
Remember me




Surgical stabilization of rib fractures (SSRF) began in the 1950s with instruments like cerclage wires, intramedullary devices, and clamping devices. However, it became widely accepted and popular in chest wall trauma surgery only in the past 15 years with the introduction of anatomically precontoured plates with locking screws [13, 22].
We successfully performed uMI-SSRF in 76 patients, fixing an average of 4 ribs with an average wound length of 4.2 cm. A fixation-fracture ratio of 59% was achieved, demonstrating sufficient stability for chest wall injuries [23, 24]. The average surgery time was 122 min, or 35 min per rib.
Taylor et al. utilized thoracotomy approaches and performed SSRF on 21 patients with multiple ribs fracture. They fixed a mean of 4.7(range, 2–7)ribs for a mean of 6(range, 3–10) fractures. Estimated blood loss and operative time was 98.1mL and 160.2 min respectively. The patients stayed in the intensive care unit and hospital for an average of 5.2days and 14.6 days [14]. Zhang et al. recorded the wound length in their series of SSRF with the zoning method, the average incision length was 6.2 cm for an average number of 5.3 internal fixations [21]. In the series by Schulz-Drost et al., they were able to fix 4 ribs with an average wound length of 6 to 7 cm, both posteriorly and laterally. Their average operation time was 100 min [19]. We achieved equivalent rib fixation with a shorter surgical wound and comparable operation time.
Our surgical approach follows the general principles mentioned in previous studies, utilizing a longitudinal incision through the auscultation triangle or the serratus muscle window, and minimal dissection of the trapezius, rhomboid, or latissimus dorsi muscles [20, 21, 25]. We were able to minimize our wound length due to modified reduction and plate holding techniques including lever arm reduction technique, freehand drilling and plate compression screw technique.
The optimal approach for SSRF remains controversial and largely depends on the surgeon’s familiarity with the exposure techniques. Posterolateral thoracotomy incision is a common approach for SSRF, especially among thoracic and trauma surgeons, as it provides a large view of the complete chest wall. However, the extensive muscle dissection associated with this approach can result in significant morbidity. The introduction of muscle-sparing techniques has minimized damage to soft tissues. Nonetheless, due to the extensiveness and complexity of rib fractures, without precise surgical planning and meticulous technique, a minimally invasive incision may need to be extended, ultimately resembling a thoracotomy incision. This can compromise the benefits of fixation due to the complications of a large wound. Currently, several minimally invasive surgical instruments, including upright plate holding forceps, 90-degree drills and screwdrivers, and Alexis wound retractors (Applied Medical, Rancho Santa Margarita, CA, USA), have proven helpful in reducing wound size and soft tissue damage [18]. However, each of these instruments may have its own limitations. Therefore, we successfully modified current SSRF techniques by integrating common fracture reduction and fixation techniques from orthopedic procedures, which we named ‘ultra’ Minimally Invasive Surgical Stabilization of Rib Fractures (uMI-SSRF).
There is no standard incision length for minimally invasive SSRF; however, most studies regarding this technique indicate an incision wound length ranging from 6 to 10 cm for fixing 3 to 4 fractured ribs [16, 19, 21, 26]. Our results demonstrate that it is possible to fix the same number of ribs with an even shorter incision length. Additionally, our study includes the largest number of patients among similar studies, highlighting the feasibility and consistency of this technique.
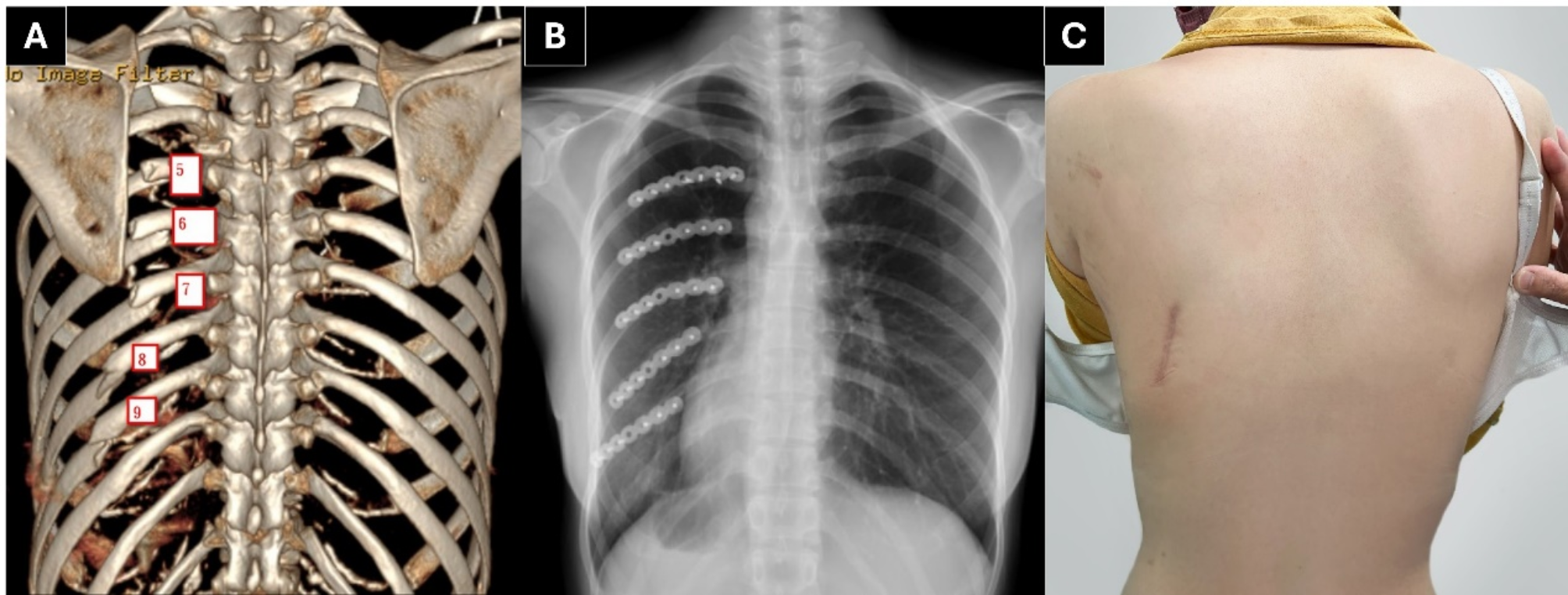
Obesity can influence surgical outcomes and affect the incision size necessary for a successful surgery [27]. Our technique can be successfully performed in patients with a body mass index (BMI) as high as 32.5 (Fig. 5). A 3 cm incision was sufficient to fix 3 posterolateral rib fractures. Langenbach et al. studied the accessible rib area with different wound lengths on cadavers and found that a minimum of 6 ribs can be accessed via a 5 cm wound through both posterior and lateral approaches [15], This provides strong evidence of the feasibility of our technique.
