MR: Mendelian randomization; MRC-IEU: MRC Integrative Epidemiology Unit; NAFLD: Non-alcoholic fatty liver disease; SBP: Systolic blood pressure; SNPs: Single nucleotide polymorphisms.
When performing NHANES analysis, we implemented multivariate-adjusted logistic regression to assess the relationship between hypertension, SBP, DBP, and NAFLD. Three models adjusted for covariates were assessed: Model 1 was not adjusted; Model 2 included gender, age, race, and education level; Model 3 was additionally adjusted for age, gender, race, education level, BMI, waist circumference, total cholesterol, triglycerides, HDL-cholesterol, diabetes, HbA1c, smoking status, and physical activity class. Results are presented as odds ratios (ORs) or β coefficients (95% confidence interval [CI]). Given the complex probabilistic clustering design of NHANES, weights were considered in statistical analyses in this study.
As for the two-sample MR analysis, we applied inverse variance weighted (IVW) as the principal method to assess the causal association of genetically predicted hypertension, SBP, DBP, and NAFLD risk. Furthermore, four complementary MR analysis methods were used, including MR Egger, weighted median, weighted mode, and MR-Pleiotropy residual sum and outlier (MR-PRESSO), to validate the results from IVW. Since the IVW estimates may be biased by introducing pleiotropic instrumental variables, the pleiotropic effects in the causal estimates were resolved by sensitivity analyses. Cochrane's Q test was used to evaluate the potential heterogeneity. A random-effects IVW analysis was used to adjust the measured heterogeneity (P <0.05). Next, the intercept of MR-Egger was adopted to estimate the horizontal pleiotropy of the genetic variants (P <0.05 was considered as the potential presence of horizontal pleiotropy). MR-PRESSO was also used to assess the presence of pleiotropy by comparing the observed residual sum of squares with the expected residual sum of squares. Moreover, the leave-one-out analysis was performed to determine whether the results were driven by individual variants.
R software, version 4.1.3 (R Foundation, Vienna, Austria) and EmpowerStats software (X&Y Solutions Inc., Boston, MA, USA) were used to perform all statistical analyses.
Results Population characteristics of study subjects according to NAFLDTable 2 shows the clinical and laboratory features of the study participants. Participants were classified into 1929 individuals with NAFLD and 1215 individuals without NAFLD according to the cutoff value of 285 dB/m for CAP. Patients with NAFLD were older, predominantly male, and of a non-Hispanic white ethnicity; additionally, they demonstrated a lower level of education and a higher prevalence of smoking, diabetes, and hypertension. Furthermore, as expected, they had significantly higher median stiffness, median CAP, BMI, waist circumference, SBP, DBP, alanine aminotransferase (ALT), aspartate transaminase (AST), alkaline phosphatase (ALP), γ-glutamyltransferase (GGT), uric acid, total cholesterol, triglycerides, high-sensitivity C-reactive protein (HS-CRP), HbA1c, and fasting glucose, while high-density lipoprotein (HDL)-cholesterol was lower.
Table 2 - Demographic and clinical characteristics of the participants with and without NAFLD. Items Non-NAFLD NAFLD Statistics P value Age (years) 48 (32, 62) 55 (41, 66) –7.052 <0.001* Gender 30.855 <0.001† Male 920 (47.7%) 703 (57.9%) Female 1009 (52.3%) 512 (42.1%) Race 60.735 <0.001† Mexican American 198 (10.3%) 222 (18.3%) Other Hispanic 519 (26.9%) 224 (18.4%) Non-Hispanic White 678 (35.1%) 456 (37.5%) Non-Hispanic Black 186 (9.6%) 113 (9.3%) Other race 348 (18.0%) 200 (16.5%) Education level‡ 14.784 0.001† High school 754 (39.1%) 526 (43.3%) Some college or AA degree 632 (32.8%) 422 (34.7%) College