
Remember me
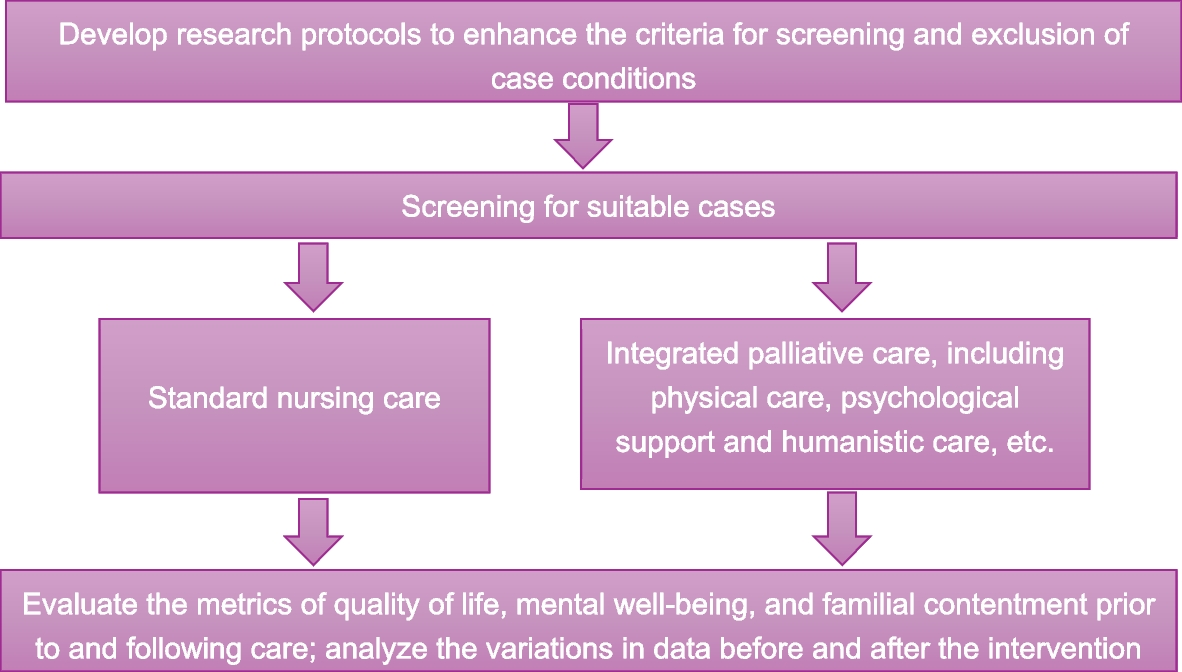
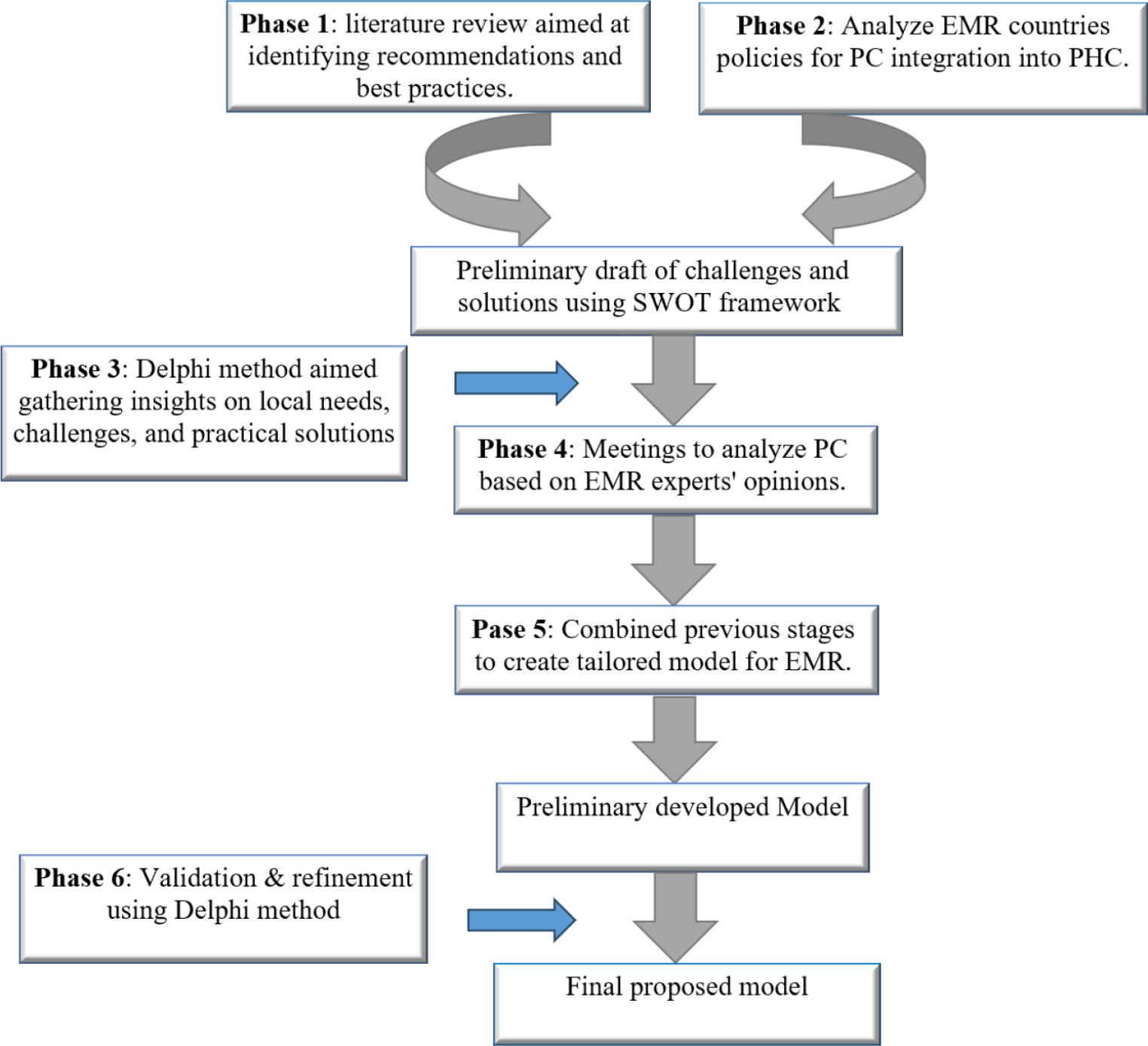
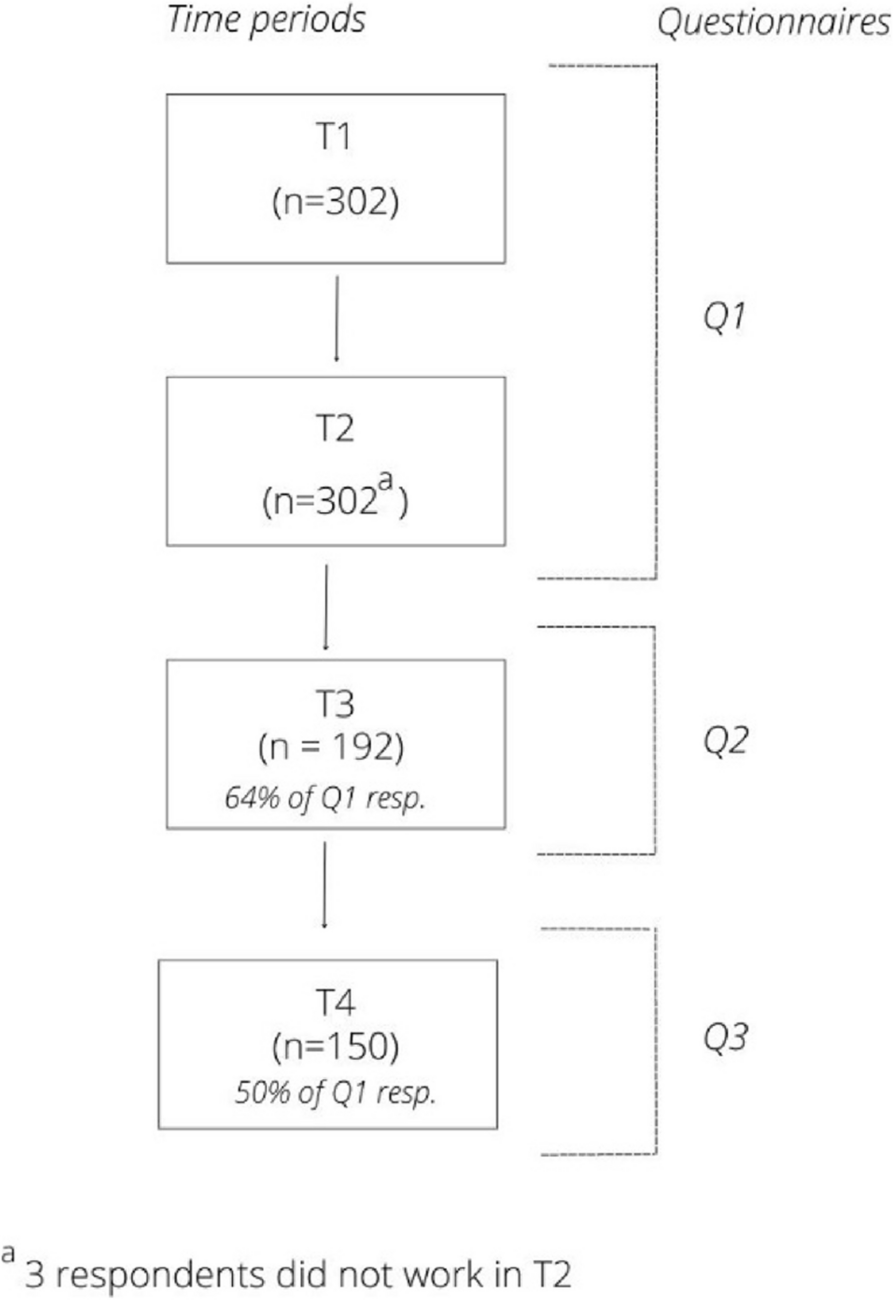

The current study was a multi-method research project, addressed separately in several sub-studies (Fig. 1).
