
Remember me


Reports indicate that, at the end of 2022, approximately 1.223 million patients with human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) have been living in China, with approximately 1.135 million patients receiving antiretroviral treatment (ART) among them.[1] In 2022, there were approximately 107,000 newly reported cases of HIV, predominantly among young- and middle-aged individuals in need of effective, safe, and convenient ART.[2] The primary goals of ART are to minimize viral load, maintain it at an undetectable level for as long as possible; restore immune system function; lower the incidence of HIV-related diseases; improve the overall quality of life; and decrease the transmission of the virus.[3]
ART has significantly prolonged the lives of HIV/AIDS patients. However, long-term adverse effects of ART, including metabolic syndrome and cardiovascular (CV) diseases, have also gradually emerged.[4,5] Long-term drug toxicity of ART is associated with metabolism disorders, leading to insulin resistance and dyslipidemia, which can in turn result in related chronic complications.[6] Additionally, HIV/AIDS patients receiving ART have twice the risk of CV disease compared to those without treatment.[7]
In China, most HIV/AIDS patients on ART primarily receive non-nucleoside reverse transcriptase inhibitors (NNRTIs) such as efavirenz (EFV), nevirapine (NVP), and protease inhibitors (PIs), with only a minority being treated with integrase strand transfer inhibitors (INSTIs). Notably, the adverse effects associated with raltegravir (RAL) and dolutegravir (DTG) are milder than those observed with older antiretroviral drugs.[8] Despite these advancements, up to half of the patients receiving the free first-line and second-line drugs report experiencing neuropsychiatric symptoms, dyslipidemia, and digestive side effects. These issues significantly affect treatment adherence and long-term therapeutic outcomes.[9]
The introduction of novel INSTIs, such as Biktarvy–a co-formulation of bictegravir, emtricitabine, and tenofovir alafenamide (BIC/FTC/TAF) marketed by Gilead Sciences aims to address the growing clinical need for effective HIV treatments. This single-tablet regimen offers rapid viral load reduction, improved safety profiles, and fewer drug interactions. Such benefits enhance patient convenience, significantly improving quality of life, and facilitating a return to normal activities.[10] BIC/FTC/TAF was included in the national medical insurance list in 2021, thus becoming more accessible to a broader demographic of Chinese HIV/AIDS patients. However, clinical reports on changes in blood lipid levels among patients treated with BIC/FTC/TAF are limited, with few studies exploring its impact on lipid metabolism in HIV/AIDS patients. For newly treated domestic HIV/AIDS patients, the short- and medium-term effects of the BIC/FTC/TAF regimen on blood lipids and related factors remain unclear. It is uncertain whether this INSTI regimen leads to adverse changes in blood lipids compared to, or not inferior to, those observed with the lamivudine, efavirenz, and tenofovir disoproxil fumarate (3TC+EFV+TDF) regimen or with previous antiretroviral drugs. This study aims to retrospectively evaluate the trend of blood lipid changes following the initiation of ART with BIC/FTC/TAF and 3TC+EFV+TDF at weeks 4, 12, 24, and 48, and to identify influencing factors among untreated male HIV/AIDS patients.
Methods Ethical approvalThis study was approved by the Ethics Review Committee of Beijing Youan Hospital, Capital Medical University (No. [2021]025). All participants who participated in this study provided their written informed consent, and all collected data were anonymous.
Study design and participantsThe case-control retrospective study was designed and conducted to collect general demographical, clinical, and laboratory data from newly treated HIV-infected individuals who visited the sexually transmitted disease (STD)/AIDS clinic at Beijing Youan Hospital, Capital Medical University between January and December 2021. These individuals initiated ART with either BIC/FTC/TAF or 3TC+EFV+TDF. The follow-up period extended from January to December 2022. The inclusion criteria were as follows: (1) a positive anti-HIV-1 or HIV RNA test, (2) aged 18 years or older, and (3) no history of receiving ART. Exclusion criteria were as follows: (1) patients with tumor or autoimmune disease, liver cirrhosis, etc., (2) those on cholesterol-lowering medications.