graduate or above 541 (28.1%) 267 (22.0%) Unknown 2 (0%) 0 (0%) Ratio of family income to poverty‡ 2.4 (1.2, 4.3) 2.2 (1.2, 4.3) –0.134 0.894* Physical activity‡ 5.607 0.061† Low level (<600 min/week) 212 (11.0%) 159 (13.1%) Moderate level (≥600 and <8000 min/week) 928 (48.1%) 529 (43.5%) High level (≥8000 min/week) 365 (18.9%) 211 (17.4%) Unknown 424 (22.0%) 316 (26.0%) Smoker status 25.011 <0.001† Never 1134 (58.8%) 642 (58.8%) Former 442 (22.9%) 376 (30.9%) Current 353 (18.3%) 197 (16.2%) BMI‡ 26.3 (23.2, 30.2) 32.7 (28.6, 37.6) –25.817 <0.001* Waist circumference (cm)‡ 92.7 (83.7, 102.7) 110.7 (100.0, 120.6) –28.052 <0.001* SBP 118.0 (108.8, 131.0) 124.3 (112.7, 138.7) –7.714 <0.001* DBP 71.3 (65.3, 79.0) 75.7 (68.3, 83.7) –9.598 <0.001* Median stiffness (kPa) 4.6 (3.8, 5.6) 5.6 (4.5, 7.0) –17.818 <0.001* Median CAP (dB/m) 230.0 (200.0, 258.0) 327.0 (302.0, 351.3) –47.284 <0.001* Hypertension 132.150 <0.001† No 978 (50.7%) 363 (29.9%) Yes 951 (49.3%) 852 (70.1%) Diabetes 201.289 <0.001† No 1697 (88.0%) 816 (67.2%) Yes 232 (12.0%) 399 (32.8%) Laboratory features‡ ALT (U/L) 16.0 (12.0, 23.0) 22.0 (16.0, 34.0) –16.732 <0.001* AST (U/L) 19.0 (16.0, 22.0) 20.0 (16.0, 27.0) –7.246 <0.001* ALB (g/dL) 4.0 (3.9, 4.3) 4.0 (3.8, 4.2) –2.406 0.016* ALP (IU/L) 71.0 (60.0, 86.0) 78.5 (65.0, 96.0) –8.842 <0.001* GGT (IU/L) 18.0 (13.0, 27.0) 25.0 (18.0, 38.0) –16.668 <0.001* Total bilirubin (mg/dL) 6.8 (5.1, 10.3) 6.8 (5.1, 10.2) –0.760 0.447 Uric acid (mg/dL) 5.1 (4.3, 6.0) 5.9 (4.9, 7.0) –12.692 <0.001* Total cholesterol (mmol/L) 4.7 (4.0, 5.4) 4.7 (4.1, 5.6) –3.208 0.001* Triglycerides (mmol/L) 1.0 (0.8, 1.5) 1.5 (1.2, 2.0) –19.664 <0.001* HDL-cholesterol (mmol/L) 1.4 (1.2, 1.7) 1.2 (1.0, 1.4) –17.134 <0.001* LDL-cholesterol (mmol/L) 2.7 (2.2, 3.4) 2.8 (2.3, 3.5) –1.051 0.293* HS-CRP (mg/L) 1.5 (0.7, 3.3) 2.9 (1.3, 5.9) –14.288 <0.001* HbA1c (%) 5.5 (5.2, 5.8) 5.9 (5.5, 6.5) –16.792 <0.001* Fasting glucose (mg/dL) 100.0 (95.0, 109.0) 112.0 (102.0, 130.0) –13.897 <0.001*Data were presented as median (interquartile range) or n (%). *Mann-Whitney U test for continuous variables. †Pearson's chi-squared test for categorical variables. ‡Presence of missing values. AA: Associate of arts; ALB: albumin; ALP: Alkaline phosphatase; ALT: Alanine aminotransferase; AST: Aspartate transaminase; BMI: Body mass index; CAP: Controlled attenuation parameter; DBP: Diastolic blood pressure; GGT: γ-Glutamyltransferase; HbA1c: glycosylated hemoglobin; HDL: High-density lipoprotein; HS-CRP: High-sensitivity C-reactive protein; LDL: Low-density lipoprotein; NAFLD: Non-alcoholic fatty liver disease; PRESSO: Pleiotropy residual sum and outlier; SBP: Systolic blood pressure.
The result of multivariate regression analysis depicted that there was a significant relationship between hypertension (OR = 1.677 [95% CI, 1.159–2.423]) and NAFLD risk [Table 3]. After adjustment for potential confounding, 130 mmHg ≤SBP <140 mmHg (OR = 1.802 [95% CI, 1.184–2.743]), SBP ≥140 mmHg (OR = 1.648 [95% CI, 1.073–2.531]), 80 mmHg ≤DBP <90 mmHg (OR = 1.397 [95% CI, 1.072–1.820]), and DBP ≥90 mmHg (OR = 1.513 [95% CI, 1.036–2.210]) were also significantly positively correlated with NAFLD. However, the significant correlation between 120 mmHg ≤SBP<130 mmHg and NAFLD becomes insignificant after adjusting for the covariates in Model 3 (OR = 1.564 [95% CI, 0.988–2.478]). Additionally, Table 4 depicts that hypertension was positively linked with CAP (β 7.836 [95% CI, 2.334–13.338]). Hypertension also exhibited a significant positive association with liver stiffness in Model 1 (β 1.142 [95% CI, 0.913–1.572]) and Model 2 (β 0.985 [95% CI, 0.411–1.559]). However, this significant relationship becomes insignificant after adjusting for the covariates in Model 3 (β –0.031 [95% CI, –0.761 to 0.699]).