Fig. 1
The flowchart of stages of methods. PC: Palliative Care
Literature reviewThe first sub-study involved a literature review aimed at identifying global recommendations and best practices from WHO and other relevant bodies. Information was collected from international electronic databases including PubMed, Scopus, ISI, ProQuest, Nursing Index, CINAHL, Elsevier, and ScienceDirect. English articles from 1980 to 2024 were searched using keywords such as “Palliative care,” “Primary health care,” “Care model,” “Health system,” “Integration,” “EMR,” and “Eastern Mediterranean Region.”
The inclusion criteria encompassed instructions, guidelines, and documents related to palliative care and its integration into PHC, as well as articles published in journals with various qualitative, quantitative, and mixed-method designs, all printed in English. A manual search was also conducted using Google Scholar to ensure comprehensive coverage. Exclusion criteria included conference articles, letters to the editor, commentaries, and reviews.
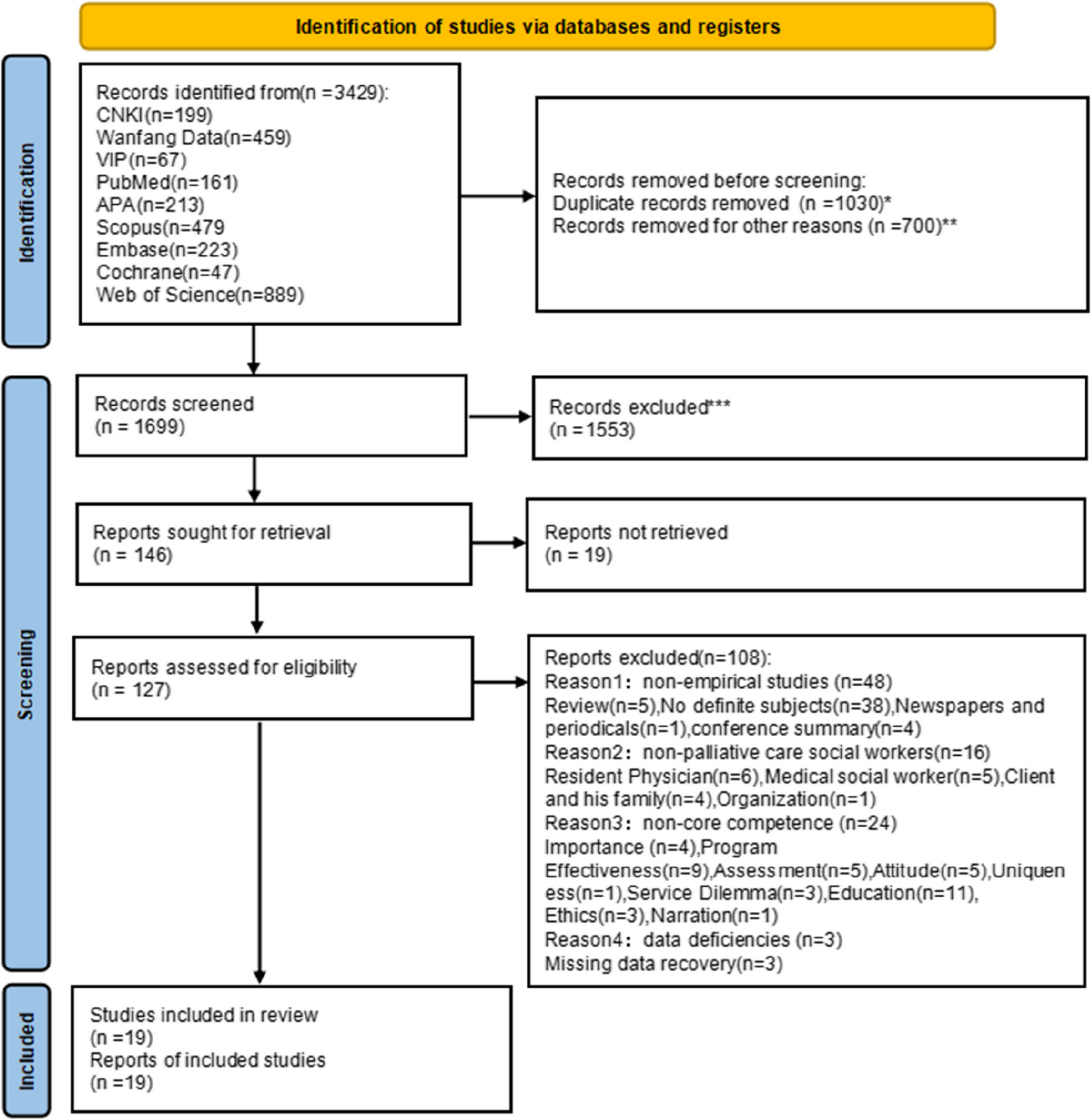
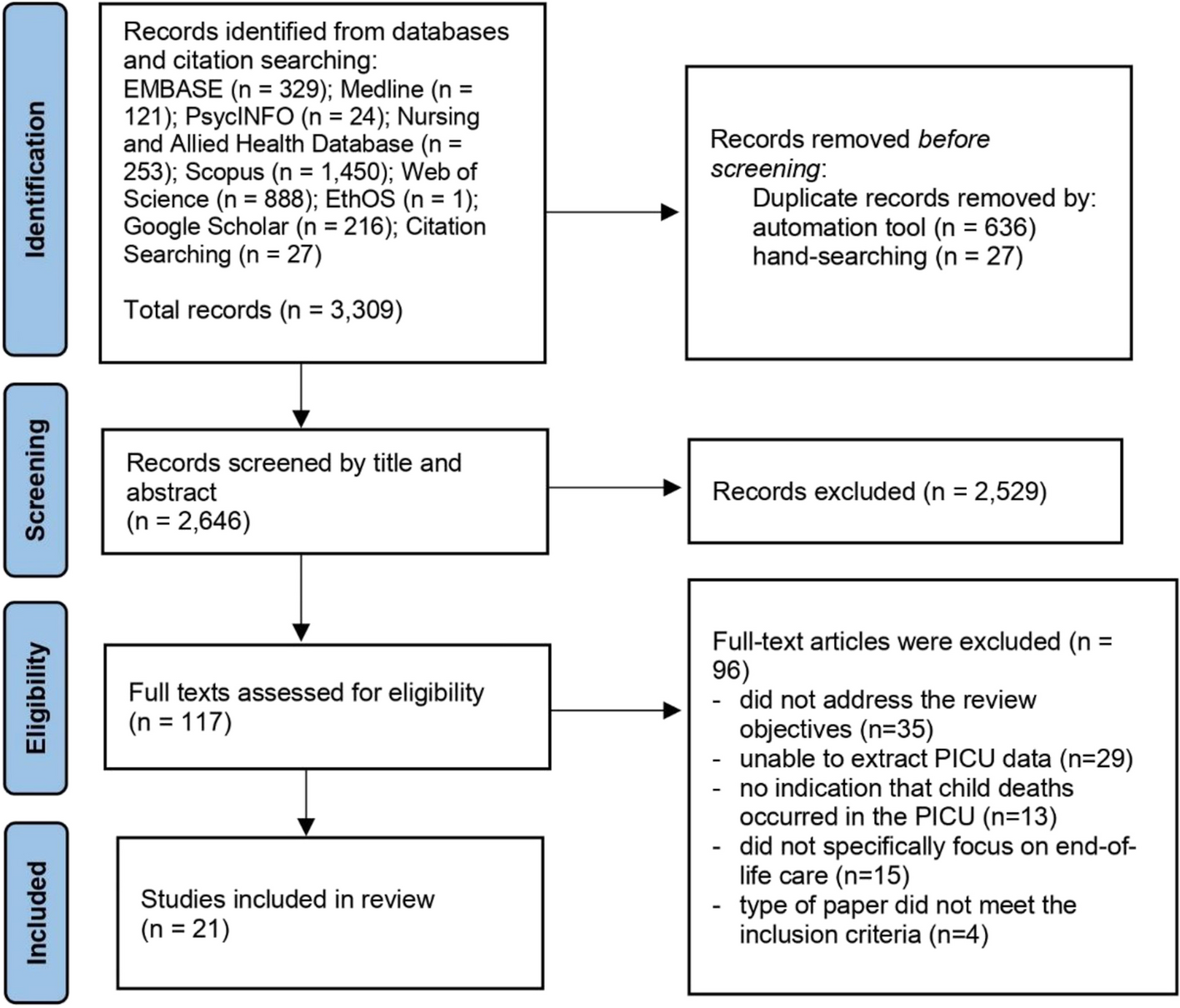
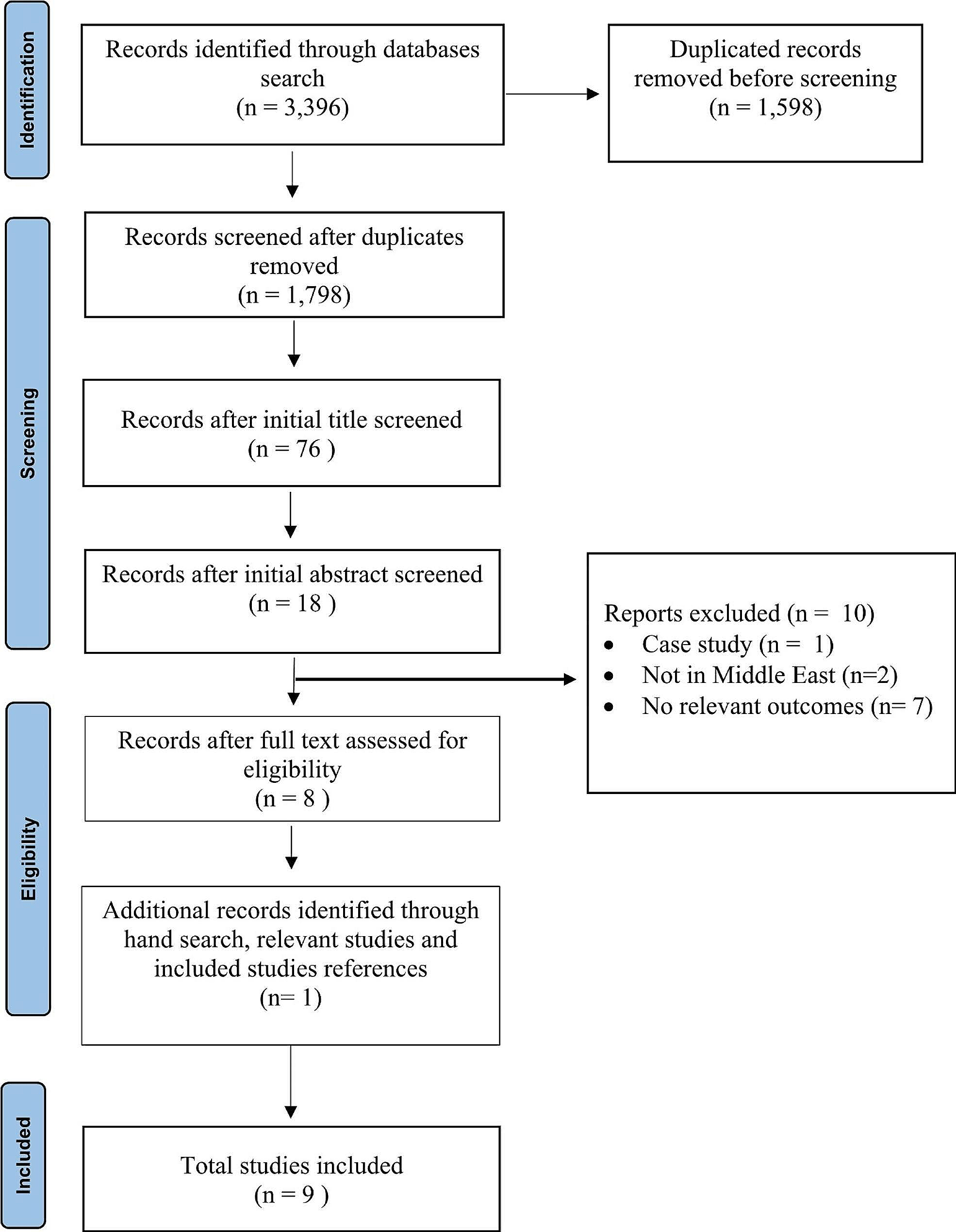
Two researchers independently evaluated the study selection stage by checking the titles and abstracts of documents and articles. Those meeting the inclusion criteria were then screened by the research team, who reviewed the full texts. The study selection process, based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist, is presented in Fig. 2.
Fig. 2
PRISMA Flowchart for the Search Strategy and Results
After extracting key concepts from the full texts, data analysis was conducted to identify and classify them according to the dimensions mentioned in the WHO guide (Drug Availability, Policy, Service Delivery, Education, Community Integration, Research). Each extracted concept was initially considered a separate code. Two researchers independently categorized these codes based on conceptual similarity. Any disagreements or ungrouped cases were reviewed by a third researcher, and the ungrouped findings were classified analogically using defined themes and classes. Finally, to ensure understanding and consistency of themes and sub-themes, the results were checked and confirmed by two additional researchers.
Policy analysisThe second sub-study was a policy analysis aimed at determining the current policies and frameworks in EMR countries to understand the existing landscape of palliative care, as well as the gaps and opportunities for integrating palliative care into PHC. The research community comprised the palliative care systems of EMR within the scope of national care programs.
To obtain appropriate data on palliative care models, databases from authoritative and governmental centers of these countries were consulted, and palliative care programs and models were reviewed. After evaluating different palliative care models, the status of palliative care programs was determined based on the dimensions extracted from the WHO guidelines.