Data collected included general demographic characteristics such as age, sex, weight, height, possible route of HIV infection, and the date of HIV-Ab positivity. Laboratory tests performed included serum total cholesterol (TC), total triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), T lymphocyte subsets count, and HIV RNA load. The levels of TG, TC, HDL-C, and LDL-C were compared at baseline and 4 weeks, 12 weeks, 24 weeks, and 48 weeks after initiating ART to assess changes in blood lipid levels over these time points. Fasting blood samples were drawn into 10-mL ethylenediamine tetraacetic acid (EDTA) tubes according to clinical testing procedures and specifications. Within an hour of collection, the tubes were centrifuged at 3000 r/min for 10 min to separate the plasma, which was then stored at a temperature of −80°C until analysis. The levels of TG, TC, HDL-C, and LDL-C were assessed using enzymatic reagents (Trinder; Bayer Diagnostics, NY, USA) with an ADVIA 2400 automated analyzer (Siemens Healthineers, Marburg, Germany). Glucose levels were measured using the glucose hexokinase method. HIV-RNA levels were quantified using an automated real-time polymerase chain reaction-based m2000 system (Abbott Molecular Inc, Des Plaines, IL, USA, with a detection limit of 40 copies/mL), and CD4+ T cell counts were obtained with a flow cytometer (BD Biosciences, San Jose, CA, USA).
Diagnosis criteria for HIV infection were based on the AIDS Diagnosis and Treatment Guideline (2021).[3] In this study, elevated serum LDL-C (≥4.9 mmol/L) is selected as a predictor of dyslipidemia and diagnosis basis of hypercholesterolemia for analysis.[11,12] With body mass index (BMI) ≥24.0 kg/m2 considered overweight, 18.5–23.9 kg/m2 considered normal, and <18.5 kg/m2 considered underweight.[13] A fasting blood-glucose (FPG) level of ≥6.1 mmol/L or treatment with oral hypoglycemic agents or insulin is indicative of hyperglycemia.[14]
Statistical analysisStatistical analysis was performed using R 4.2.3 (R Foundation, Vienna, Austria). Descriptive analysis was conducted to describe demographic characteristics, behavior characteristics, and other variables of adult male HIV/AIDS patients. Continuous data were presented as mean ± standard deviation (SD) and compared between two groups using the Wilcoxon rank-sum test. Categorical data were presented as proportions and rates, and compared between two groups using the chi-squared test. The changes in indices at different time points were described, and a comparison with baseline values was made using Wilcoxon rank-sum tests, due to the skewed distribution of lipid data.
Augmented Dickey–Fuller (ADF) test was utilized to assess the stationarity of time series data, the change in lipid levels over time, based on the first order difference method. The ADF test, applied to the differenced data, indicated that the post-difference data were stationary (P <0.05). This suggests that the differenced data no longer exhibited a trend or serial correlation, representing a stable random process instead.
The Wilcoxon rank-sum test was also employed to compare the differences in lipid profiles between the two treatment groups at various time points. Additionally, line graphs were created to illustrate the trends of different lipid indicators among adult male HIV/AIDS patients receiving the two treatment regimens at various time points. A Cox regression analysis was initially performed to select univariate factors, followed by a multivariate Cox regression model, to identify relevant influencing factors for the population at high risk of increased LDL-C. A P-value <0.05 was considered statistically significant for this analysis.
Results Baseline characteristics of HIV/AIDS patients initiating ART with BIC/FTC/TAF or 3TC+EFV+TDFA total of 917 individuals were assessed for eligibility, and 870 individuals who received at least one follow-up blood lipid examination after initiating ART with BIC/FTC/TAF (n = 510) or 3TC+EFV+TDF (n = 360) were enrolled in this study. There were no statistically significant differences in median age (32.0 years vs. 34.0 years, t = 1.843, P = 0.066), baseline CD4/CD8 ratio and median BMI (22.6 kg/m2vs. 22.4 kg/m2, t = 0.403, P = 0.687) between the two groups, but there were statistically significant differences in CD4+ cell count (311.3 cells/μL vs. 350.0 cells/μL, t = 2.285, P = 0.023), and HIV-1 RNA (25,876.5 copies/mL vs. 18,815.0 copies/mL, t = 3.514, P <0.001) between BIC/FTC/TAF and 3TC+EFV+TDF groups [Supplementary Table 1, https://links.lww.com/CM9/C14].
