Demographic, clinical, and operative characteristics as well as admission, hospital, and surgeon characteristics prior to matching are summarized in Table 1. From January 1, 2017, to December 31, 2020, a total of 233,945 patients were identified in the dataset as having undergone Ur-Em cholecystectomy: open (n = 2687), robotic (n = 10,019), or laparoscopic cholecystectomy (n = 221,239). Patients were evenly distributed over the age groups of 18–44 years (35%), 45–64 years (33%), and ≥ 65 years (32%). Patients were similar in terms of body mass index (BMI), race, ethnicity, primary diagnosis, and comorbidity burden.
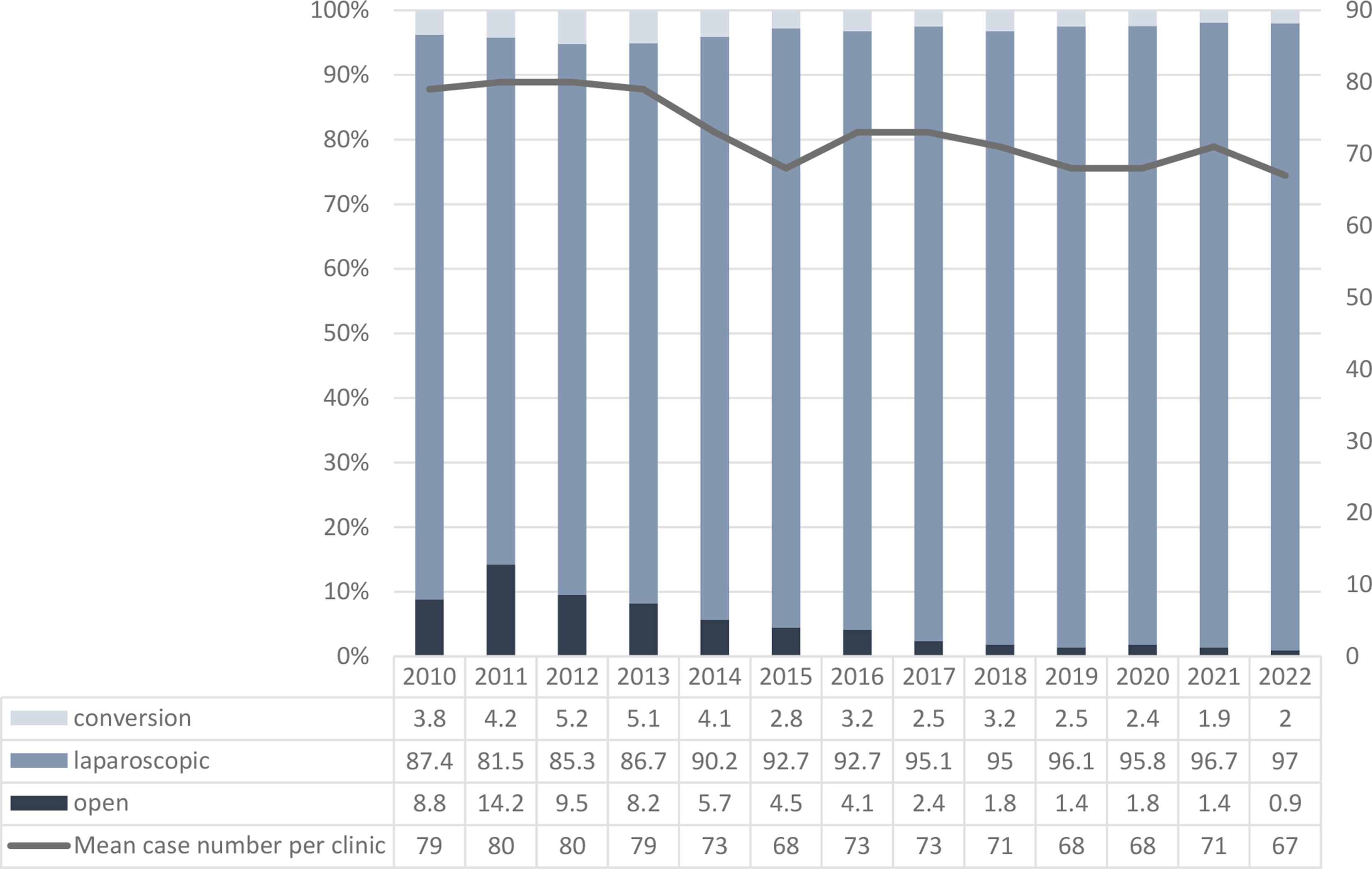
Table 1 Comparative patient demographics, medical presentation, hospital, and surgeon characteristics prior to propensity score matching (PSM)aThe frequency of robotic cholecystectomy increased each year from 2017 (2.6%) through 2020 (7.7%). Both the incidence of open cholecystectomies and laparoscopic cholecystectomies decreased over the same period (1.3–1% and 96–91.3%, respectively). Sixty-five percent (n = 152,139) of cholecystectomies were performed for cholecystitis across all surgical modalities (open, robotic, laparoscopic); the next most common indication for cholecystectomy was choledocholithiasis (18%), followed by biliary pancreatitis (9%). RAC was more commonly performed in urban medical centers (92%) compared to rural medical centers (8%). Hospital size did not impact likelihood of the robotic approach. RACs were least likely to be performed by low volume surgeons (21%).