Fig. 5
The ultra Minimally Invasive Surgical Stabilization of Rib Fractures (uMI-SSRF) performed in an obese patient. An obese patient (BMI 32.5) with fractured 5-7th ribs fixed in a 3 cm wound
A common technique for temporary fixation involves using plate holding forceps on both sides of the plate. This requires a larger incision to secure both ends of the plate simultaneously. The fixed angle nature of the clamps limits their effectiveness in small exposures. In osteoporotic bone, the compressive force of bone clamps may further shatter the fractured bone, leaving a more comminuted fracture pattern to fix. Additionally, they can potentially injure the intercostal artery and nerves while assessing either from the superior or inferior border of the rib. It is commonly understood that the intercostal artery runs inside the concave intercostal groove. However, in certain areas, such as 6 cm from the spinous process, the artery may not be shielded by the rib [28]. Routine clamping underneath the bone poses a threat to the underlying artery and nerves, potentially resulting in unnecessary blood loss and nerve damage.
Our article discusses three reduction techniques that can all hold the fracture in a reduced state while providing sufficient counterforce during drilling of screw holes in the bone. These techniques are minimally invasive to the intercostal space and underlying structures. The lever arm technique is particularly useful when the rib is well under the skin flap.
Many studies on minimally invasive techniques have addressed the use of a 90-degree drill and screwdriver [16, 18, 19]. We prefer performing freehand drilling instead. The ability to alter the drilling angle makes it more flexible in a small surgical exposure. A deviation of less than 30 degrees does not significantly affect the compression force of the screw [29]. A potential drawback of using a 90-degree drill is the lack of clear sensation when penetrating the cortical bone during drilling. Locking screws can be secured to the plate regardless of whether they are fully within the bone, therefore screw misplacement is a common technical error with this technique.
Freehand drilling without a threaded drill guide poses the risk of penetrating underlying vital organs. However, bi-cortical drilling is a well-established technique in orthopedic procedures. With sufficient practice, a surgeon can perform this technique with minimal risk to underlying organs. In our series, no complications from penetration were encountered. In specific anatomical areas requiring special attention, such as ribs near the heart, diaphragm, or liver, using a drilling guide or self-drilling screws can minimize the risk of critical complications.
Ribs, though classified as ‘flat’ bones, are typically curved in anatomy, with inconsistent curvature radii. The outer surface of the rib is also not uniformly flat and smooth, becoming more convex to triangular posterior to the costal angle. These unique features make contouring and positioning the plate more challenging. A short segment plate reduces the effort required for contouring, particularly in addressing the ‘frowning’ or ‘smiling’ in-plane curvature. Even when plate positioning is suboptimal, using variable angle screws can improve screw purchase and, consequently, increase construct stability.
Conventional non-locking screws (Fig. 6) offer three benefits in uMI-SSRF. First, the smooth screw head presses the plate down to the bone, indirectly elevating the depressed bone. Second, the compression effect further contours the flexible titanium plate to perfection. Third, by inserting the screw eccentrically to the fracture site, it provides a dynamic compression effect. Together with the curved plate placed on the tension side of the rib, this acts as a tension band construct, shortening the fracture gap, increasing stability, and decreasing the chance of nonunion [30].
Fig. 6
Benefits of plate compression with nonlocking screws and fracture gap reduction with eccentric screw placement. A. Nonlocking screws presses the plate against the bone, indirectly reduces the depressed bone to the plate. B. Inserting 2 nonlocking screws eccentrically at both side of the fracture further shortens the fracture gap, increases stability. From AO Surgery Reference, https://surgeryreference.aofoundation.org, with copyright by AO Foundation, Switzerland [31].
There are several limitations to our study. First, this is a single center study which may affect the generalizability of the results to other settings or surgical teams with different levels of expertise. Second, the absence of a control group makes it difficult to assess whether the uMI-SSRF technique offers superior outcomes compared to traditional or other minimally invasive methods. Further studies with larger sample sizes and comparisons with other methods are warranted to verify the advantages of uMI-SSRF.
Comments (0)