Political documents related to palliative care, including documents, minutes, laws, regulations, guidelines, approvals, programs, reports, articles, news, meeting statements, and speeches, were identified through published sources, studies, and reports, as well as interviews with key informants from the respective countries. The documents were collected by visiting the websites of these countries, and their data were extracted after a credibility evaluation.
The output of phases 1 and 2 was a preliminary draft which was developed using the SWOT framework (Strengths, Weaknesses, Opportunities, and Threats) as the conceptual basis. According to this model, selecting an appropriate strategy maximizes a program’s strengths and opportunities while minimizing its weaknesses and threats [46].
Expert opinion (Delphi Method)This part of the research was conducted as a Delphi study aimed at gathering insights on local needs, challenges, and practical solutions for integrating palliative care which was prepared as a draft according the integrated results of phases 1 and 2. This part of the research was conducted as a Delphi study aimed at gathering insights on local needs, challenges, and practical solutions for integrating palliative care. The draft was prepared based on the integrated results of phases 1 and 2. A group of experts (n = 10), including policymakers in palliative care, regional experts, care providers, and faculty members, were selected using a purposive sampling method based on their scientific, clinical, administrative, and research experiences. Through the Delphi study, the experts provided practical solutions for integrating palliative care into PHC, drawing from the needs and challenges identified in the previous stages and their own views and experiences.
In the first round of the Delphi study, relevant experts were asked to express their answers in the form of indicators related to each component. The first-round questionnaire was designed and sent in an open-ended and unstructured format to adhere to the principles of a Delphi panel while allowing experts to freely answer the questions based on their knowledge and experiences. This approach aimed to reveal all aspects related to the subject.
Panel members were asked to express their opinions and categories regarding the questionnaire questions freely and anonymously. At the end of the questionnaire, they were asked if they considered any additional components not listed. After collecting the returned questionnaires, repeated answers were combined, and similar comments were aggregated and shortened as much as possible. The answers were then organized and grouped.
The result of this stage was the identification of the main components and the indicators related to these components, which the researchers used to create a structured questionnaire for the second round of the panel.
In the second round, participants were asked to indicate their agreement or disagreement with the indicators using scores from 1 to 5. After collecting the second round of questionnaires, the data were analyzed, and the agreement coefficient for all indicators was calculated.
At the end of each component of the second-round questionnaire, to provide another opportunity to complete the answers, participants were asked to note any additional components or indicators not mentioned, after commenting on each indicator.
Dimension-specific analysisAfter conducting the Delphi study, several meetings were held with a group of experts active in the field of palliative care from EMR countries to analyze specific dimensions based on the experts’ opinions.
Policy: Assessing the role of the Ministry of Health (MOH) in overseeing palliative care, including the establishment of a focal person or working group for policy-making and guideline formulation.
Drug Availability: Evaluating access to essential medications, such as morphine, and propose strategies to facilitate their administration and consumption at home.
Education: Developing training programs for care providers at preliminary, intermediate, and advanced levels to address various challenges in palliative care.
Community Integration: Exploring the involvement of volunteers, charities, and NGOs in providing community-based palliative care.
Service Delivery: Designing monitoring and evaluation systems to ensure service provision and continuity, supported by an appropriate payment system.
Research: Conducting needs assessments, promoting evidence-based practices, and designing evaluation indicators to measure the effectiveness of the proposed model.
Model developmentAt this stage, the results from the previous stages (literature review, policy analysis, and expert opinions) were combined to create a comprehensive model tailored to the unique conditions of EMR countries. This model emphasizes the role of community health workers, especially nurses, in providing palliative care. Additionally, the use of digital health technologies was developed to support networking, collaboration, and service delivery at home.
Validation and refinement (Delphi Method)At this stage, experts and policymakers were involved in finalizing the model. The importance, scientific validity, and operational applicability were confirmed, and the experts were asked to provide their corrective opinions. Based on the feedback and practical implementation experiences, the proposed model was subsequently modified.
The proposed modelComprehensive integration of palliative care at the PHC level involves several key steps. These include understanding the local context, assessing capacity and needs through stakeholder engagement, conducting co-design workshops, and piloting a demonstration project in selected PHC settings The project should encompass training initiatives, the establishment of a network across different levels of care, rigorous program evaluation, and a thorough cost analysis. Based on the outcomes, feasible implementation modalities can be considered for broader scale-up. These follow the afore-mentioned WHO public health model for palliative care, which includes policy, drug availability, training, community engagement, ensuring service provision, and research.
PolicyAccording to the WHO model, policy plays a pivotal role in shaping effective palliative care service delivery. Indeed, suitable policies act as an umbrella, enabling other dimensions and hence carrying greater significance than other aspects [47]. Key policies include ensuring palliative care is part of the health services provided at the primary care; establishing a national coordinating authority (e.g., a unit or department) responsible for palliative care within the MOH or equivalent; enacting laws to guarantee access to and regulation of palliative care services; and developing guidelines for delivering palliative care services in community settings [48].
