
Remember me




The clinical characteristics of the 221 patients included in this study are summarized in Table 1. The patients comprised 129(58.37%) male and 92(41.63%) female with a median age of 70(60–78)(range 18–85 years). Among the 221 patients included, 88(39.82%) received non-operative treatment, and 133(60.18%) underwent surgery. Intestinal resection and ITIN concerned 89(66.92%) and 68(51.13%) of patients who underwent surgery, respectively. The mean BMI of the 221 patients was 23.09 ± 3.29Kg/m2.
All 221 patients included in the study had a documented history of abdominal surgery, which encompassed various surgical sites, including the small bowel (38.91%), colorectum (30.77%), uterus and annex (15.39%), appendix (12.67%), and stomach (2.26%).
Among the 221 patients studied, enhanced CT scans revealed small bowel necrosis in 47 individuals (21.27%), comprising 45 patients in the operative group and 2 patients in the non-operative group. Within the necrotic group of 68 patients, enhanced CT identified necrosis in 45 patients, while 23 patients were found to have no necrosis.
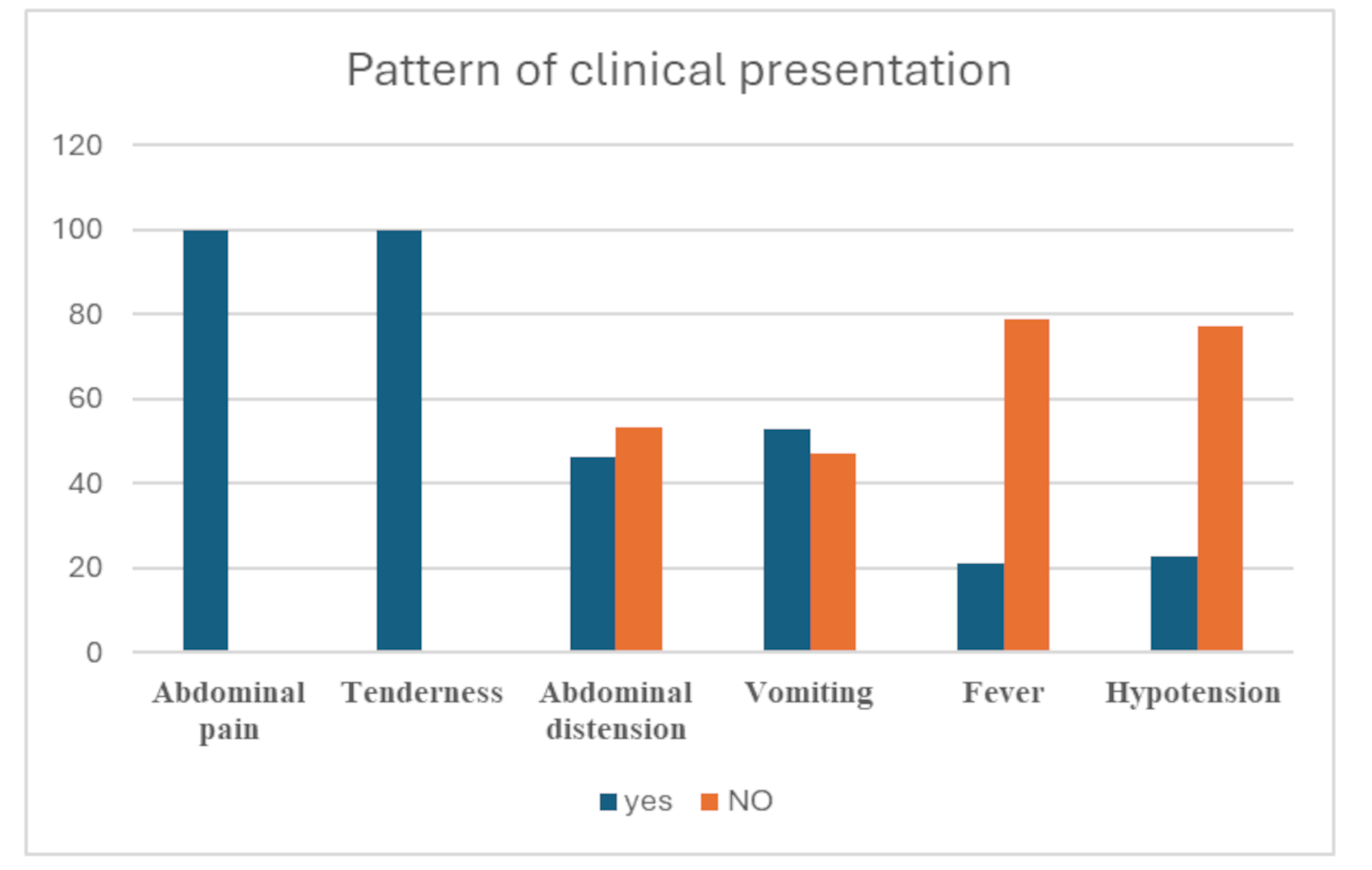
Among 221 ASBO patients 31(14.03%) patients exhibited obvious peritonitis during physical examination. In operative group, 30 out of 133 showed peritonitis, while in the necrotic subgroup, 24 out of 68 presented with peritonitis.