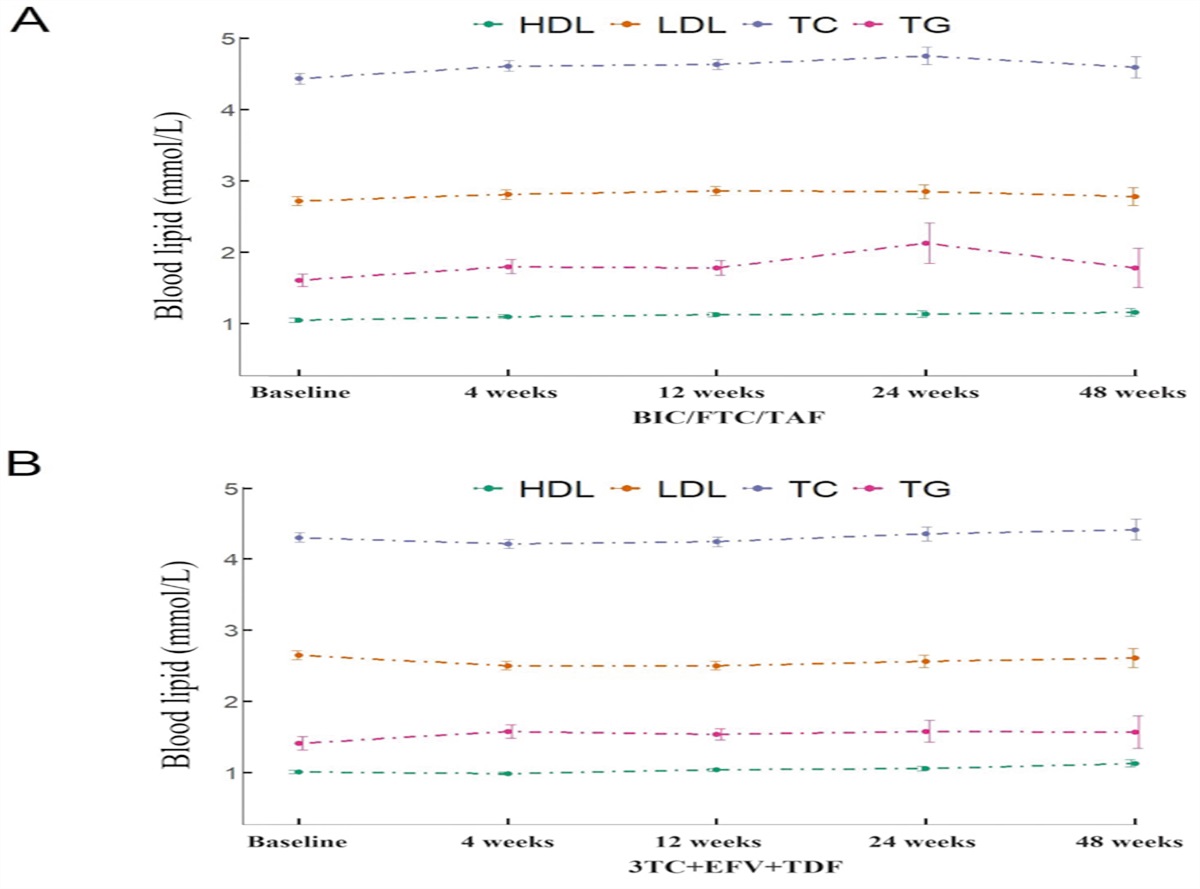
Trend of blood lipid among HIV/AIDS patients at different time points after treatment with BIC/FTC/TAF or 3TC+EFV+TDFIn the BIC/FTC/TAF group, the levels of TG, TC, and LDL-C were higher at 4 weeks, 12 weeks, and 24 weeks of treatment (all P <0.05 for TG, TC, and LDL-C), while HDL-C levels were significantly higher at 4 weeks, 12 weeks, 24 weeks, and 48 weeks of treatment (all P <0.001) compared to the baseline [Table 1]. However, the differences in TG, TC, and LDL-C levels between the baseline and 48 weeks in the BIC/FTC/TAF group were not statistically significant (TG: 1.61 mmol/L vs. 1.78 mmol/L, Z = 24,577, P = 0.719; TC: 4.43 mmol/L vs. 4.59 mmol/L, Z = 26,926, P = 0.0621; LDL-C: 2.72 mmol/L vs. 2.78 mmol/L, Z = 26,363, P = 0.132), indicating that the median changes in these blood lipid parameters at 48 weeks compared to baseline were not clinically meaningful. Despite some indicators showing elevation, they remained within the normal range, and median changes of lipid profiles over time were stationarity.
