
Remember me




Our study demonstrates that oSSRF and cTSSRF significantly reduces pain and improves respiratory function in patients with multiple rib fractures, consistent with previous reports [6,7,8]. The median numeric rating scale (NRS) pain score reduction from 7 to 3 postoperatively aligns with findings by Pieracci et al., who noted superior pain control at 2 weeks compared to non-operative management [9]. This reinforces SSRF’s role in mitigating ventilator-associated complications by preserving cough efficacy—none of our patients required reintubation, supporting its physiological benefits in maintaining airway clearance.
Conventional approaches to oSSRF include the pectoral muscle preservation technique, which utilizes the smallest possible incision and muscle-sparing principle [10]. Rib fracture fixation is conducted in accordance with the muscle-sparing principle, in which the muscle gap is opened without cutting the chest muscles. Combinations of posterior and lateral minimized approaches allow surgical fixation of 6–9 and 7–11 ribs through 5 and 10 cm incisions, respectively [11]. This procedure ensures not only the integrity of the chest wall muscles, but also a reduction in the impairment of respiratory muscle function. Zhang et al. [4] reported that based on the ZZF zone of the chest wall anatomical structure and the application of the principle of muscle-sparing, rib fracture internal fixation surgery was completed through a minimally invasive small incision and achieved good clinical results. Muscle-sparing minimally invasive thoracotomy rib fixation is safe and improves pulmonary function in G60 trauma patients diagnosed with severe rib fractures [12].
However, for rib fractures in the high posterior rib region, limitations such as the large number of muscle groups in the region, scapular coverage, and thick muscle tissue make it difficult to expose the surgical field. During surgery, some muscles may be severed, soft tissues around the shoulder blade may be dissociated, and the scapula may be stretched, resulting in secondary injuries. Traditional approaches often require scapular retraction or partial muscle division, increasing the risk of chronic shoulder dysfunction. Endocortical plating eliminates scapular impingement—a common complaint after conventional SSRF, affecting 15–20% of patients [13].
To address the aforementioned limitations, an alternative approach was implemented using a lateral anterior chest wall incision to facilitate the completion of high posterior rib fracture fixation via the thoracoscopic technique. The theoretical advantages of cTSSRF are as follows: First, the incision is small with a wide field of view and direct access. Through a small incision of 3–5 cm in the anterior chest wall or axilla, almost all posterior rib areas can be clearly explored using the thoracoscopic technique. Rib fractures can be observed by incising only the parietal pleura, which can be achieved without multiple incisions. The incision is in the lateral chest wall and axilla, which is more hidden, especially for some people who have special needs for the incision site, such as patients with posterior rib fractures in the tattooed area requiring surgical treatment. Second, rib fracture fixation surgery through the endo cortex can eliminate discomfort due to plate dislodgement, palpable plates, and contact with the scapula during shoulder movement. In Felix Peuker’s study, 30.1% (n = 25) of patients experienced varying degrees of implant irritation, resulting in the removal of 4.8% (n = 4) of the patients [14]. (3) Minimize injury to the overlying muscles, nerves, lungs, and heart. (4) Identification and repair of associated intrathoracic injuries concurrently. We successfully applied cTSSRF to stabilize most posterior rib fractures. This approach required only 3–5 cm incisions on the anterolateral chest wall, while preserving the dorsal muscles and nerves intact, thereby maximizing the functional integrity of back muscles and sensory innervation.
