
Remember me

The experimental group (EG) hospital (UHPA) provides healthcare services to around 243 000 inhabitants, mainly in urban areas, but also in rural areas in the northeast of Madrid. The control group (CG) hospital (UHG) covers 250 000 inhabitants, both in rural areas and in the city of Guadalajara itself; it is also the reference hospital for AHSCT in two provinces of Castilla la Mancha (Ciudad Real and Cuenca). The two hospitals are university-affiliated and share similar characteristics in terms of size, staff, and range of services; and they are only 20 km apart.
The study included all consecutive patients undergoing AHSCT who met the inclusion criteria: age ≥ 18 years, signed informed consent and no significant cognitive impairment or language barrier, from March 2021 to June 2022. Patients hospitalised in the UHPA were included in the EG, while the CG consisted of patients of the UHG, given that this hospital did not have a hospital PCU.
All patients signed an informed consent form before their inclusion in this study.
Study designThis is a pilot feasibility study with a limited number of participants to assess the viability of the protocol and obtain additional information on the required sample size.
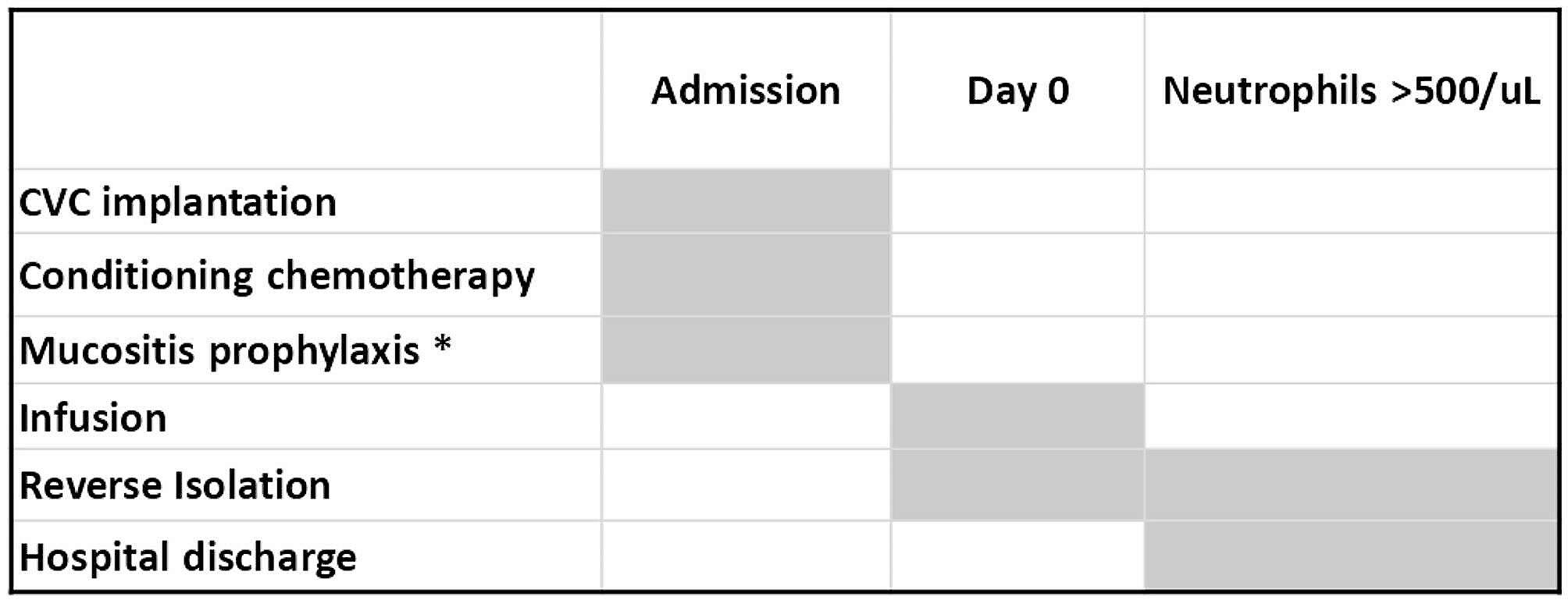
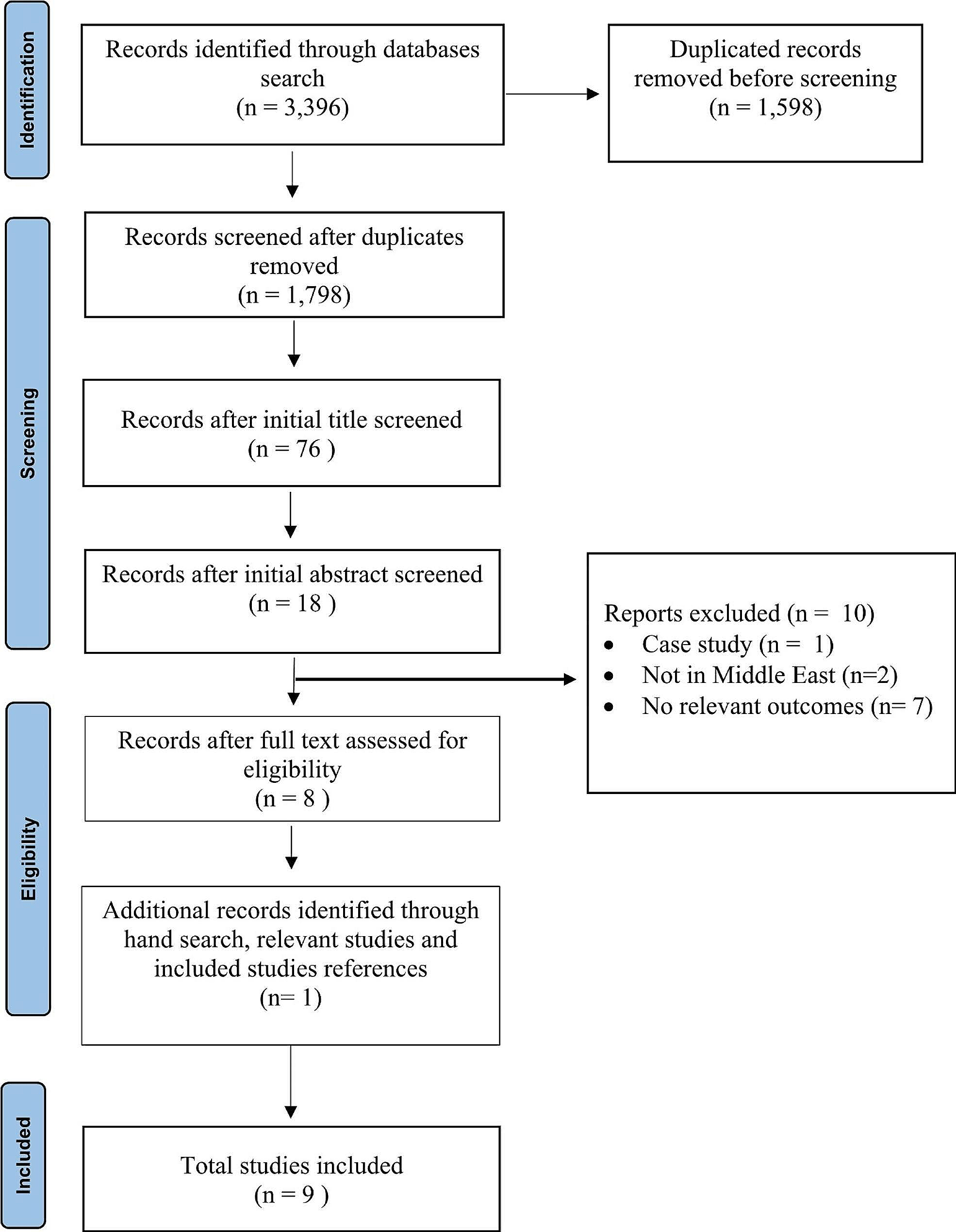
In both groups, AHSCT was conducted with a similar protocol as described in Fig. 1.
Fig. 1