Table 1 - Comparison of blood lipid by BIC/FTC/TAF and 3TC+EFV+TDF groups of treatment-naïve adult male patients with HIV/AIDS at different time points. Characteristics Baseline 4 weeks 12 weeks 24 weeks 48 weeks ADF‡ P-value Mean ± SD Mean ± SD D* Z † P-value Mean ± SD D* Z † P-value Mean ± SD D* Z † P-value Mean ± SD D* Z † P-value TG (mmol/L) BIC/FTC/TAF 1.61 ± 1.01 1.80 ± 1.18 0.08 144,889 0.019 1.78 ± 1.21 0.10 142,280 0.032 2.13 ± 2.33 0.15 70,119 0.022 1.78 ± 1.41 0.06 24,577 0.719 –20.345 <0.001 3TC+EFV+TDF 1.41 ± 1.13 1.58 ± 1.13 0.13 106,254 <0.001 1.54 ± 0.94 0.15 81,877 0.013 1.58 ± 1.25 0.03 36,207 0.134 1.57 ± 1.15 0.13 21,710 0.219 –18.816 <0.001 TC (mmol/L) BIC/FTC/TAF 4.43 ± 0.90 4.61 ± 0.90 0.23 148,427 0.002 4.63 ± 0.86 0.26 150,865 <0.001 4.75 ± 1.01 0.30 75,425 <0.001 4.59 ± 0.78 0.20 26,926 0.062 –20.235 <0.001 3TC+EFV+TDF 4.31 ± 0.82 4.22 ± 0.78 –0.08 87,870 0.101 4.25 ± 0.80 –0.06 70,077 0.187 4.36 ± 0.80 0.01 32,334 0.698 4.42 ± 0.73 0.12 21,910 0.165 –19.817 <0.001 HDL-C (mmol/L) BIC/FTC/TAF 1.05 ± 0.41 1.10 ± 0.32 0.09 154,837 <0.001 1.13 ± 0.36 0.10 158,488 <0.001 1.14 ± 0.38 0.09 76,694 <0.001 1.16 ± 0.29 0.14 30,793 <0.001 –21.078 <0.001 3TC+EFV+TDF 1.01 ± 0.27 0.99 ± 0.25 0 90,913 0.413 1.04 ± 0.25 0.03 80,339 0.046 1.06 ± 0.26 0.08 36,322 0.006 1.13 ± 0.26 0.15 25,964 <0.001 –19.380 <0.001 LDL-C (mmol/L) BIC/FTC/TAF 2.72 ± 0.76 2.81 ± 0.76 0.08 143,271 0.045 2.86 ± 0.77 0.15 147,839 <0.001 2.85 ± 0.81 0.10 69,384 0.042 2.78 ± 0.64 0.09 26,363 0.132 –20.967 <0.001 3TC+EFV+TDF 2.65 ± 0.75 2.50 ± 0.69 –0.16 81,947 0.001 2.50 ± 0.70 –0.17 63,640 <0.001 2.56 ± 0.73 –0.13 28,246 0.041 2.61 ± 0.68 –0.11 19,112 0.406 –20.051 <0.001*D showed median changes in blood lipid profiles from baseline to different time points. †Z showed the Wilcoxon rank-sum test used to compare the median of lipid profiles at different time points to the baseline. ‡ADF showed the data after the difference were stationary (P <0.05), which means that the data after the difference no longer have a trend or serial correlation, but is a stable random process. 3TC+EFV+TDF: Lamivudine, efavirenz, and tenofovir disoproxil fumarate; AIDS: Acquired immunodeficiency syndrome; BIC/FTC/TAF: Bictegravir, emtricitabine, and tenofovir alafenamide; BMI: Body Mass Index; HDL-C: High-density lipoprotein cholesterol; HIV: Human immunodeficiency virus; IQR: Interquartile range; LDL-C: Low-density lipoprotein cholesterol; SD: Standard deviation; TG: Triglyceride; TC: Total cholesterol.
