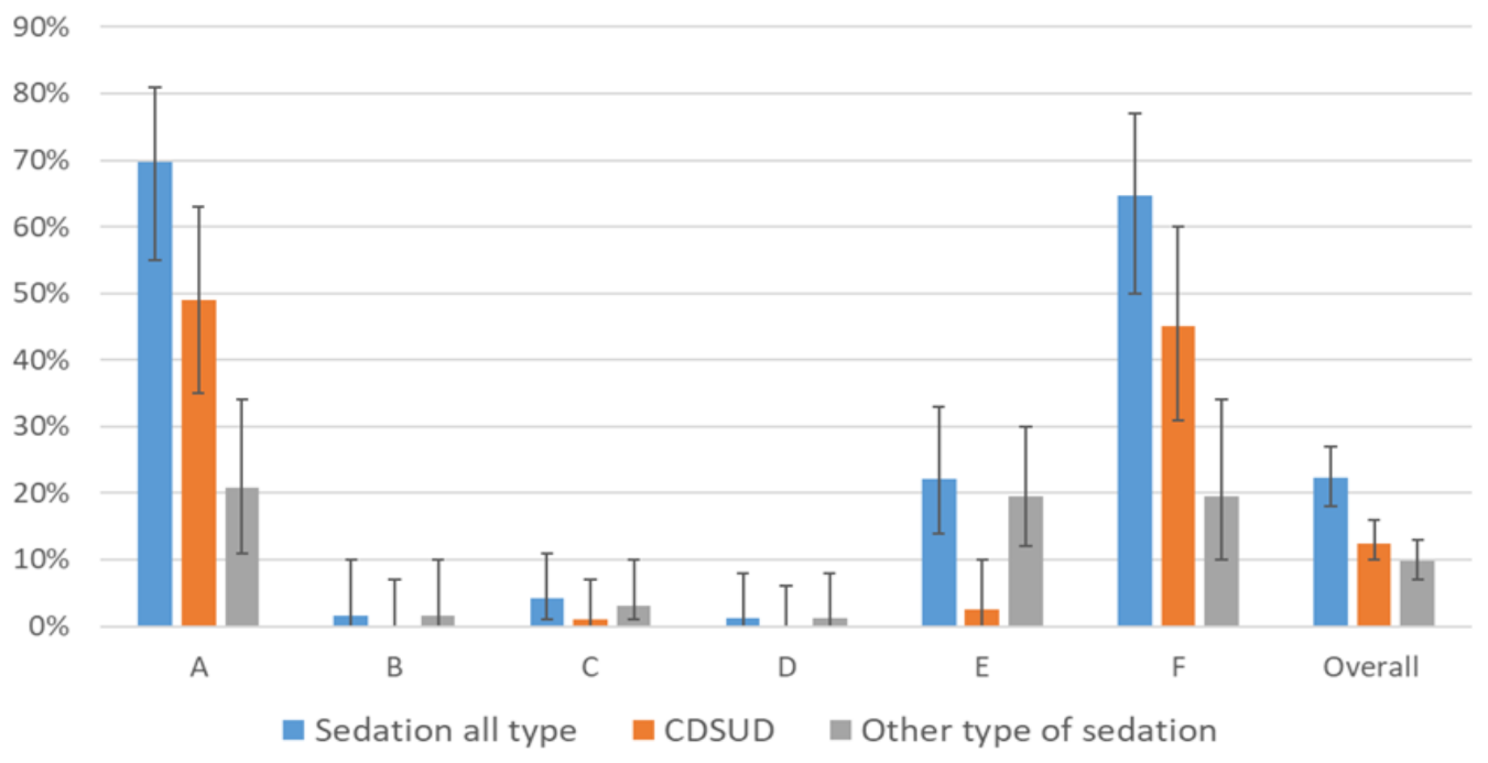
Our study emphasized the significant variability in sedation practices among French PCUs. Sedation was documented in 22% of the medical records of dying patients. A CDSUD was performed in 12% of dying patients. We identified three distinct profiles of PCUs: (1) Units with frequent sedation practices, where more than half of the patients died following the implementation of sedation, often CDSUD; (2) Units with moderate sedation practices, primarily using proportional sedation; and (3) Units where sedation practices are rare, occurring in less than 5% of patients. These findings raise important ethical questions, both regarding reluctance toward sedation in some units and, conversely, the normalization of CDSUD, which has profound implications for patients, as it marks the end of their relational life [21]. The 2024 e-Delphi revision of the 2009 European recommendations emphasizes that proportionality in PS is essential, advocating for light and/or intermittent sedation as preferable to CDSUD in most cases [22].
Sedation practices were used mainly for refractory symptoms in approximately three-quarters of the cases and for the withdrawal of life-sustaining treatment in one-quarter, almost exclusively in Unit E. This discrepancy may reflect differing interpretations of the Claeys–Leonetti law across units. The law mandates the implementation of deep and continuous sedation when life-sustaining treatments are discontinued. However, key questions remain: Should the cessation of hydration during the dying phase be considered equivalent to withdrawing life-sustaining treatment? Should sedation be initiated when a patient experiences significant disturbances in consciousness near death? The lack of consensus on these issues underscores the need for further ethical and clinical reflection.
These variations in palliative sedation practices may account for the differences in the prevalence of sedation reported in the two French studies. A national study [19] , reported an 8% prevalence of sedation practices in palliative care units, whereas a single-center study [20] , reported a 38% prevalence of CDSUD, without considering other forms of sedation.