Distribution of serum HCY levelThe serum HCY levels of 221 ASBO patients was higher than Healthy individuals (12.01(8.75–17.40) vs. 8.78(7.51–10.35), p<0.0001) with no difference in Age (p = 0.1431) or Gender (p = 0.5797) as shown in Table 2. No significant difference in serum HCY levels was observed between male and female patients (13.42(9.44–17.94) vs. 11.3(8.48–15.85), p = 0.0599) among the 221 individuals studied with no difference in Age (70(64–77) vs. 70(63–80), p = 0.3174) as shown in Table 2. Additionally, the serum HCY levels in the 221 patients showed no significant correlation with Vitamin B12 (r = 0.0448, p = 0.5073) or folic acid (r = 0.1207, p = 0.0735). However, HCY levels were significantly correlated with endotoxin (r = 0.8052, p < 0.0001) in operative group, as well as with the non-necrotic group (r = 0.7536, p < 0.0001) and the necrotic group (r = 0.3994, p = 0.0007). as shown in Fig. 2.
Table 2 Distribution of serum HCY levelFig. 2
(A): Correlation between HCY and Vitamin B12 in all 221 ASBO patients; (B): Correlation between HCY and Folicacid in all 221 ASBO patients; (C): Correlation between HCY and Endotoxin in Operative group; (D): Correlation between HCY and Endotoxin in Non-necrotic group; (E): Correlation between HCY and Endotoxin in Necrotic group
Variant serum levels of HCY、ENDOTOXIN、IL-5、IL-6、Hs-CRP、IL-1β 、PCT、NGAL and LDH between non-operative and operative groupsThe serum levels of HCY、ENDOTOXIN、IL-5、IL-6、Hs-CRP、IL-1β and PCT in patients underwent surgery were significantly higher (p<0.0001) than in patients received non-operative treatment with no difference in Age (p = 0.0922)、Gender (p = 0.4033) or BMI (p = 0.8729), while the serum levels of NGAL and LDH showed no significance (p = 0.1345 and p = 0.0736, respectively) as shown in Table 3.
Table 3 Variant serum levels of HCY、ENDOTOXIN、IL-5、IL-6、Hs-CRP、IL-1β 、PCT、NGAL and LDH between Non-operative and operative groupsComparison of serum levels of HCY、IL-5、IL-6、Hs-CRP、IL-1β 、PCT、NGAL and LDH between necrotic and non-necrotic groupsThe serum levels of HCY、PCT、IL-5、IL-6、Hs-CRP、IL-1β and ENDOTOXIN in necrotic groups were significantly higher compared to nonnecrotic groups (p<0.0001, p = 0.0017, p = 00022, p = 0.0033, p<0.0001, p = 0.0005, p<0.0001. respectively) with no difference in Age (p = 0.0590)、Gender (p = 0.5980) and BMI (p = 0.9796). In contrast, the serum levels of NGAL and LDH between two groups showed no significance (p = 0.3171 and p = 0.1951, respectively) as shown in Table 4.