AHSCT protocol AHSCT: autologous haematopoietic stem cell transplantation. CVC: central venous catheter. * The mucositis prophylaxis protocol consisted of cryotherapy during the administration of melphalan, as well as administration of Ectoin mouthwash in the case of EG patients
In addition, in the EG, the PCU of the UHPA (formed by 3 doctors, 3 nurses, a psychologist and a social worker) conducted daily visits to the patient during admission, followed by a re-evaluation after 21 days in the outpatient clinic.
Throughout these visits, the PCU systematically assessed the symptom burden at each stage of the procedure: on Days 0 (stem cell infusion), + 7 (bone marrow aplasia, acute symptoms) and + 21 (aplasia recovery), adjusting the treatment based on the observed symptoms or signs. The clinical psychologist, following an initial assessment, scheduled regular visits tailored to the individual needs of each patient and their caregivers. Lastly, an evaluation of the main caregiver’s situation was performed. If the main caregiver experienced care overload, the hospital social worker assessed the family situation and proposed personalised support measures.
Study variablesTo facilitate a comprehensive comparison of intervention outcomes, the following variables were evaluated in both study arms:
Socio-demographicAge, sex, history of anxious-depressive syndrome, baseline comorbidities and prior treatments leading up to AHSCT were collected from the electronic medical records.