Several studies suggest that younger patient age may be associated with a higher likelihood of receiving continuous palliative sedation [17, 23, 24]. In our study, units with a lower mean patient age had a higher prevalence of palliative sedation. However, our subgroup analysis by age indicates that age alone is insufficient to explain the substantial difference in sedation prevalence across units. No other significant differences were observed in the patient population.
Other studies have suggested that prescriber-related factors may contribute to variations in palliative sedation practices [24, 25]. These factors include religious faith and attitudes toward assisted death. From a broader perspective, we hypothesize that unit culture may play a significant role in explaining the observed difference in prevalence. PCUs appear to be conducive environments for developing mindlines, a concept described by Gabbay [26, 27] as “collectively reinforced, internalized, tacit guidelines”. Each unit seems to interpret the law differently, leading to substantial variations in practice. This may also explain the discrepancies in medication use across centers. For example, prescribing habits within a unit could account for why clorazepate is the most commonly used benzodiazepine in Unit B, whereas midazolam is preferred in other units. Similar variations in prescription patterns have been observed in Japan [28]. The omission of opioid administration data may be criticized, as these can have sedative effects beyond analgesic doses. However, we believe and hope that palliative care practitioners adhere to best practice guidelines.
The analysis of patients who received CDSUD revealed an average sedation duration of 34 h, which is consistent with the literature. However, the average midazolam dose used to achieve sedation varied significantly between Units A and F, the two units with the highest prevalence. These data suggest that assessments of sedation depth may differ across centers, despite the recommended use of vigilance tools such as the palliative version of the Richmond Agitation-Sedation (RASS-PAL), which necessitate the adjustment of sedative treatments. This may be attributed to the underuse or improper use of the RASS-PAL. Some research teams are exploring the potential of combining hetero-evaluation of vigilance with more objective techniques, such as the Bispectral Index, which could lead to a more standardize assessment of sedation depth [29,30,31].
Our study has several strengths. That is one of the few multicenter studies investigating the prevalence of sedation practices since the enactment of a law enabling CDSUD. An examination of all deceased patients within palliative care units over six months provides a more precise understanding of sedation practices in these settings.
However, this study has several limitations that should be acknowledged. First, its retrospective design inherently limits data quality and completeness. While it may have reduced social desirability bias by relying on existing medical records, the reliance on documentation that was sometimes unclear introduced interpretation bias. In cases where the intention behind sedation—other than continuous deep sedation until death—was not explicitly stated, investigators had to rely on subjective interpretation, potentially leading to misclassification, especially regarding the depth and duration of sedation or its clinical indication. Moreover, data extraction was primarily performed by a single researcher, without inter-rater reliability checks, which may have increased the risk of errors or subjective bias. Additionally, there was no standardized assessment of consciousness levels, limiting our ability to analyze this aspect in depth. Selection bias is another concern: participating centers were chosen based on self-reported prevalence of sedation practices rather than through random sampling, which may affect the generalizability of the findings. Finally, the overall response rate was low (12%), raising concerns about the representativeness of the sample. However, this limited participation may also reflect the sensitive and potentially controversial nature of the CDSUD practice within the palliative care community, which could have influenced centers’ willingness to participate.
The concept of “tacit sedation” is not clearly defined nor widely described in the literature. It originates primarily from clinical experience in palliative care, where certain sedation practices may occur without being explicitly acknowledged or documented as such. In this study, the hypothesis of tacit sedation was explored through the analysis of potentially sedative medications administered to all patients. To approximate this phenomenon, we pragmatically chose the first quartile of midazolam dosage as a threshold, acknowledging that this decision was heuristic and made in the absence of a formal or validated definition. Moreover, it was not possible to verify the appropriateness of this threshold due to the lack of standardized data on patients’ levels of consciousness or vigilance in medical records. Nevertheless, only 4% of patients without any documented mention of sedation received what could be considered a potentially sedative dose of midazolam, suggesting that undocumented sedation practices were rare in this cohort.
Unfortunately, we were not able to study the impact of drug combination on sedation. The analysis of potentially sedative drug combinations presents significant challenges. The pharmacodynamic interactions between agents such as benzodiazepines, antipsychotics, and other central nervous system depressants are complex and may produce synergistic effects that amplify sedation beyond what would be expected from each drug individually. However, quantifying this synergistic impact is difficult in a retrospective design, especially in the absence of standardized assessments of sedation depth or patient responsiveness.
The variability observed in both the frequency of sedation and the use of sedative medications highlights the need for disseminating national protocols that clearly define the different types of palliative sedation, particularly distinguishing between continuous deep sedation until death (CDSUD) and proportional sedation, and provide practical criteria for assessing the depth of sedation and evaluating patient symptoms. For clinicians, structured training programs and continuing medical education should be implemented to ensure consistent and ethically grounded application of sedation practices, especially regarding indications, proportionality, and medication use. Incorporating validated tools for assessing consciousness and discomfort could improve the quality and transparency of care.
Furthermore, a certain dissensus exists between European recommendations—which emphasize the need to initiate sedation with a proportional approach tailored to symptom severity—and the French Claeys-Leonetti law, which does not explicitly address proportional sedation. This ambiguity may contribute to the observed heterogeneity in practices. Clarifying the place of proportional sedation in clinical guidance could help bridge the gap between legal frameworks and international ethical standards. Finally, future research—particularly qualitative studies—should explore the ethical, cultural, and institutional factors influencing this variability, to support evidence-based policy and harmonized practices.


Comments (0)