Study design
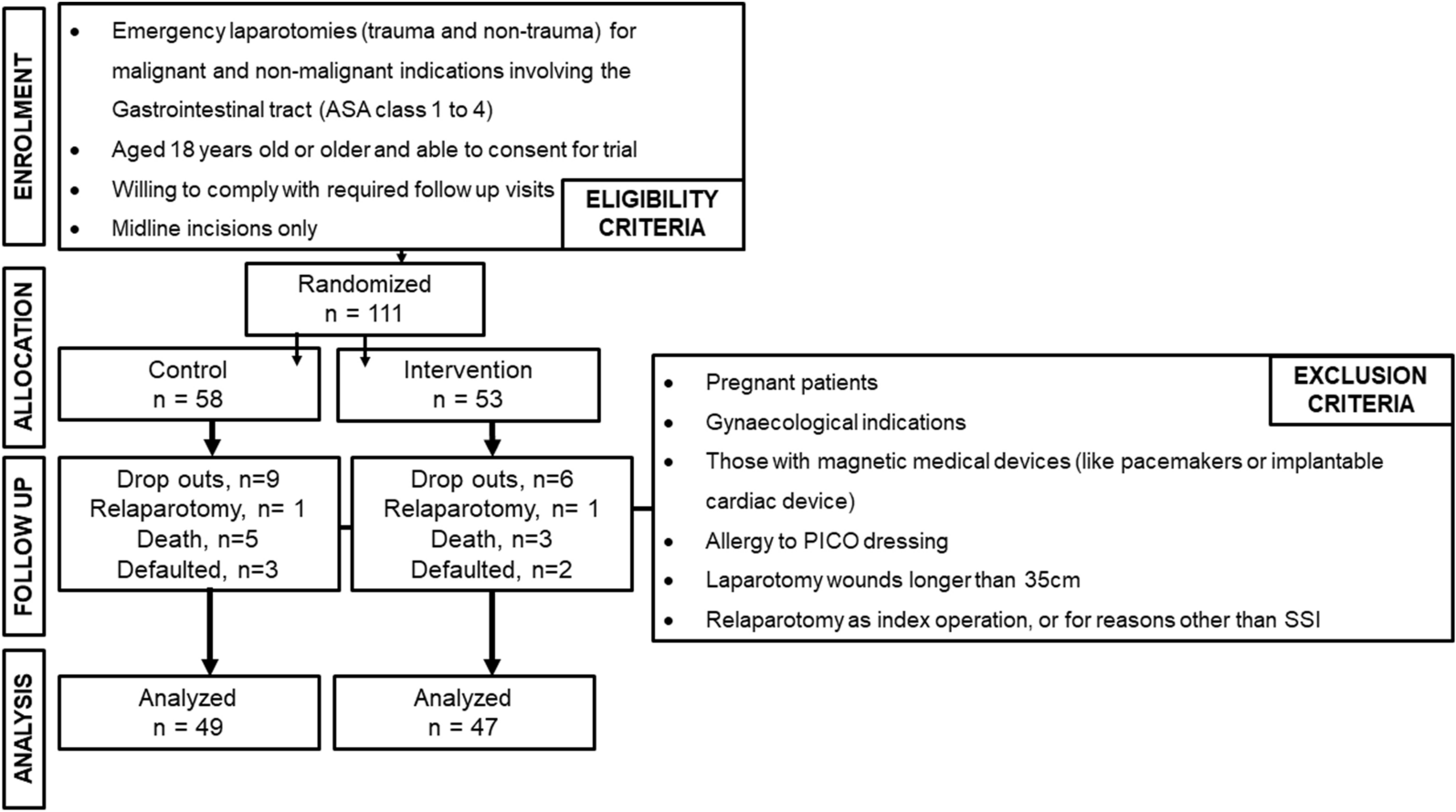
This was a double blinded randomized controlled trial conducted in University Malaya Medical Centre (UMMC), a tertiary teaching hospital in Kuala Lumpur, Malaysia, between October 2020 and February 2022. The inclusion and exclusion criteria are shown below.
Inclusion
Emergency laparotomies (trauma and non-trauma) for malignant and non-malignant indications involving the gastrointestinal tract
ASA class 1 to 4
Midline incisions
Aged 18 years old or older and able to consent for trial
Willing to comply with required follow up visits
Exclusion
Pregnant patients
Gynaecological indications
Those with magnetic medical devices (like pacemakers or implantable cardiac device)
Allergy to PICO dressing
Laparotomy wounds longer than 35 cm
Relaparotomy as index operation, or for reasons other than SSI
Emergency laparotomy was defined as surgery within 8 h of presentation for a life-threatening general surgical condition in which access to the abdominal cavity is through a midline incision [16].
Ethical approval from the institutional Medical Research Ethics Committee (MREC ID NO: 202057-8603) was obtained before date of commencement and the study was registered with the National Medical Research Registry (NMRR) with ID No. NMRR-20-1975-55222. Insurance coverage was also obtained for this study [2020-HB-L0002099-LNC]. The clinical use of the NPWT system was approved by the Biomedical Engineering Department of UMMC. Written consent was obtained from all patients enrolled in this study.
Study intervention
The PICO◊ system utilizes a single-use, portable, battery-operated pump that delivers NPWT at a pre-set pressure of − 80 mmHg. Weighing 70 g, it lasts for 7 days of continual use. Controlled by a single button, it incorporates leak detection and low-battery indicators. The dressing is made up of four layers with the capacity to absorb 200 mL of exudate, and removes wound exudate predominantly through evaporative loss [17].