Fluorescent-guided imaging was performed more frequently in RAC (44.2%) compared to LC (1.4%). Intraoperative cholangiography more commonly was incorporated in LC (9.1%) versus RAC (4.8%). The majority of cases had neither intraoperative cholangiogram nor fluorescent imaging.
Propensity score analysis
Propensity score analyses was performed comparing RAC and LC (Table 2), RAC and OC (Table 3), and LC to OC (Table 4). For the RAC and LC comparison, there were 9996 matched patients, and overall there were no significant differences between the groups for intraoperative, postoperative complications, or 30-day postoperative outcomes (Table 2). There was a statistically significant decreased rate of conversions in RAC compared to LC (1.9% vs. 3.2%, p < 0.001). Mean and median (IQR) operating room times were significantly longer for RAC (128.4 min; 120 (91,150) compared to LC (110.7 min; 96 (75,128) (p < 0.001). Median hospital length of stay was identical.
Table 2 Robotic-assisted and laparoscopic cholecystectomy outcomes and 30-day post-surgery following post-propensity score matching (PSM)Table 3 Robotic-assisted and open cholecystectomy outcomes and 30-day post-surgery following post-propensity score matching (PSM)Table 4 Laparoscopic and open cholecystectomy outcomes and 30-day post-surgery following post-propensity score matching (PSM)There were 2054 matched patients in the RAC compared to OS analysis (Table 3) and 2637 matched patients in the LC compared to OC analysis (Table 4). For both analyses, open cholecystectomy was significantly associated with higher rates of overall postoperative complications, hospital LOS, 30-day mortality, 30-day readmissions, and blood transfusion (Tables 3 and 4). Index hospitalization complications were all significantly greater in the OC cohort except for: bile duct injury, gastrointestinal hemorrhage, and wound hematoma/seroma. Analysis of 30-day outcomes demonstrated significantly lower rates for the both cohorts for complications including: sepsis, intestinal obstruction, all wound infections/complications, pulmonary complications, cardiovascular complications, and drainage of intraperitoneal abscess.
Differences were seen in operating room time which were significantly longer for robotic cholecystectomy [RAC 150 min (115, 195) vs. OC min 120 (93, 180) p < 0.001)] and shorter for LC [120 min (90,150) vs. OS 150 min (120,201) p < 0.001)].
Subgroup analyses for cholangiogram and Class III obesity
Subgroup analysis of 3267 propensity-matched patients RAC performed with near-infrared (fluorescent) imaging and RAC performed without either fluorescent imaging or IOC showed no significant difference in intraoperative complications, immediate postoperative complications, median operating room time, and 30-day postoperative outcomes including bile duct injury, retained gallstone, surgical site infection, or 30-day readmission (Additional file 9: eTable 4).
A total of 1133 matched pairs were analyzed for outcomes in RAC or LC in patients with Class 3 obesity (Additional file 10: eTable 5). RAC was associated with a significant lower rate of conversion to OC (2.6%) compared to LC (4.4%, p = 0.024). There were no significant differences in intraoperative complications, immediate postoperative complications, postoperative to 30-day outcomes/complications, and readmission between the two operative approaches. Operative time was significantly longer in RAC (120 min (101,172) compared to LC (110 min (90,150) (p < 0.001).
Exploratory analysis for risks for key outcomes (bile duct injury, conversions, complications)
Multivariate regression analysis for significant risk factors associated with bile duct injury was open cholecystectomy (2.15 (1.44–3.21), p < 0.001), male sex (1.22 (1.06–1.41), p < 0.01), and primary diagnosis of bacteremia/sepsis (1.75 (1.37–2.24), p < 0.00) or CBD stones and disease (3.94 (3.38–4.60), p < 0.001) (Additional file 11: eTable 6). Conversely, surgery performed in later admission years (2020: 0.50 (0.41–0.63), p < 0.001) and outpatient procedures (0.47 (0.24–0.92), p < 0.03) were associated with a significantly lower risk of bile duct injury.
Significant lower risks for conversion to OC were seen in patients that had RAC (0.54 (0.47–0.63), p < 0.001), a primary diagnosis of biliary pancreatitis (0.42 (0.38–0.47), p < 0.001) or common bile duct stone-related disease (0.87 (0.82–0.92), p < 0.001), outpatient procedures (outpatient 0.03 (0.01–0.07), p < 0.001 and outpatient observation < 24 h. 0.02 (0.01–0.04), p < 0.001), and surgeons with a higher volume of cholecystectomy in the year prior to the index surgery [0.77 (0.73–0.82), p < 0.001) (Additional file 12: eTable 7).
Significant risk factors for increased postoperative overall complications (Additional file 13: eTable 8) were open cholecystectomy (2.41 (2.19–2.65), p < 0.001), male patients (1.20 (1.16–1.24), p < 0.001), higher BMIs, any diagnosis other than cholecystitis without common bile duct stone with the greatest risk a diagnosis of bacteremia/sepsis (6.44 (6.20–6.69), p < 0.001), CCI score > 0, and outpatient observation < 24 h. (1.95 (1.86–2.06), p < 0.001).
Covariate balance
The covariate balance tests for RAC versus LC, RAC versus OC, LC versus OC as well as RAC with or without fluorescent imaging and RAC versus lap in patients with class 3 obesity indicated that the absolute standardized mean differences were < 0.1 for all covariates indicating a satisfactory covariate balance (see Additional file 1: eFigure 1–Additional file 5: eFigure 5).





Comments (0)