In the 3TC+EFV+TDF group, compared to the baseline, significant increases in TG and HDL-C levels were noted at specific weeks, but the differences between the baseline and 48 weeks in TG, TC, HDL-C, and LDL-C levels were not statistically significant, indicating stationarity median changes over time.
The median changes from baseline to 4 weeks, 12 weeks, 24 weeks, and 48 weeks in blood lipid profiles among naïve treated male adult HIV/AIDS patients based on two regimes are illustrated in Figure 1.
 Figure 1:
Figure 1: Lipid profile changes at different time points by BIC/FTC/TAF and 3TC+EFV+TDF in naïve treated adult HIV/AIDS male patients. 3TC+EFV+TDF: Lamivudine, efavirenz, and tenofovir disoproxil fumarate; BIC/FTC/TAF: Bictegravir, emtricitabine, and tenofovir alafenamide; HDL-C: High-density lipoprotein cholesterol; HIV/AIDS: Human immunodeficiency virus/acquired immunodeficiency syndrome; LDL-C: Low-density lipoprotein cholesterol; TC: Total cholesterol; TG: Triglyceride.
Comparison of changes in blood lipid at different time points among HIV/AIDS patients using BIC/FTC/TAF and 3TC+ EFV+TDF treatmentThe differences in average changes in the level of TG from weeks 4, 12, 24, and 48 to baseline between BIC/FTC/TAF and 3TC+EFV+TDF groups were not statistically significant (Z = 1,553,355, P = 0.959). The difference in average changes in the level of TC (Z = 1,552,672, P = 0.983), HDL-C (Z = 1,559,673, P = 0.875), and LDL-C (Z = 1,550,967, P = 0.897) between two groups was also not statistically significant.
Influencing factors of blood dyslipidemia (increased LDL-C) among HIV/AIDS patients receiving ART at 48 weeksThe median follow-up time for the 870 HIV/AIDS patients was 30.9 weeks, with 19 (2.2%) patients developing increased LDL-C (≥4.9 mmol/L), with 14 (2.7%) in BIC/FTC/TAF group and 5 (1.4%) in 3TC+EFV+TDF group, resulting in an overall incidence density of 0.07/100 person-weeks. The incidence density for the two regimes was 0.09/100 person-weeks and 0.04/100 person-weeks, respectively. However, there was no correlation with an increased LDL-C level in the BIC/FTC/TDF group compared with the 3TC+EFV+TDF group. The multivariate Cox proportional risk model analysis indicated that initiating ART with a baseline HIV-1 RNA ≥100,000 copies/mL, compared to <100,000 copies/mL, was significantly positively correlated with the incidence of increased LDL-C (hazard ratio [HR] = 1.26, 95% CI: 1.07–1.48) [supplementary Table 2, https://links.lww.com/CM9/C14].
DiscussionRelative factors contributing to dyslipidemia among the general population are categorized into primary and secondary factors.[12] These include a family history of disease, sex, age, a long-term high-fat diet, obesity, smoking, drinking, chronic disease, drug side effects, and among others. Such factors can disrupt lipoprotein metabolism, leading to increased levels of TG, TC, and LDL-C in plasma, and decreased levels of HDL-C.