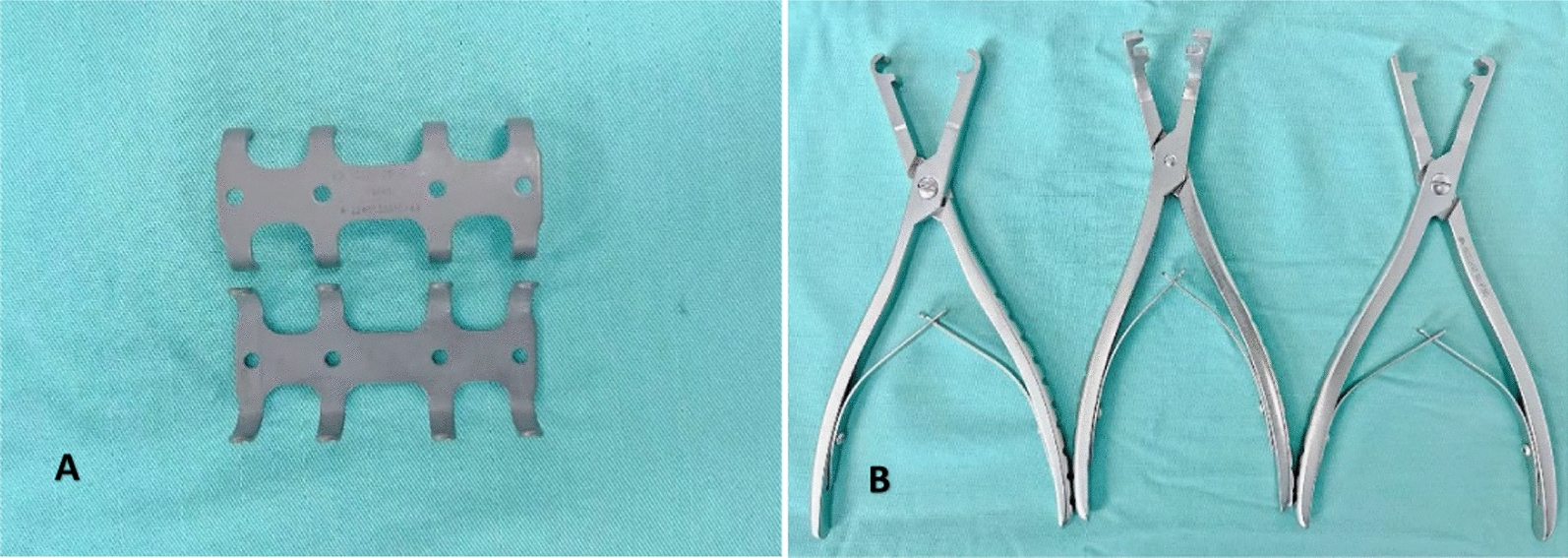
Simultaneously, cTSSRF has several drawbacks. A review analysis of complications from Choi [15] on 2404 patients with rib fractures who underwent rib stabilization surgery showed a 4% complication rate with implants. Mechanical failure (2.62%) (including fracture displacement and screw detachment) was the most common implant complication. The data from this study indicated that the implant displacement rate of 6.33% (5/79) and the fracture malalignment rate of 25.32% (20/79) were higher under cTSSRF than under mechanical failure of external cortical internal fixation of rib fracture surgery from Choi’s review analysis (2.62%).The cTSSRF group demonstrated a significantly higher incidence of fracture malalignment compared to conventional SSRF (21.52% [20/79] vs. 2.46% [3/122]; χ2 = 24.72, P < 0.001)(Fig. 5A, Table 4). The elevated complication rates associated with cTSSRF may be attributed to the following technical and anatomical challenges. The first reason is mismatch between implant design and rib anatomy. The ribs have the characteristics of three-dimensional structure of surface curvature, lateral curvature, and torsion angle [16], whereas the thoracoscopic transthoracic memory alloy rib coaptation board has a straight plate design, which cannot fully match the anatomical morphology of the ribs. In addition, the thoracoscopic transthoracic memory alloy rib coaptation board cannot be effectively stabilized because of the small gripping area caused by only one pair of arms embracing each end (Fig. 7A). An additional contributing factor is suboptimal fracture reduction under thoracoscopy. Although the thoracoscopic visual field was well exposed, intraoperative application of surgical instruments for implant placement could obstruct the view of the fracture, making it difficult to ensure proper reduction of the rib fracture. Because a moderate extra-pulsive force is required to reset fractures, an inadequate force strength often results in the angular deformation of the fractured ends. Unlike open techniques, thoracoscopy limits tactile feedback, making it harder to judge reduction adequacy.