A focal person for palliative care at MOH is necessary. This can be a part-time temporary appointment whose tasks include lead on writing up a palliative care strategy for the country; promoting community-based palliative care education; ensuring availability of oral opioids; might devise in the future an electronic system for oral morphine dispensing; early integration of palliative care with oncology and other chronic conditions; ensure availability and coverage by insurance for essential medications and supplies; advocacy programs; and implementation and monitoring of projects [24].
Moreover, a technical advisory group (or Taskforce) for palliative care is essential; they are the stakeholders who can be consulted and are requested to facilitate and advocate for palliative care issues. Their membership includes the palliative care specialists, head of pharmacy department, head of primary health centres, representative of Ministry of Higher education, representative from Ministry of Finance and Ministry of Social affairs (both optional), civil society, and patient/family representatives [49].
While health care professionals should be encouraged to work in an evidence-based manner, clinical guidelines and service packages can be developed by adapting well-established guidelines to each country’s unique situation and the available medications [50].
Drug availabilityA crucial aspect of palliative care service delivery in every setting involves regulating medicine policies to ensure effective and safe procurement. Policy makers are responsible for reviewing and revising laws and regulations related to drug control including registration, distribution, accountability, pricing, and prescribing methods. Additionally, their role is to monitor supply chains to ensure the availability and affordability of essential palliative care medications, including oral morphine [51].
Generally, to ensure drug availability for community-based palliative care, two main points should be considered. The first one is access to oral and injectable morphine, along with the possibility of dispensing such medications at home. The other point is availability and access to the essential list of palliative care medications at affordable prices [24].
Facilitating home dispensing of oral and injectable morphine allows patients to receive pain relief without unnecessary hospital visits. Home-based palliative care services should include provisions for dispensing and administering morphine at home, especially for patients with mobility limitations.
Palliative care relies on a range of medications beyond morphine. These include medications for symptom management (e.g., antiemetics, laxatives, anxiolytics), wound care (e.g., dressings, topical analgesics), and supportive care (e.g., antipyretics, antihistamines). Ensuring availability of this essential list of medications is crucial [52].
Additionally, high costs can be a barrier to accessing palliative care medications. Policymakers should work toward pricing policies that make these medications affordable for patients, families, and health systems. This involves negotiations with pharmaceutical companies, bulk procurement, and subsidies to reduce financial burden [53].
TrainingThe majority of palliative care needs can be addressed by health professionals trained in basic palliative care (level 1) [54], which includes communication skills, symptom management, the ethics of palliative care, and addressing social, psychological, and spiritual issues. This comprehensive training contributes to a holistic approach to patient care. Achieving this comprehensive training can occur through various avenues, including undergraduate curricula, continuous medical education programs, or pre-registration initiatives. Beyond managing palliative care issues effectively, these skills also enhance referrals to dedicated palliative care services [55].
Intermediate-level training (Level 2) is particularly beneficial for health professionals who have direct and continuous contact with patients requiring palliative care [56]. This extended training program includes specialized areas such as pediatric palliative care, practical assignments, and complex communication topics. It is essential that this training be mandatory for oncology and family medicine specialists and optional for other residents [49].
Advanced training (Level 3) is attainable through higher degrees in or residency programs in palliative medicine. Graduates from such programs play a crucial role in training professionals at other levels and supporting policy and service development. Teams comprising personnel trained at the tertiary level can effectively manage the most complex cases [57]. Of course, advanced training is not necessary for the integrated model of palliative care, especially when such services cannot be provided at the PHC level.
Community engagementUtilizing and training community volunteers to contribute to palliative care represents a promising approach, particularly in addressing social, psychological, and spiritual needs [58]. These volunteers can receive training, apply their acquired knowledge during regular home visits, and assist in identifying patients who require palliative care. Additionally, their involvement can help foster acceptance within the community [59, 60].
Empowering patients and their families as active participants in their care is crucial. Through targeted awareness programmes, patients and families can better understand their disease and its potential outcomes. Furthermore, a comprehensive, long-term public education strategy should be developed in collaboration with partners such as government agencies and community leaders. This strategy aims to enhance public understanding of palliative care over time, promoting openness and acceptance of this valuable option when appropriate [61].
Awareness-raising and advocacy efforts at the community level are essential. These efforts may include organizing seminars, distributing informative leaflets, creating posters, and establishing support groups. Collaborating with local municipalities to incorporate endowments into palliative care projects can contribute to sustainable development [26, 62, 63]. Partnerships with civil society organizations further strengthen these initiatives and ensure continuity [64].
Service provisionFor long-term sustainability and expansion, a robust system should be established to track patients who may require home care, community-based care, and end-of-life care. This system would utilize identification tools specifically designed for assessing palliative care needs, documenting diagnosis, disease stage, and performance status. An electronic platform would facilitate timely provision of care, enable consultation requests, and support follow-up through patient outcome scores. Additionally, this system would play a crucial role in quality assurance and evaluation.