In the context of HIV infection, chronic inflammation and immune activation lead to the release of numerous cytokines and other immunoreactive substances. These substances induce stress response in fat cells and cause inflammatory changes, potentially leading to steatosis. These alterations can impact the body’s blood lipid metabolism, resulting in various metabolic disorders such as hypertriglyceridemia and low HDL-C levels.[15]
Since LDL-C levels can independently predict the risk of arteriosclerotic cardiovascular disease (ASCVD) in individuals or populations, both domestic and international guidelines for the prevention and treatment of dyslipidemia emphasize the crucial role of LDL-C in the pathogenesis of ASCVD and recommend it as the primary target for intervention.[16] According to the recommendation for primary diagnosis and treatment of dyslipidemia,[12] the levels of TG (<1.7 mmol/L), TC (<5.2 mmol/L), and HDL-C (1.0–1.6 mmol/L) were appropriate at baseline in this study. However, the baseline LDL-C levels in the BIC/FTC/TAF group (2.72 ± 0.76 mmol/L) and in the 3TC+EFV+TDF group (2.65 ± 0.75 mmol/L) were slightly higher than the recommended level (<2.6 mmol/L). These findings are consistent with previous domestic researches in China, which reported that more than 50% of untreated HIV-infected individuals had dyslipidemia,[17] and about 20% of patients exhibited elevated LDL‑C levels after 2 years of ART treatment.[18]
HIV/AIDS patients, especially those on ART, are considered high-risk groups for dyslipidemia.[19] Lipid screening and intervention are crucial for controlling dyslipidemia to prevent the long-term risk of ASCVD.[20] The precise mechanism behind ART-related dyslipidemia is not fully understood but is thought to be related to alterations in liver synthesis function, inflammatory response, oxidative stress, drug effects, and potential genetic factors following ART.[21]
Regarding drug categories, NRTIs and NNRTI generally increase the levels of TC, LDL-C, HDL-C, and TG. Most PIs can increase the levels of TC, LDL-C, and TG, whereas a low dose of ritonavir is known to decrease HDL-C.[22,23] Fusion inhibitors minimally impact blood lipid levels. Clinical studies comparing various antiretroviral drugs have indicated that although EFV has a smaller effect on blood lipids than lopinavir/ritonavir (LPV/r), it can still increase the levels of LDL-C, TG, and HDL-C.[4,24] In this study, significant differences were observed in the changes of TC and LDL-C between the BIC/FTC/TAF and the 3TC+EFV+TDF groups before week 12, with no significant differences in lipid changes between the two groups after week 12. This aligns with the findings from a previous study on the effect of switching from 3TC+EFV+TDF to BIC/FTC/TAF on blood lipids.[25] However, the difference in the impact on blood lipid profiles between the two groups diminished over time, indicating the need for further long-term observation.
The introduction of new antiretroviral drugs with fewer adverse metabolic effects may lead to a reduction in ASCVD events among HIV-infected individuals. According to the current Chinese Guidelines for HIV Diagnosis and Treatment (2021), the rapid initiation of antiretroviral therapy in the early stages of HIV infection can reduce inflammation, preserve immune function, and potentially reduce the risk of atherosclerosis induced by HIV infection. Previous researches on the effects of BIC/FTC/TAF on blood lipids have primarily focused on comparative analysis with DTG/abacavir/lamivudine or DTG plus TDF, or plus TAF/FTC therapies. These studies have generally shown similar lipid outcomes over 48 weeks with BIC/FTC/TAF compared to those in patients receiving DTG-based therapies, both among treatment-naïve and treatment-experienced patients.[26,27] However, some trials have shown significant differences in median changes in TG levels and the TC to HDL-C ratio between BIC/FTC/TAF and DTG-based regimens.[28]
After 48 weeks of observation, a slight and transient increase in blood lipids was noted in the first 24 weeks, with TG, TC, and LDL-C levels remaining relatively stable at 48 weeks compared to baseline, except for an increase in HDL-C. Although changes in lipid profiles were observed at certain time points, the clinical differences were not significant due to the lack of substantial median value changes. This study found that the comparison between the 3TC+EFV+TDF regimen and the BIC/FTC/TAF regimen showed a stable effect on the blood lipids of newly treated patients, indicating that the changes in lipid panel parameters at different time points within 48 weeks did not show an upward trend. Given the predictive effect of HDL-C on the risk of ASCVD, LDL-C was selected as an evaluation index in accordance with the Guidelines for diagnosis and treatment of dyslipidemia.[12] Multivariate analysis revealed that a patient’s HIV viral load at baseline was a significant factor after adjusting for age, BMI, baseline CD4, and starting regimen. Contrary to previous findings that suggested age and BMI at the initiating ART were risk factors for dyslipidemia but plasma HIV viral load was not,[29,30] this study found that a baseline HIV viral load ≥105 copies/mL was associated with an increase in LDL-C.