Fig. 7
A The thoracoscopic transthoracic memory alloy rib coaptation board could not completely encircle the upper and lower edges of the ribs, and one side of the arm was stuck in the intercostal nerve groove. B The image illustrates the inevitable large parietal pleural damage resulting from the cTSSRF for the fixation of the 3rd-7th posterior rib fractures
Part of the parietal pleura should be removed during surgery to expose and fix rib fractures. Especially in multiple rib fractures, damaged parietal pleura is unavoidable and extensive (Fig. 7B), often leading to postoperative encapsulated pleural effusions despite complete removal of the pleural effusions intraoperatively by thoracoscopic techniques and accurate placement of thoracic drainage tubes. In the current study, the incidence of postoperative encapsulated pleural effusion—defined as a maximum anteroposterior fluid thickness > 20 mm surrounding the internal fixation device on axial CT scans—was 46.7% (14/30 cases) during the 7–14 day postoperative period. During the initial phase of our surgical practice, ultrasound-guided closed thoracostomy was attempted in selected cases. However, minimal drainage output was observed, likely attributable to severe localized parietal pleural injury with subsequent encapsulation and adhesions. Despite the absence of systemic febrile reactions, dyspnea, or clinical signs of pleural space infection in these patients, no additional invasive interventions were implemented in subsequent cases. The management protocol emphasized proactive encouragement of pulmonary rehabilitation exercises and early ambulation to facilitate pleural fluid resorption. Even in the absence of overt clinical manifestations, peri-implant pleural effusion surrounding the rib fixation plate remains a clinically significant risk factor, potentially precipitating severe complications including but not limited to empyema, implant-associated infection, osteomyelitis, and eventual requirement for implant removal due to refractory infection or biomechanical failure. Although uncommon, hardware infection after SSRF carries considerable morbidity [17].
Notably, the development of dense postoperative pleural adhesions secondary to extensive parietal pleural injury presents a substantial intraoperative challenge during re-thoracotomy for implant explantation, as exemplified in Fig. 5B. Vincenzo Verzeletti et al.’s study about in redo VATS for pulmonary ipsilateral malignancy revealed that reoperation cases exhibited significantly longer surgical duration (P < 0.01), higher incidence of pleural adhesions, increased postoperative drainage, and prolonged hospital stay compared to primary procedures[18]. The application of completely thoracoscopic surgical stabilization for posterior rib fractures risks injury to the sympathetic chain ventral to the ribs, with an estimated 1% incidence of iatrogenic nerve injury in thoracic surgery, primarily from direct surgical trauma [19]. Given the heightened risk of intercostal neurovascular injury associated with cTSSRF, it is imperative that the operator possesses a more precise understanding of the anatomy of the rib cage and has extensive experience in the surgical fixation of rib fractures, as well as in thoracoscopic techniques.
This study also has some limitations. Our hybrid approach (combined open/thoracoscopic fixation) introduces confounding variables. Due to study limitations (retrospective design, small sample size, and multiple rib fracture sites), only 5 patients received purely thoracoscopic fixation for posterior rib fractures, while 25 patients underwent both surgical techniques to address fractures in the lateral/anterior and posterior ribs. Therefore, the postoperative outcomes in this study were actually a combined effect of traditional surgery and fully thoracoscopic rib fixation. The available evidence does not permit definitive conclusions regarding the comparative efficacy of these surgical approaches. While cTSSRF appears to offer some potential benefits relative to conventional procedures, it also carries notable drawbacks.
Furthermore, due to the pronounced curvature of the posterior ribs, a 21.52% fracture malalignment rate was observed following fully thoracoscopic rib fracture internal fixation. This is consistent with the findings of the CWIS-published multicenter retrospective study, which reported a 3% (38 of 1,224) hardware failure (HF) rate after SSRF, primarily due to screw migration (n = 17, 44.7%) and plate fracture (n = 18, 47.4%) in the posterolateral region [20]. Theoretically, these plates are more suitable for the anterior ribs, which have a smaller curvature. In this study, we did not apply cTSSRF for anterior rib fractures. For oSSRF addressing lateral and anterior fractures, small incisions with neuromuscular protection enabled effective fixation while minimizing operative time and surgical trauma [4] and the operative time for conventional SSRF was 82 ± 40.6 min, which was longer than that of cTSSRF in this study (109.9 ± 30.2 min). The cTSSRF in these regions would limit intrathoracic workspace, reducing thoracoscopic advantages and increasing surgical complexity. Thus, completely thoracoscopic fixation was avoided for smaller-curvature ribs due to unfavorable risk–benefit balance.
Future research directions should focus on expanding the sample size, collaborating with multiple centers, optimizing the materials for internal fixation(including patient-specific 3D-printed plates) and increasing the length of follow-up to improve the accuracy of the clinical effect of cTSSRF. We propose for standardized fracture-specific surgical protocols: open fixation for anterior/lateral fractures (simpler exposure, shorter operative time, less trauma) and thoracoscopy for posterior fractures (avoids scapular dissection, improves access). This strategy could enhance precision, reduce invasiveness in rib fracture management.
Comments (0)