For many years, colleagues around the world believed that everything had been said about the therapeutic algorithms for treating appendicitis. However, this is only the case at first glance. The various manifestations of appendicitis and their treatment methods are by no means fully discussed. For example, there is currently debate about when uncomplicated acute appendicitis can be treated conservatively with antibiotics and painkillers without worsening outcomes [3, 17, 18]. We found that only a small portion of appendicitis cases admitted to hospital, 4.34%, were treated non-surgically, with an increase from 3.6% in 2010 to 4.4% in 2022.
There are also several studies on the value of open vs. laparoscopic surgery [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. To have such discussions, the surgical results for the treatment of acute appendicitis must be clearly analyzed and published up to date. For this purpose, we used routine administrative data from health insurance companies collected from patients in the Clinotel hospital network in Germany. The aim was to use the data collected from 33,000 patients to identify possible peculiarities in the patient characteristics, treatment, and therapy of acute appendicitis.
The age and gender distribution data we collected showed that appendicitis occurs primarily at young ages; 67% of cases occurred in patients aged 49 years and younger. The gender distribution was almost equal.
Almost three-quarters of the cases (72.6%) were uncomplicated appendicitis.
This is consistent with the results of other research groups in the literature review [34, 35].
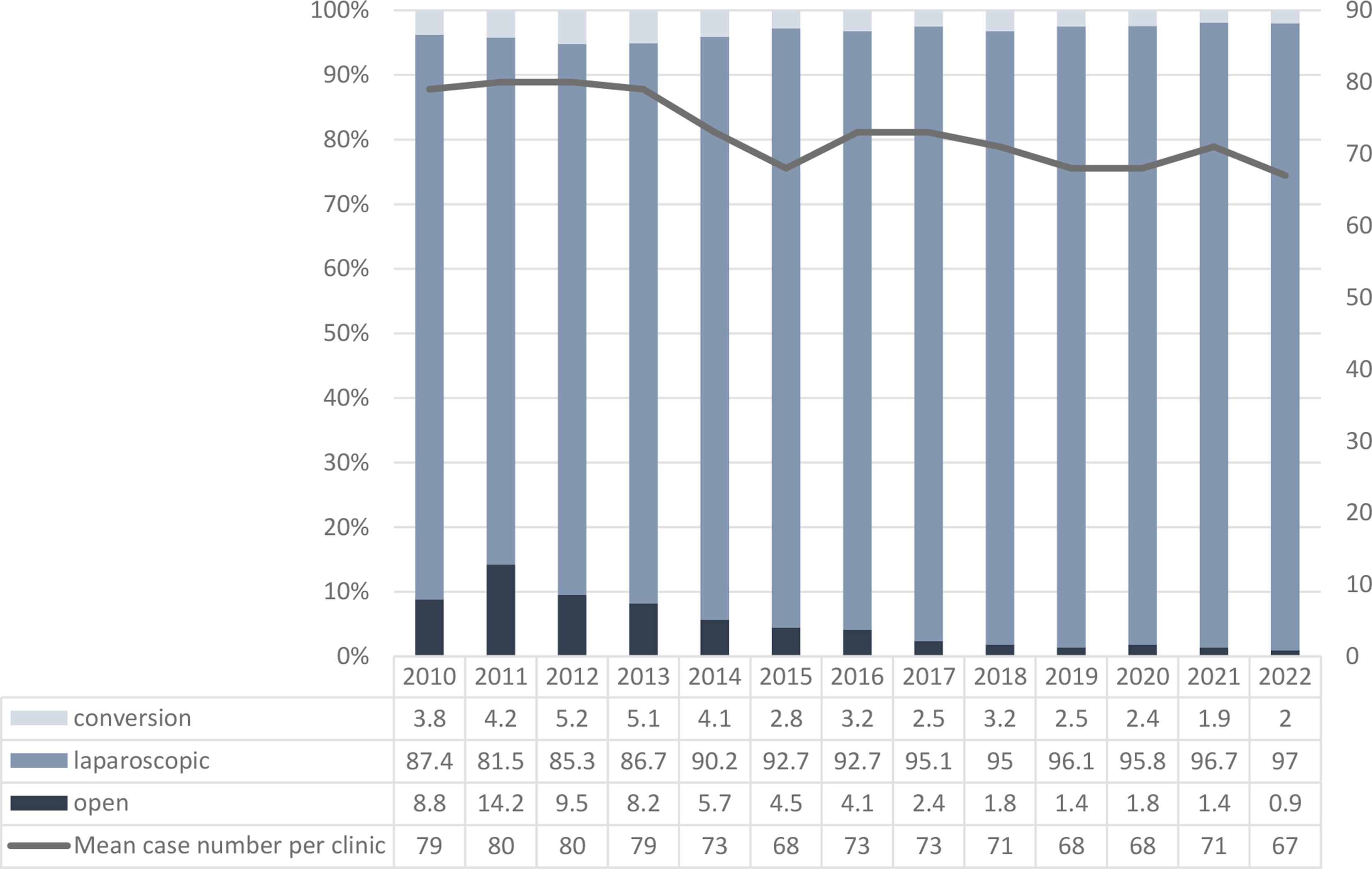
Our results show an almost complete conversion to laparoscopic appendectomy. The proportion of laparoscopic appendectomies increased significantly from 87.4% in 2010 to 97.0% in 2022 (P <.001). Appendix removal by stapler increased from 74.1% in 2011 to 85.6% in 2022. Usually the surgeon decides how the appendix base will be closed. In some hospitals in Germany the stapler is generally used. If the base of the appendix is not relevantly involved in the inflammation (uncomplicated appendicitis), discontinuation with a double Roeder loop seems also be safe [36, 37]. However, the data we use does not provide information about the reasons for the use of the procedure (stapler vs. Roeder loop).
