This study employed a hospital-based retrospective cross-sectional design to investigate the magnitude, outcome, and predictors of mortality in patients undergoing surgery for perforated peptic ulcer disease (PUD) at two public hospitals in Jigjiga, Ethiopia: Karamara Hospital and Sheikh Hassan Yabare Referral Hospital (SHYR-hospital). The study was conducted over three years, from April 1st, 2018, to July 30th, 2021.
Study setting
The study was conducted at Karamara Hospital and Sheikh Hassan Yabare Referral Hospital, both public hospitals located in Jigjiga town, the capital of the Somali Regional State of Ethiopia. These hospitals serve a large population in the region and provide surgical services for various conditions, including perforated PUD.
Study population
The study population consisted of all patients who underwent surgery for perforated PUD at Karamara Hospital and SHYR-hospital during the study period.
Inclusion criteria
All patients who underwent surgical repair for perforated PUD at the study hospitals between April 1st, 2018, and July 30th, 2021.
Complete medical records with sufficient information for data extraction.
Exclusion criteria
Patients with incomplete medical records or missing key variables.
Patients whose perforation was due to causes other than peptic ulcer disease (e.g., trauma).
Sample size and sampling technique
The sample size was determined to be 130 patients. Medical record numbers were retrieved from the operating room registration logbooks of the two hospitals. A consecutive sampling technique was used to select the medical records from the archives, ensuring that all eligible patients within the study period were included in the sample. Specifically, 48 records were retrieved from Karamara Hospital and 79 from SHYR-hospital. Three patients were excluded from the study because of incomplete data and not meeting inclusion criteria, making the response rate 97.7%.
Data collection
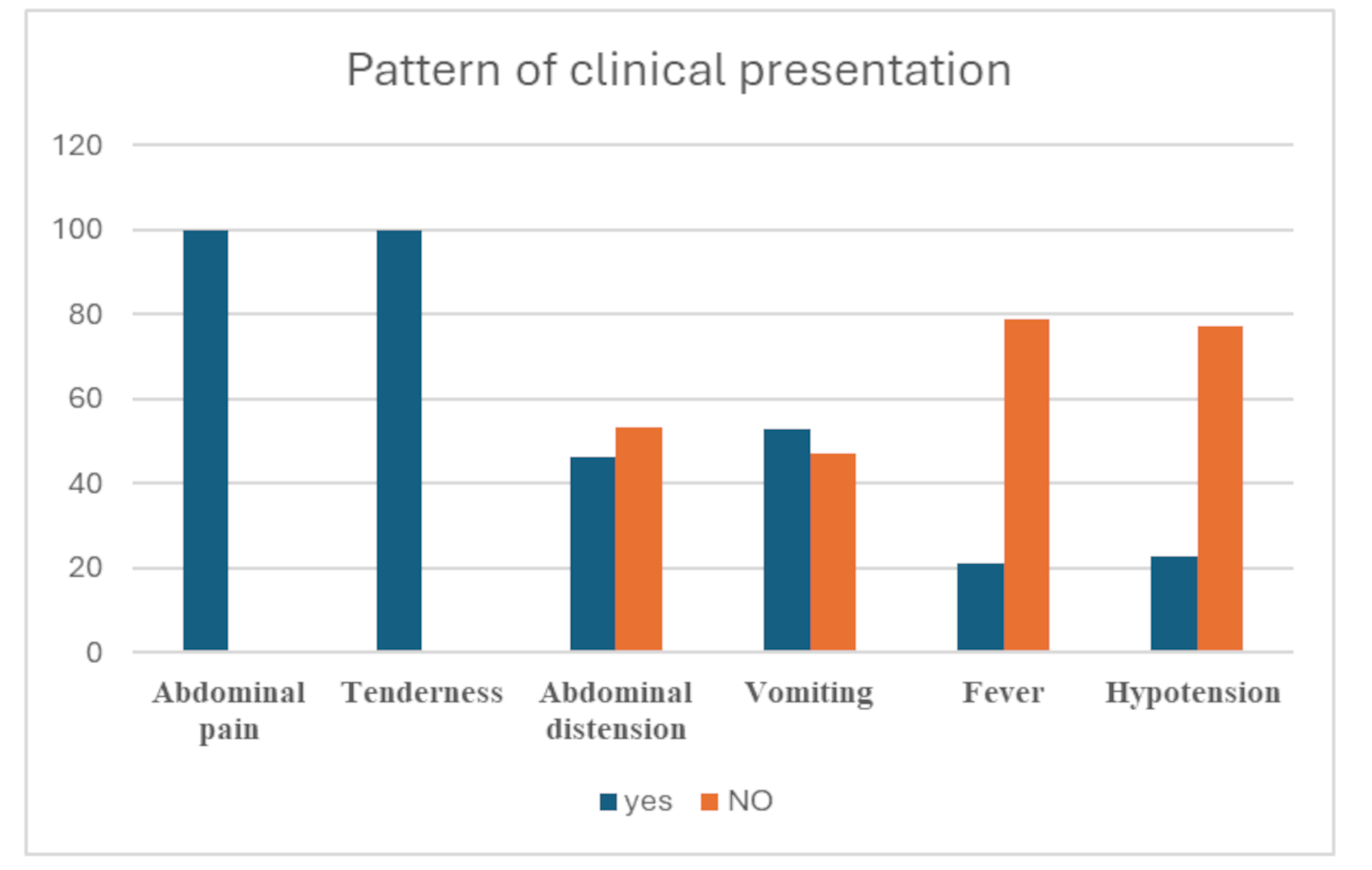
Data were extracted from patients’ medical records using a pre-tested, structured data extraction form. The data extraction form was designed based on a review of relevant literature and included the following variables: socio-demographic characteristics (age, sex, and residence); lifestyle factors (smoking status, khat chewing, alcohol consumption, coffee drinking, and history of fasting); clinical presentation (duration of symptoms, presenting symptoms such as abdominal pain, nausea, and vomiting, pre-operative systolic blood pressure, previous history of dyspepsia, and previous treatment for peptic ulcer disease); pre-morbid conditions (presence of hypertension, diabetes mellitus, and chronic kidney disease); laboratory findings (white blood cell count and creatinine levels); intra-operative findings (location of perforation, size of perforation, amount of peritoneal contamination, surgical procedure performed, and use of drainage); post-operative complications (surgical site infection, pneumonia, acute kidney injury, patch failure, and fascial dehiscence); mortality (in-hospital mortality status and cause of death); and time-related variables (duration of symptoms before presentation, time of diagnosis, and duration before surgery).