Symptom burdenAssessment of symptom burden was conducted using the revised Edmonton Symptom Assessment System (ESAS), which measures 10 symptoms on a 0–10-point scale. Higher scores indicate a higher symptom burden [14]. Anxiety and depression levels in patients were gauged using the 14-item Hospital Anxiety and Depression Scale (HADS), which consists of two subscales assessing symptoms of depression (HADS-D) and anxiety (HADS-A), with scores ranging from 0 (no distress) to 21 (maximum distress). Cut-off scores above 7 indicate clinically significant symptoms [15].
FunctionalityPatient functionality was assessed using the Palliative Performance Scale (PPS) [16] and the Barthel Scale [17, 18]. Both scales, scored from 0 to 100, ascertain the degree of patient dependency and autonomy. A Barthel score below 20 indicates total dependence, while a PPS of 0% signifies death and 100% represents full functionality.
Quality of life (QoL)The Functional Assessment of Cancer Therapy-Bone Marrow Transplant (FACT-BMT) [19] was employed to evaluate patients’ QoL. Comprising 47 items across four domains—physical well-being, functional well-being, emotional well-being, and social well-being—higher scores indicate improved QoL. Additionally, a fifth domain, “additional concerns,” (23 items) addresses specific aspects related to transplantation.
Primary caregiver overloadThe reduced Zarit Scale determined the existence of primary caregiver overload, with a score ≥ 17 indicating familial claudication [20].
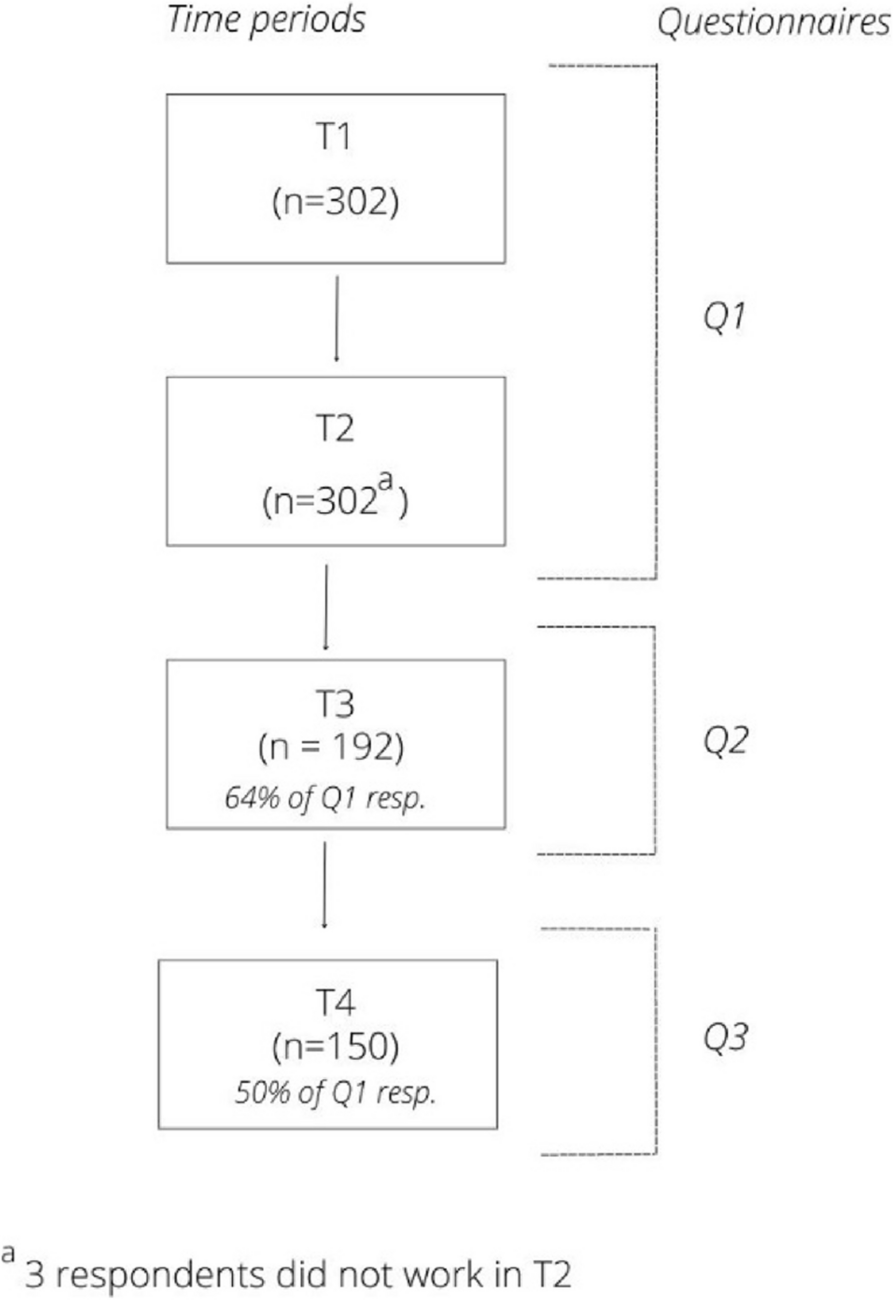
Study protocol summaryRefer to Fig. 2 for a visual representation of the study protocol.
