Design
A qualitative, prospective study by means of semi-structured interviews with:
i)
patients hospitalized for COVID-19,
ii)
family members of patients who have been hospitalized for COVID-19,
iii)
HPs (physicians and nurses) caring for hospitalized patients with COVID-19.
The consolidated criteria for reporting qualitative research (COREQ) guided the reporting of our findings (Supplementary File 1).
The Braun and Clarke’s methodological framework [21] has been followed, considering the theoretical approach suggested originally in Guba and Lincoln (1989) and revisited by Luciani and Campbell (“How to critically appraise a qualitative health study”) [22]. The constructivist approach has been chosen as the epistemological stance, as the study tries to understand a specific and peculiar experience lived by the subjects, producing ad interpretation of data gathered through multiple perspectives.
Setting and recruitment
The study was conducted at the “Arcispedale Santa Maria Nuova” General Hospital, a 900-bed public hospital located in Reggio Emilia, in northern Italy, which was recently designated as a Comprehensive Clinical Cancer Center by the Organization of European Cancer Institutes (OECI).
Sample
A purposive sample of HPs from the Infectious Diseases Department was involved, together with patients who were hospitalized for COVID-19 in this Department between March 2020 and October 2021. The heterogeneity of the patient population (who received ventilation and non-ventilation intervention) and the intensity of intervention in acute and intensive care were considered.
Specifically, according to inclusion criteria, six physicians and seven nurses were randomly selected and contacted by GM using a list of names agreed upon with the head of the Department and the Head of Nursing. A list of ten patients was provided by the Head of Nursing, while family members were suggested by patient participants. The family members