In our opinion, open appendectomy no longer plays a significant role when considering the entire operated group; the laparoscopic approach has become the gold standard for all stages of appendicitis.
Comparing our results with the publications of other groups, the situation is not so clear. Thompson et al. reported an open surgery rate of 4.8% in 3019 patients studied, which is 2.5 times higher than in our group [38]. In another publication with over 65,000 patients from 2013, the proportion of laparoscopic procedures was only 33.8% [39]. All these results show that our study demonstrates a nearly complete conversion to laparoscopic surgery for the first time. This development took several decades. This is not surprising, as there are already theories about the introduction and spread of technologies in this context. The diffusion of an innovation involves five phases: adoption by innovators, followed by early adopters, the early majority, the late majority, and finally the laggards [40].
In addition, good ideas must be expressed through conversations (“word of mouth”). The tipping point in favor of surgical technology in this case is an average acceptance of this procedure by 20% of the users (e.g. surgeons). This clearly shows why it takes so long for a procedure to spread [41,42,43,44]. According to our study, it took 37 years from the first laparoscopic appendectomy in 1980 to achieve a continuous laparoscopic rate of over 95%.
This raises the question: How innovative is surgery today? It is time to discuss this, especially with a diagnosis as common as acute appendicitis. From our perspective, surgeons must approach such processes more constructively. In addition to the above-mentioned descriptive theories on the dissemination of innovations, we need better involvement of our professional representatives such as the surgical society, which promotes the dissemination of innovations In our opinion, the surgical societies should play a more important role in this process. Significant surgical innovations should not be left to chance or the market; this is ethically problematic. We argue that the widespread implementation of an innovation with such clear advantages as laparoscopic appendectomy should take no longer than 12–15 years. How can this be achieved? We suggest that surgical societies form innovation teams. They could rank important projects and studies from congresses or publications several times a year to identify relevant innovations. The focus should be on projects that could either relatively improve the therapy of a large group of patients or greatly improve the therapy of a smaller group of patients. The innovation teams should then develop a plan for the innovations, demonstrating the potential of new methods. This includes, for example, study planning and benefit/cost analysis. When it comes to important potential innovations, it should not be left to chance how intensively and with what resources they are pursued. As a rule, when innovations are introduced, only case studies are available, possibly in comparison with retrospective data. The innovation teams would then need to verify the results through multi-center analyses or, ideally, prospective randomized studies to promptly incorporate them into guidelines. We believe that the financing of these processes should not be left to health insurance companies or medical companies, as there is a risk of conflicts of interest on both sides. In addition to third-party funding, state funds should also be available for these processes, as the state must have an interest in promoting innovations for its citizens.
Our data concerning the surgical complication rate of 4%, intensive care unit admission of 4.4%, and overall in-hospital mortality of 0.1% (total population) is consistent with publications from other groups [45,46,47,48,49].
Our results showed that patients who underwent open surgery or conversion from laparoscopic to open surgery were significantly older than those who underwent laparoscopic surgery (P <.001). The proportion of men was highest in the conversion group (62.8%), followed by the open surgery group with 60.8% men (laparoscopic: 51.2% men; P <.001), indicating that women have a significantly lower risk for conversion to an open operation than men (p <.001). 13.0% (n = 121) of the conversion group required admission to the intensive care unit (open: 8.0% (n = 87), laparoscopic: 4.0% (n = 1149); P <.001). Accordingly, the average length of hospital stay was different among the surgical groups (P <.001). The in-hospital mortality rate was highest in the open surgery group (P <.001). A comparison of our results with publications from other groups shows similar results [13, 50,51,52,53,54].
The multivariable analyses of our cohort identified the following variables associated with conversion: increasing age (P <.001), gender (female vs. male: P <.001), and for in-hospital mortality, increasing age (P <.001) and occurrence of (a) acute appendicitis with generalized peritonitis (P <.001), (b) heart failure (P <.001), (c) neurological disorders (P <.001), and (d) a puncture/cut wound. In addition, the type of surgery is associated with in-hospital mortality (laparoscopy yes vs. no; P <.001).
Due to the size of the study, we were able to examine both the above-mentioned epidemiological data and clinical data in the multivariate analysis carried out.
Taking into account the newly published literature, this study was able to specify the risk parameters already known from other studies, such as age and gender, as well as complications and mortality. Additionally, our study identified neurological disorders as a risk factor [51, 55,56,57].





Comments (0)