Study participantsRandomization
Patients were randomized into two arms namely the PICO◊ dressing (intervention arm) or the conventional dressing (control arm) with a ratio of 1:1. Patients were randomized into blocks of eight utilizing the codes generated via the website-based randomizing tool [18]. Randomization was performed just before skin closure.
Standardization
All teams under the UMMC General Surgery Division participated in this trial. All patients who consented for this trial were provided with a patient information sheet. In all cases, intravenous antibiotics were given either as prophylaxis or for therapeutic intent, skin was prepared using povidone iodine, a wound protector was utilized, closure of fascial layer was performed with continuous loop nylon 1/0 (Ethicon, Inc., Somerville, NJ) and skin was closed with either staplers or non-absorbable or absorbable sutures.
Patients in the intervention arm had the PICO◊ 7 system (30 × 10 cm or 40 × 10 cm) applied onto their laparotomy wounds in the operation theatre immediately after skin closure. The system would be turned on as soon as it was assembled so that NPWT would be delivered promptly. The device would then be secured next to the dressing in order to prevent the patient from seeing the device.
The patients in the control arm would have the conventional post operative occlusive ‘island’ dressing applied onto their laparotomy wounds along with a non-functioning ‘dummy’ PICO◊ device plastered next to the conventional dressing. In this way, the patient was blinded to the intervention arm they were in. The surgeon and the managing team however were not blinded to the intervention the patient received.
Demographic and surgical characteristics data was collected. Wound inspection was carried out on days 3, 7, 14 and 30 post-operatively. The wound assessor, an enterostomal and wound therapy nurse was blinded to the wound therapy used. Wounds were evaluated for SSI, seroma and dehiscence.
If a patient in the intervention arm developed SSI, they ceased to be on the PICO◊ dressing and were managed according to the standard of care. If there was evidence of seroma or dehiscence in the intervention arm after day 7, another cycle of PICO◊ was reapplied and wound was reinspected on day 14. In the control arm, SSI, seroma and dehiscence in the control arm were managed according to the standard of care. On day 14 onwards, wounds were inspected again. If wounds were healed, they were left exposed. If SSI, seroma, and/or dehiscence developed in either arm, they were treated according to the standard of care. Patients’ wound experience was explored during a clinic encounter between 1 and 6 months post operatively using the Wound Experience Questionnaire by the Bluebelle Study Group [19].
Study parameters and outcome measures
Demographic data such as age, gender and smoking status, BMI, comorbidities, ASA physical status classification, albumin levels and exposure to steroids, chemotherapy and radiotherapy were obtained from the electronic medical records. Body mass index (BMI) was grouped according to the WHO classification and comorbidities were identified. Patients were also grouped according to their American Society of Anaesthesiologists (ASA) physical status, albumin levels (< 28, 28–35, > 35 g/L) and if they had received steroids, chemotherapy or radiotherapy.
Surgical characteristics like day (weekday or weekend), timing [day (before 8 pm) or night (after 8 pm)], classification of wounds (clean, clean contaminated, contaminated and dirty) as per CDC and surgeon status (General Surgical Trainees and Consultant) were tabulated. Diagnoses were classified into ischemia, trauma, haemorrhage, obstruction or perforation from a benign cause and obstruction or perforation from a malignant cause. Duration of surgery (in minutes), wound length (in centimetres), indication of antibiotics (prophylactic or therapeutic) and number of days on antibiotics were also noted.
Holistic assessment of outcomes is necessary to determine the value of an intervention. Our primary outcome was the rate of SSI within 30 days after emergency laparotomy in patients receiving the PICO◊ system dressing versus those who received the standard occlusive post-operative dressing. SSI was defined according to the CDC guidelines [7]. Wounds would be evaluated four times during the first 30 days post-operatively namely on day 3, day 7, day 14 and day 30 post operatively. Secondary outcomes like seroma and dehiscence rates as well as length of stay in days, number of days on dressing and patients’ wound experience were also observed. Questions related to wound experience are listed in Table 4. Patients were given the option of four possible answers: “Not at all”, “A little”, “Quite a bit” or “A lot”.
Sample size justification
Based on a retrospective audit carried out by the Division of General Surgery of University Malaya Medical Centre (UMMC), between January to June 2019, the SSI rate post-emergency laparotomy was as high as 28.9% (N = 83).
The sample size was calculated using G Power calculator by Franz Paul from the University of Germany (Version 3.1.9.4). Since SSI was the primary outcome, the ratios of reported SSI rate post-emergency laparotomy of roughly 30% and the expected reduction in SSI rate to 7% with PICO◊ dressing were utilized. Forty patients were required in each arm to detect a difference of 23% to achieve 80% power with an α-risk of 5%. A 20% drop out rate was expected in this study. Therefore, a total of 96 patients were required i.e. 48 in each treatment arm.
Statistical analysis
All outcomes were tabulated in the data proforma and transferred to spreadsheet for analysis. Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY. Categorical data was expressed as number and percentage while continuous data was presented as mean and standard deviation if normally distributed, or median and interquartile range if non-parametric. Categorical variables (patient and study characteristics, diagnosis, CDC wound classification, level of surgeon’s training, presence of SSI, seroma, dehiscence, patients’ wound experience) were analysed using Chi Square test or Fisher Exact Test. The independent T test was used to analyse parametric data (i.e., wound length) while the Mann–Whitney U test was utilized for non-parametric data (i.e., duration of surgery, duration on antibodies, length of stay and duration of dressing). Further analysis using univariate and multivariate logistic regression were performed to determine possible predictors for SSI after emergency laparotomy at 30 days post-op; i.e. risk for SSI rates. P values < 0.05 were considered to be significant.





Comments (0)