Table 4 Comparison of serum levels of HCY、IL-5、IL-6、Hs-CRP、IL-1β 、PCT、NGAL and LDH between necrotic and Non-necrotic groupsUnivariable and multivariable analyses of various biomarkers to predict ITINUnivariable and multivariable analyses identified HCY, ENDOTOXIN, and Hs-CRP as independent predictors for small bowel necrosis, with odds ratios of 1.420 (p = 0.000), 1.061 (p = 0.001), and 1.032 (p = 0.019), respectively. Among these, HCY emerged as the strongest independent predictor of small bowel necrosis. In contrast, variables such as Age, Gender, IL-5, IL-6, IL-1β, PCT, NGAL and LDH did not demonstrate significant predictive value as shown in Table 5.
Table 5 Univariable and multivariable analyses of various biomarkers to predict ITINFluctuations in different serological indicators in operative groupsThe serum levels of HCY, NGAL, IL-1β, IL-5, and LDH exhibited an initial decrease on the first day post-treatment, followed by an increase on the third day, and then a gradual decline from the fifth to the seventh day (p < 0.0001). In contrast, the serum levels of PCT, Hs-CRP, and IL-6 increased on the first day post-treatment and progressively decreased on the third, fifth, and seventh days (p < 0.0001). Notably, the serum levels of endotoxin significantly decreased after surgery and remained consistently below 5 pg/mL as shown in Table 6.
Table 6 Fluctuations in different serological indicators in operative groupsPredictive value of different indicators for ITINTo determine the serum HCY cutoff level for the diagnosis of small bowel necrosis, ROC analysis was performed on the data of the 133 patients who underwent surgery. Among these, 68 patients with confirmed small bowel necrosis were classified into the necrotic group, while 65 patients without necrosis were assigned to the non-necrotic group. Serum levels of HCY、ENDOTOXIN、IL-5、IL-6、Hs-CRP、IL-1β 、PCT、NGAL and LDH were compared between these two groups.
The ROC analysis identified a serum HCY cutoff level of 15.53 µmol/L as the optimal threshold for distinguishing between the necrotic and non-necrotic groups. The area under the ROC curve (AUC) for HCY was 0.9253 (p < 0.0001), which was significantly higher than that of other biomarkers, including ENDOTOXIN (AUC = 0.8291, p < 0.0001) and Hs-CRP (AUC = 0.7023, p < 0.0001).
HCY demonstrated superior diagnostic performance, with a sensitivity of 89.71% and specificity of 83.03%, compared to endotoxin (sensitivity = 82.83%, specificity = 62.08%) and Hs-CRP (sensitivity = 73.53%, specificity = 50.77%) as shown in Tables 7 and 8; Fig. 3, highlighting HCY as the most effective biomarker for predicting small bowel necrosis interms of sensitivity and positive and negative predictive values, in the diagnosis of irreversible transmural intestinal necrosis (ITIN).
Table 7 The receiver operating characteristic curves of different biomakersTable 8 Diagnostic value of the different markers for the diagnosis of ITINFig. 3
Receiver operating characteristic curve for different indicators in predicting irreversible transmural intestinal necrosis of adhesive small bowel obstruction
Predictive value of HCY for ITIN with patients aged 65 and elderThe 30-day mortality rate was 3.76%(5/133) in patients underwent surgery with all deceased individuals aged over 65 years, which means that the postoperative 30-day mortality rate for surgical patients aged 65 and older was 5.75%(5/87). Besides, It is important to note that these individuals exhibited a significantly elevated preoperative HCY level of 35.50(21.66–48.91) as shown in Table 9.
Table 9 Analysis of operative patientsPatients aged 65 years and older accounts for 75%(51/68) in necrotic group, whereas only 29.41%(15/51) showed peritonitis in these patients.
Among 133 surgical patients, 15 patients were admitted 6–8 h after the onset of symptoms, exhibiting a significantly elevated preoperative HCY level of 26.26(17.63–30.61). Notably, they were all over 65 years old with 73.33%(11/15) of patients did not exhibit typical signs of peritonitis. In surgical patients aged over 65 years, 58.62% (51/87) experienced small bowel necrosis among which only 29.41% (15/51) showed signs of peritonitis, while HCY was significantly elevated at 15.90(10.96–19.81). In surgical patients younger than 65 years, 36.95% (17/46) experienced necrosis, and 52.94% (9/17) of these patients showed signs of peritonitis, with an HCY level of 16.90 (11.95–22.42).
The AUC of HCY for predicting necrosis in patients with ASBO aged over 65 years was calculated to be 0.9009 (P<0.0001), with sensitivity (96.08%) and specificity (72.22%).
Comments (0)