Fig. 2
Visual representation of the study protocol
Ethical approvalThe study received approval from the ethics committee of the Hospital Principe de Asturias on 26/02/2021, with the code PAL-TASPE.
Sample size calculationTo calculate the sample size, we estimated an effect size of 0.60 standard deviations (SD), with a statistical power of 80% and a significance level of 0.05. Considering a dropout rate of 20%, it was determined that at least 20 patients per group were needed to detect significant differences between the groups.
Statistical analysisIn the analysis of demographic parameters, qualitative variables were analysed using Fisher’s exact test (2 × 2 matrices) or chi-square test (matrices larger than 2 × 2). Quantitative variables were analysed using the Wilcoxon test. For the analysis of variables collected at different time points, Kruskal-Wallis (KW) tests were used. In these analyses, the response variables used were those obtained by subtracting the value of each variable at 7 or 21 days from the value corresponding to the same patient at baseline. All statistical analyses were performed using the R statistical package (R Core ed, 2020).
ResultsForty-one patients were included in the study: 20 from the CG cohort and 21 from the EG cohort. One patient in EG was excluded due to language barrier (in the EG). Patients´ characteristics of both cohorts were comparable in percentage of males and females, age of patients, background, frequency of patients with different baseline diagnoses, conditioning regimens, frequency of patients with different lines of treatment and risk associated with the transplant process, calculated by Hematopoietic cell transplantation - specific comorbidity index (HCT-CI). (Table 1).
Table 1 Sociodemographic and medical characteristicsAll patients who underwent AHSCT during the study period, agreed to participate and all of them completed the study. No patients died during the study period.
QoL according to the FACT-BMT scale showed a statistically significant difference between cohorts at day 7 (X2KW = 20.67; p < 0.001). The total FACT-BMT value was significantly higher in the CG (median: 0.50; interquartile range (IQR): 10.75) than in the EG (median: -63.00; IQR: 128.25), and the difference was maintained at 21 days (X2KW = 29.28; P < 0.001): EG (median: -2.00; IQR: 17.75); CG (median: -129.00; IQR: 63.50). On day 0, the mean FACT-BMT in the CG was 131 and in the EG 89.35 (p < 0.001). Thus, the differences obtained in the FACT-BMT results between the CG and the SG were 41.65 on day 0, 20.75 on day 7 and 43.4 on day 21. The results obtained on the FACT-BMT Scale on days 0, 7 and 21 are summarised in Table 2.
Table 2 Mean FACT-BMT† scale on days 0, 7 and 21 in control group (CG) and experimental group (EG)Regarding symptomatic control, we found a significant difference in pain scale values between CG and EG patients (X2KW = 5.95; P = 0.01), being significantly higher in the CG cohort (median: 2.50; IQR: 3.00) than in the EG cohort (median: 0.00; IQR: 1.75). This significance disappeared after 21 days (X2KW = 0.02; P = 0.89), after the acute phase of the process. 45% of patients in the EG were using opioids on day 0 (mean 38.5 mg of morphine/day/patient), while none of the patients of the CG were under opioids. This difference was maintained throughout the admission, with 100% of patients in the third step of Analgesic Ladder belonging to the EG, versus the CG, with 95% of patients (p = 0.001).
No statistically significant differences were obtained in the rest of symptoms assessed with the ESAS Scale (Table 3).
Table 3 ESAS† scale results (median) for control group and experimental group on days 0, +7 and +21Also, no statistically significant results were obtained in terms of functionality, measured by the Barthel and PPS scales, and the HADS anxiety and depression scales.
Primary caregivers identified as at risk of overload by the reduced Zarit Scale (3 in the EG and 2 in the CG) were assessed by the social worker in both groups. The differences were not statistically significant.
Finally, a significant difference was observed in the number of total days of admission between CG and EG patients (X2KW = 24.3; p < 0.001), being significantly higher in CG patients (median: 18.5; IQR: 2.25) than in EG (median: 13.00; IQR: 2.00).
Comments (0)