are those who have an informal role of care, support and closeness and who participate in the patient’s illness experience and who engage in daily personal care activities.
The inclusion criteria were:
1)
HPs who assisted patients during COVID-19 for at least one week,
2)
hospitalized patients who experienced COVID-19 and who have not been seen by or require support from the Emergency Psychology Service,
3)
family members of living patients hospitalized for COVID-19 and who have not been seen by or require support from the Emergency Psychology Service,
4)
all aged > 18.
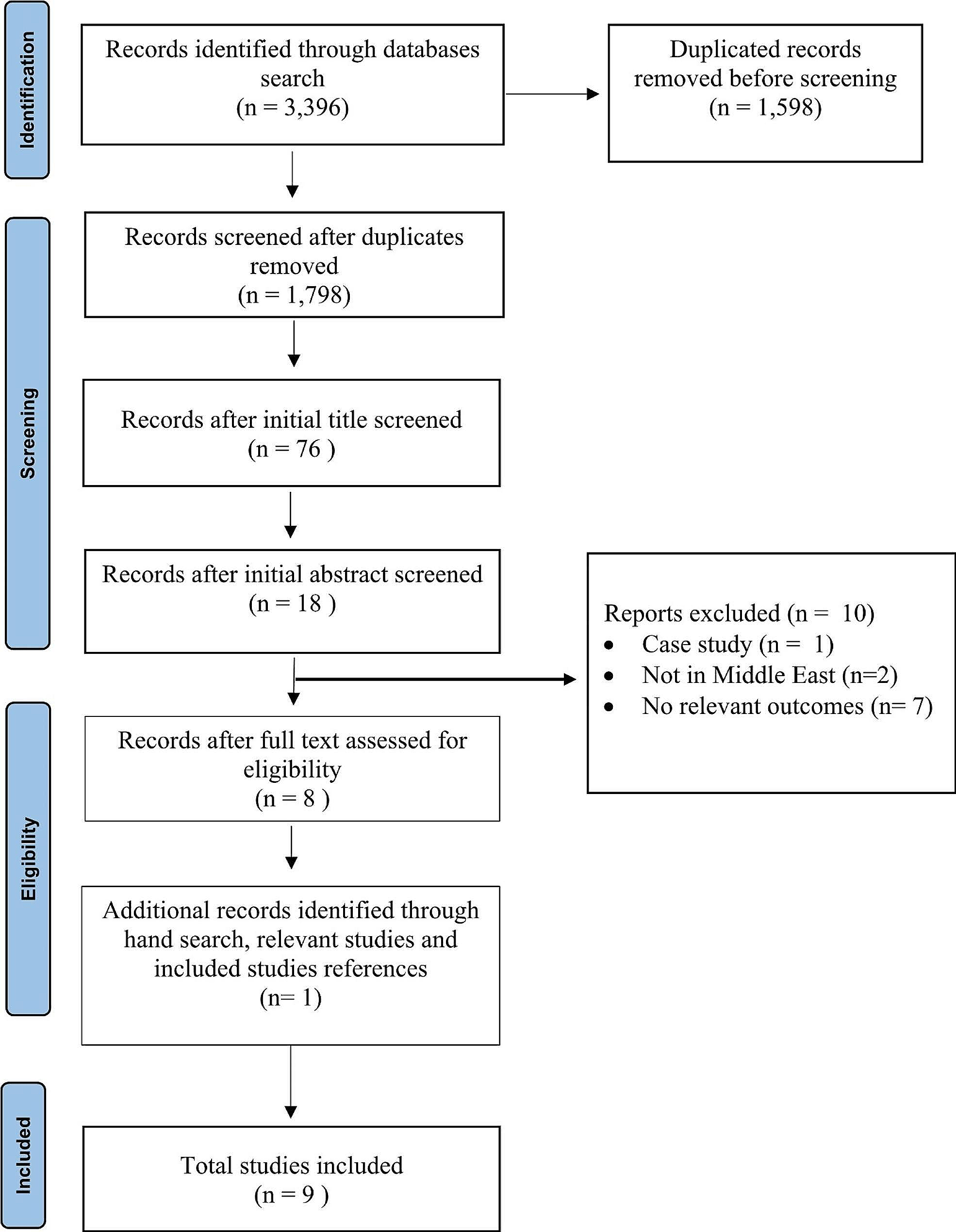
From March 2020 to October 2021, physicians and nurses cared for 2,423 COVID-19 patients.
Between March 2021 and October 2021, we selected 13 HPs and ten patients, as described previously in the “sample” paragraph.
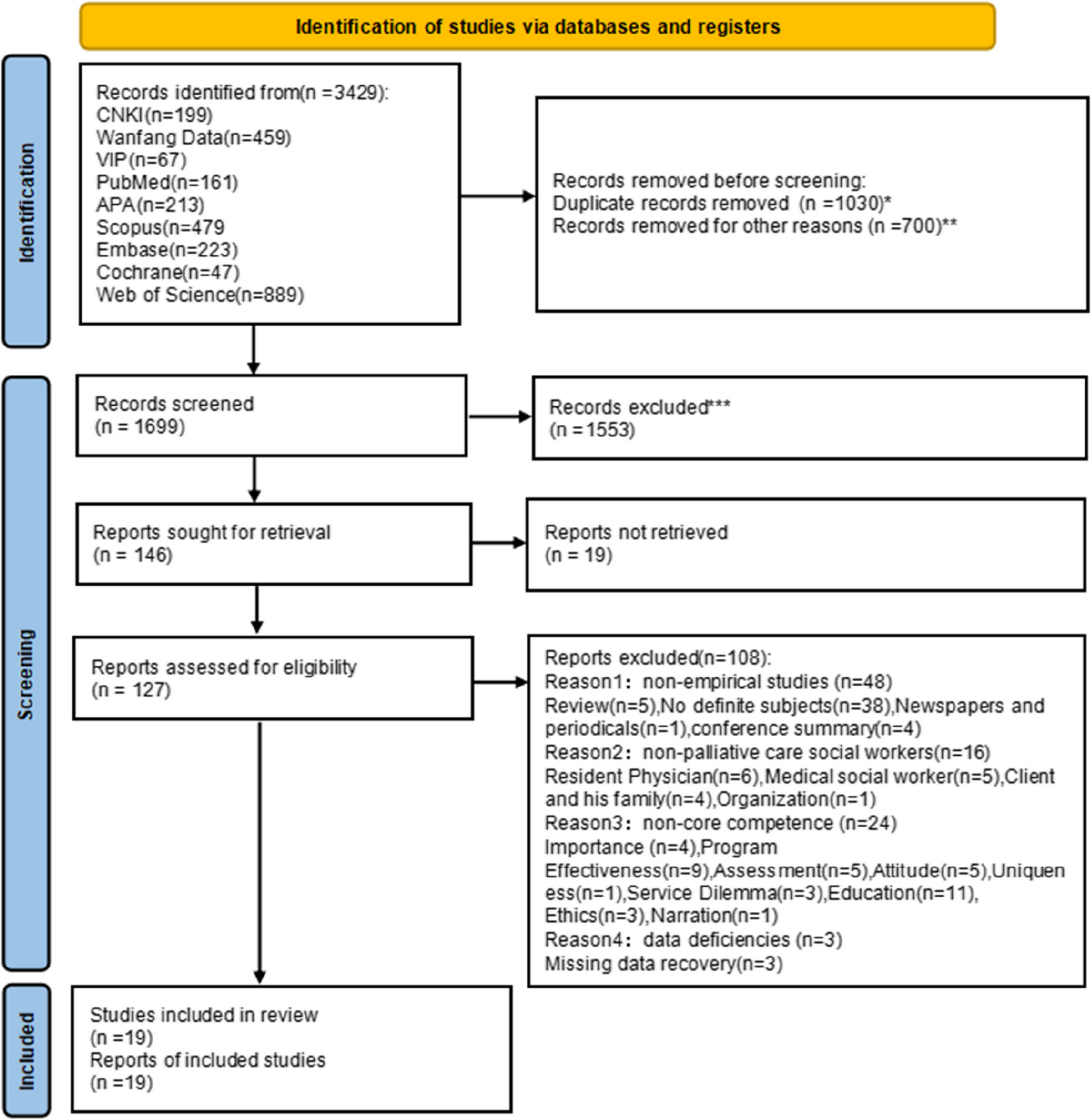
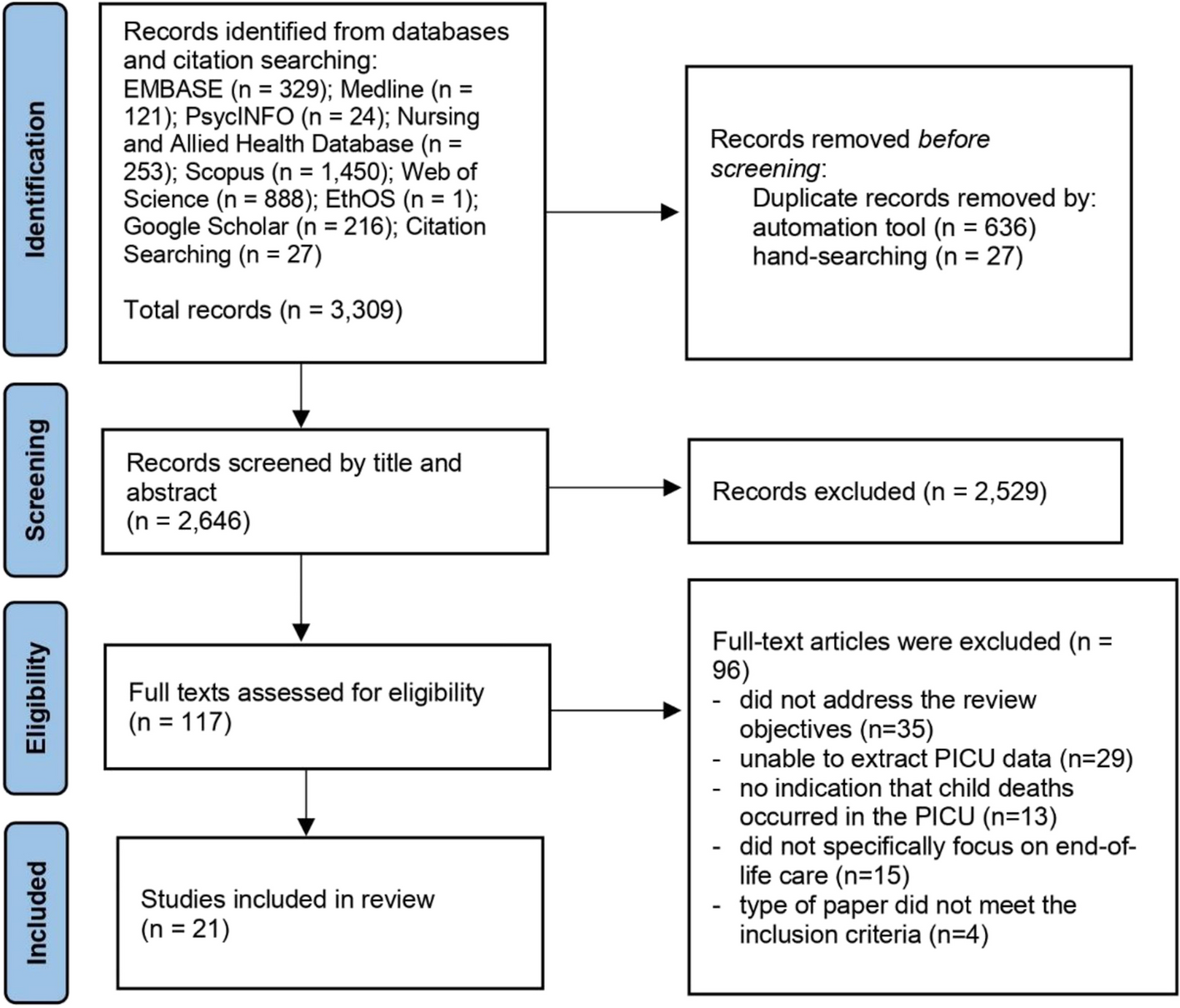
Figure 1 shows the path of selection for participants.