Table 3 - Association between blood pressure categories and NAFLD. Items Model 1: OR (95% CI) Model 2: OR (95% CI) Model 3: OR (95% CI) Non-hypertension Reference Reference Reference Hypertension 3.126 (2.507, 3.898) 2.857 (2.067, 3.948) 1.677 (1.159, 2.423) SBP SBP <120 mmHg Reference Reference Reference 120 mmHg ≤ SBP < 130 mmHg 1.991 (1.493, 2.655) 1.712 (1.071, 2.736) 1.564 (0.988, 2.478) 130 mmHg ≤ SBP < 140 mmHg 1.931 (1.562, 2.386) 1.562 (1.223, 2.173) 1.802 (1.184, 2.743) SBP ≥140 mmHg 2.197 (1.628, 2.966) 1.661 (1.029, 2.682) 1.648 (1.073, 2.531) DBP DBP <80 mmHg Reference Reference Reference 80 mmHg ≤ DBP < 90 mmHg 2.102 (1.635, 2.702) 2.069 (1.472, 2.907) 1.397 (1.072, 1.820) DBP ≥90 mmHg 2.704 (1.913, 3.823) 2.609 (1.571, 4.333) 1.513 (1.036, 2.210)Model 1 adjusted for: none. Model 2 adjusted for: gender, age, race, and education level. Model 3 adjusted for: gender, age, race, education level, BMI, waist circumference, total cholesterol, triglycerides, HDL-cholesterol, diabetes, HbA1c, smoking status, and physical activity class. BMI: Body mass index; CI: Confidence interval; DBP: Diastolic blood pressure; HbA1c: Glycosylated hemoglobin; HDL: High-density lipoprotein; NAFLD: Non-alcoholic fatty liver disease; OR: Odds ratio; SBP: Systolic blood pressure.
Model 1:
β (95% CI)
Model 2:
β (95% CI)
Model 3:
β (95% CI)
Model 1:
β (95% CI)
Model 2:
β (95% CI)
Model 3:
β (95% CI)
Non-hypertension Reference Reference Reference Reference Reference Reference Hypertension 36.386 (29.769, 43.004) 29.324 (21.759, 36.888) 7.836 (2.334, 13.338) 1.142 (0.913, 1.572) 0.985 (0.411, 1.559) –0.031 (–0.761, 0.699)Model 1 adjusted for: none. Model 2 adjusted for: gender, age, race, and education level. Model 3 adjusted for: gender, age, race, education level, BMI, waist circumference, total cholesterol, triglycerides, HDL-cholesterol, diabetes, HbA1c, smoking status, and physical activity class. BMI: Body mass index; CAP: Controlled attenuation parameter; CI: Confidence interval; HbA1c: Glycosylated hemoglobin; HDL: High-density lipoprotein.
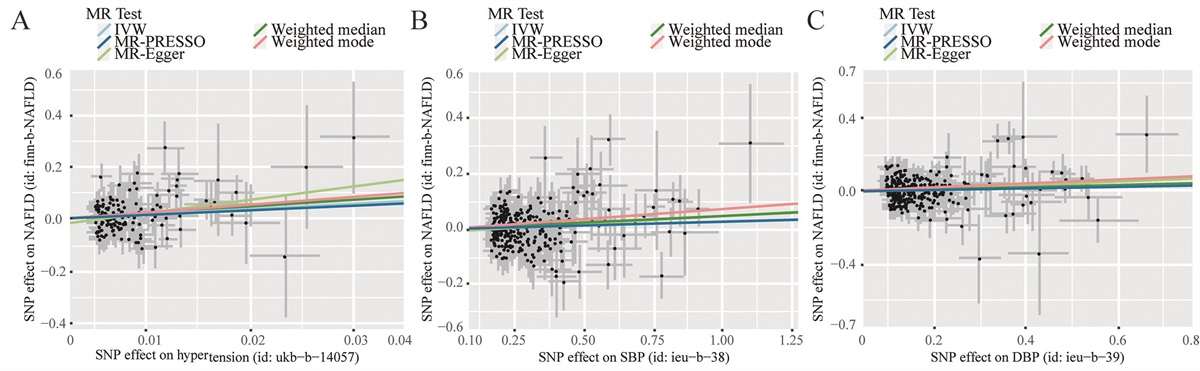
As the significantly positive correlation between hypertension and NAFLD risk was observed in the multivariable regression analysis mentioned above, we further conducted MR analysis to deduce the causal effects of hypertension on NAFLD risk. As shown in Table 5, results suggested that there were positive causal relationships between hypertension (OR = 7.203 [95% CI, 2.297–22.587]), SBP (OR = 1.024 [95% CI, 1.003–1.046]), and DBP (OR = 1.047 [95% CI, 1.005–1.090]) and NAFLD using the IVW method. Additionally, these results were consistent with other supplementary MR methods in terms of the direction of causal estimation and the magnitude of the causal effect, thus indicating that these findings are reliable and robust. Figure 1 depicted the effect estimates of exposure on NAFLD that were measured by different MR methods. The forest diagram was used to show the estimated effect of each SNP on NAFLD [Supplementary Figure 2, https://links.lww.com/CM9/B606].
Table 5 - MR estimates from each method of assessing the causal effect of hypertension on the risk of NAFLD. Exposure MR method β SE OR (95% CI) P vale for associationP value for heterogeneity test
P value for MR-Egger intercept
P value for MR-PRESSO global test
Hypertension IVW 1.975 0.583 7.203 (2.
Comments (0)