In the early stages of HIV infection, the high level of viral replication not treated with antiretroviral drugs causes chronic inflammation and immune activation. The release of numerous cytokines and other immunoreactive substances induces the stress response in fat cells, leading to inflammatory changes that may cause steatosis, affect the body’s lipid metabolism, and induce metabolic disorders such as high TC and low HDL-C levels.[31] Dyslipidemia is primarily associated with HIV infection and the use of antiretroviral drugs. Thus, promptly initiating antiretroviral therapy to effectively suppress viral replication is beneficial for maintaining normal blood lipid levels in HIV patients. It was crucial for patients receiving BIC/FTC/TAF or 3TC+EFV+TDF to conduct periodic screening of blood lipid panels and other CV risk factors to assess the risk of dyslipidemia.[32] Furthermore, lipid-lowering therapy, such as the use of pitavastatin, has been shown to significantly reduce the incidence of major adverse CV events in HIV-positive individuals on ART.[33]
There are some limitations in this study. The data related to factors that could influence dyslipidemia, such as diet, exercise intensity, family history, and use of lipid-lowering drugs, were not collected, which could affect the extrapolation and applicability of the findings. The primary endpoint of increased LDL-C levels may have implications for the interpretation of the results. Additionally, the analysis was based solely on four traditional lipid tests: TG, TC, LDL-C, and HDL-C, which may not fully capture the overall lipid metabolic status. Moreover, some subjects were lost to follow-up, potentially leading to an underestimation or overestimation of the prevalence of dyslipidemia. The main reasons for the loss of follow-up of patients or the absence of blood lipid results were either the failure to conduct timely blood lipid tests after viral load reduction and stabilization or patients transferring to other hospitals.
In summary, BIC/FTC/TAF, as a new INSTI-based compound in a single tablet with FTC/TAF, demonstrated elevated blood lipid levels after 12 weeks and 24 weeks of administration. However, the difference in the impact on blood lipid changes between BIC/FTC/TAF and 3TC+EFV+TDF was gradually reduced after 12 weeks. High viral load in newly treated HIV patients at baseline was associated with elevated LDL-C after treatment, but these levels did not significantly differ from baseline levels after 48 weeks. Overall, maintaining normal blood lipid levels suggests that the use of single tablet regimens can promote long-term adherence to treatment, meeting the clinical demand for ART in HIV-infected individuals.
FundingThis work was supported by the Gilead Sciences and the Capital Health Research and Development of Special Fund (No. 2022-1G-3015).
Conflicts of interestNone.
References 1. Zhao Y, Gan XM, Zhao DC, Dou ZH, Wu YS, Lian YT, et al. The progress of antiretroviral treatment of HIV/AIDS in China and the consideration of promoting high-quality development (in Chinese). Chin J AIDS STD 2023;29:619–622. doi: 10.13419/j.cnki.aids.2023.06.01. 2. Han MJ. Analysis of epidemic situation of AIDS in China and prospect of prevention and treatment (in Chinese). Chin J AIDS STD 2023;29:247–250. doi: 10.13419/j.cnki.aids.2023.03.01. 3. HIV/AIDS Hepatitis C Group, Chinese Association of Infectious Diseases Branch, Chinese Center for Disease Control and Prevention. China AIDS diagnosis and treatment guidelines (2021 edition). Chin J AIDS STD 2021;27:1182–1201. 4. Lagathu C, Béréziat V, Gorwood J, Fellahi S, Bastard JP, Vigouroux C, et al. Metabolic complications affecting adipose tissue, lipid and glucose metabolism associated with HIV antiretroviral treatment. Expert Opin Drug Saf 2019;18:829–840. doi: 10.1080/14740338.2019.1644317. 5. Chang HH. Weight gain and metabolic syndrome in human immunodeficiency virus patients. Infect Chemother 2022;54:220–235. doi: 10.3947/ic.2022.0061. 6. Sapuła M, Suchacz M, Załęski A, Wiercińska-Drapało A. Impact of combined antiretroviral therapy on metabolic syndrome components in adult people living with HIV: A literature review. Viruses 2022;14:122. doi: 10.3390/v14010122. 7. Islam FM, Wu J, Jansson J, Wilson DP. Relative risk of cardiovascular disease among people living with HIV: A systematic review and meta-analysis. HIV Med 2012;13:453–468. doi: 10.1111/j.1468-1293.2012.00996.x. 8. Yazie TS. Dyslipidemia and associated factors in tenofovir disoproxil fumarate-based regimen among human immunodeficiency virus-infected Ethiopian patients: A hospital-based observational prospective cohort study. Drug Healthc Patient Saf 2020;12:245–255. doi: 10.2147/DHPS.S283402. 9. Zhang J
Comments (0)