We interviewed 16 participants: five physicians, three nurses, and eight patients (Tables 1 and 2 provides the participants’ sociodemographic characteristics). None of the patients interviewed consented for family members to participate: they considered it important to protect them from bringing the painful memory back to the period of their hospitalization.
In particular, none of the patients expected to be interviewed on the subject of dignity. All patients told the interviewers that they had appreciated an interview on this topic and that they were able to remember difficult moments in a “protected” context where they felt supported.
Two interviews were conducted via audio call and 14 by video call; all lasted between 15 and 40 min.
Data collection
The individual interviews were conducted by video or audio call. All of the interviews were audio-recorded and transcribed verbatim.
The interviews were developed for this study (Supplementary File 2). A multi-disciplinary expert panel––consisting of a researcher and psycho-oncologist psychotherapist (LB), a PC researcher and bioethicist (LDP), a researcher and PC physician (ST), and a researcher physician (GM)––designed the interviews, after reviewing the literature on the concept of dignity in terminally ill patients. Some questions of the interviews was based on the study by Chochinov et al. that examined perceptions of dignity in patients nearing death [12]. We decided to use this model as a reference because it took the experience of patients into direct consideration. In addition, the research team is familiar with this model and employs it in clinical practice [13,14,15,16]. The interview explored how patients and families perceived dignity, and how HPs perceived the patients’ and their own dignity during the COVID-19 assistance.
The semi-structured interview let the interviewers the chance to rephrase and adapt the question to the single interviewee, specifying terms or clarifying concepts as needed. At the end of each interview, they met with a third researcher (GM) to supervise the progress of the interview.
A member of the research team (GM) contacted each patient to ask for consent to be interviewed. Two authors (LB and LDP) conducted the interviews. Before the start of each interview, written and verbal informed consent was obtained from all participants. Attention was paid to after-care, in particular, in light of the type of questions that would investigate the experience linked to hospitalization for COVID-19, participants were informed that they could speak to a dedicated psychologist if needed following the interview.
Data analysis
One author (LB) transcribed the interviews, and two authors (LDP and ST) conducted the thematic analysis based on the verbatim transcripts. The data was validated by two external researchers (LB and GM).
Interviews were analyzed as a unified dataset comprised of all interviews. The analysis process consisted of several steps, according to Braun and Clarke [21]. All researchers received a detailed guide on how to approach the analysis according to the thematic analysis. They all went through the different stages required, which were (1) familiarizing oneself with the data, (2) generating initial codes, (3) searching for themes (4) reviewing themes and (5) defining and naming them, and finally (6) the production of an initial report.
This process was designed to lead to the development of a thematic map (which aimed to visually represent the relationship between the codes/themes and the data set), a list of themes with a short definition of each theme, comprehensive inclusion and exclusion criteria (answering the question “Why does this theme include this tag and not that tag?”), and a selection of significant quotations.
The two thematic analyses were then compared to obtain a third, more robust analysis, under the supervision of a third researcher (GM). The need to reach data saturation was discussed, but was deemed not important in light of the type of interview and the research question. We used the work of Guba and Lincoln [22] to focus on credibility, dependability, and confirmability. To increase the credibility of our analysis we used triangulation of sources (as we interviewed subjects with different roles, such as HPs and patients, about the same experience), and triangulation of researchers (researchers with different backgrounds, professions, and involvement in the study, e.g., two external researchers did not conduct the interviews) [23]. Researchers’credibility was also quite relevant, as all of the researchers involved in the process had a PC background, including publications on the topic of dignity-in-care, and were familiar with the ward dynamics and routines. We also focused on the dependability of our analysis, based on achieving consensus among different coders. Furthermore, we attempted to increase the confirmability of our research by way of reflexivity [23].
Reflexivity
The interviewers, moderators, and analysts were experts in qualitative methods and were supervised by a researcher physician (GM). The authors consisted of a researcher and psycho-oncologist psychotherapist with PC experiences (LB), a PC researcher and bioethicist (LDP), a researcher and PC physician (ST), and a researcher physician (GM). The interdisciplinary analysis obviated personal interests or disciplinary assumptions. The interviewers (LB and LDP) did not have any pre-existing relationship with the participants and were external to the work settings of the HPs. They are specifically trained in conducting qualitative interviews. Moreover, they had a PC background, including published papers on the topic of dignity therapy, and they were all familiar with the ward considered. Finally, to increase the confirmability of the results, an author (HMC), external to the data gathering and analysis, provided relevant methodological feedback, and an audit trail of the analysis process.


Comments (0)