The data extraction process was conducted by trained data collectors who were familiar with medical record documentation. A pilot study was conducted on a small sample of records to ensure the clarity and consistency of the data extraction form.
Data analysis
Data were entered and analyzed using SPSS version 25.0 (Statistical Package for the Social Sciences). Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize the data.
Bivariate analysis was performed using chi-square tests or Fisher’s exact tests (where appropriate) to assess the association between independent variables (e.g., age, comorbidities, pre-operative hypotension, delayed presentation) and the outcome variables (post-operative complications and mortality). Variables with a p-value of < 0.05 in the bivariate analysis were considered for inclusion in the multivariate logistic regression model.
Multivariate logistic regression analysis was used to identify independent predictors of postoperative complications and mortality. Adjusted odds ratios (AOR) and 95% confidence intervals (CI) were calculated to quantify the strength of the association. A p-value of < 0.05 was considered statistically significant in the multivariate analysis.
Diagnostic approach and operative techniques
All patients presenting with clinical signs of generalized peritonitis, including severe abdominal pain, tenderness, guarding, and signs of systemic infection, underwent emergency surgical intervention. Diagnosis of perforated peptic ulcer was primarily based on clinical evaluation and confirmed by abdominal radiographs (erect chest and abdominal X-rays) demonstrating free subdiaphragmatic air. In cases where the diagnosis remained uncertain, abdominal ultrasonography was utilized to identify free intraperitoneal air or fluid. Surgical procedures performed included primary closure of the perforation with or without an omental (Graham’s) patch reinforcement, accompanied by thorough peritoneal lavage with warm saline to reduce the risk of postoperative infection.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of the respective hospitals. Permission to access medical records was also obtained from the hospital administration. Patient confidentiality was maintained throughout the study by anonymizing the data and storing it securely. Informed consent was waived by the IRB, as the study involved retrospective data collection from medical records, and no direct contact with patients was required.





Comments (0)