As an alternative approach, consider engaging the municipality, community, or various health insurance providers to cover these essential services. Collaborating with these stakeholders can enhance access to palliative care and ensure its availability to those in need.
ResearchEvidence should inform the contextual implementation of palliative care services at PHC level. Regular evaluation of the service including costs, benefits, and quality assurance enhances informed decision making by policy makers.
In this dimension, the initial focus should be on needs assessment, a fundamental activity for determining the level of care required by the target population [65]. To maximize the benefits of integrated palliative care in PHC, data related to patients’ needs, values, beliefs, and their suffering should be collected through situation analysis. This includes an examination of the most common and severe physical, psychological, social, and spiritual sufferings [16]. Needs assessment is an integral part of the service development process, and its results should be implemented and carefully planned [65].
Another area of interest is determining the cost-effectiveness of integrating community-based palliative care into PHC. While economic evaluation for palliative care has received limited attention and the available evidence remains insufficient, existing studies indicate that palliative care is cost-saving [65].
Program monitoring and evaluation indicators is another crucial dimension in this field. Various frameworks have been proposed for evaluating palliative care programs. One such framework consists of three hierarchical levels that assess impact and outcomes for consumers (patients, families, caregivers, and communities), providers (professionals, volunteers, organizations), and the care delivery system (structures, processes, networks, and relationships) [66].
The WHO publication “Assessing the Development of Palliative Care Worldwide: A Set of Actionable Indicators” provides a refined set of practical indicators that countries can use to monitor and assess the development of palliative care in every setting including community level [42].
The proposed model for delivery of palliative care services in primary health settingsThe proposed model relies on community nurses as the backbone for conducting community palliative care, including home palliative care. These nurses can be accompanied by volunteers and other health professionals. The health professionals involved would include general practitioners from primary health centers and others affiliated with secondary or rarely tertiary health facilities. While these nurses receive basic training in palliative care, they will be supported as follows:
Networking and collaborationNetworking and collaboration between PHC staff (expected to be less specialized) and the tertiary palliative care team are recommended. This collaboration can occur through a series of training and mentoring activities, such as monthly sessions with regular constructive feedback following referrals.
Use of digital health technologiesToday, technology plays a crucial role in supporting healthcare professionals, including community nurses. The WHO defines digital health technologies as the use of information and communication technologies (ICT), digital, mobile, and wireless technologies to achieve health objectives (WHO, 2016). These technologies enhance healthcare delivery by supporting clinical decision-making and improving access to patient records and specialist consultations [67].
Notably, mHealth and telehealth are particularly important for remote monitoring, documenting patient needs and care preferences, and managing symptoms [68]. In PHC, these interventions also improve communication between patients and healthcare professionals, supporting self-assessment and symptom management [69]. However, implementing digital solutions as primary methods for healthcare service delivery requires careful consideration, including access to electronic devices, uninterrupted electricity, stable internet connectivity, digital literacy, language skills, and user-led recommendations for ongoing improvement [70].
Incorporating patient-reported outcomesDigital technologies allow for the incorporation of patient-reported outcomes into treatment plans and healthcare systems with limited resources (both human and material) and can enable informed decisions by allocating resources to those most in need [70].
Overall, supportive supervision by providers with advanced training ensures successful implementation. Obviously, establishing a system for monitoring, evaluating, and compensating such services is essential.
Care coordination is much needed between the different health facilities and primary health centres in terms of referral and back referral. Clear referral pathways for different catchment areas, as well as referral forms should be posted at the MOH website, indicating which primary health centres have end-of-life care at home (hospice@home program) [71].
The usual referral pathway for complicated cases starts with a malignancy diagnosis at specialized centers. Patients may then be referred to comprehensive health service centers or directly to home care. As depicted in Fig. 3, there is potential for reverse referrals between health service centers and home health care centers, emphasizing integrated community-based palliative care within primary health center systems. The expected competencies needed at each level correspond with these transitions. Ultimately, this integrated approach aims toward achieving ‘Good Death’ at home for patients.
Fig. 3
Integrated community-based palliative care in PHC system [76]
Here we are proposing a model, where personnel at PHC facilities can provide home care, including end-of-life care, through a system of networking and mentoring by palliative care specialists at tertiary health facilities, leveraging technology. While similar models for home care have been established in some countries within the region, they are not comprehensive and face challenges.
Table 1 shows that some requirements should have already been established in the country, (long-standing) – second row; while supplementary are additional aspects to improve palliative care services at primary health centers (PCaPHC). As such, to initiate PCaPHC, it is important to ensure access to oral morphine at home, the training of staff at PHC, and the networking with the palliative care specialists, with the supporting policies and systems in place.
Table 1 Summary of requirements for the model in terms of drug availability, education and implementationFeasibility of the proposed modelThe developed model aligns well with the conditions and requirements of many countries in the region and has practical applications. In some of these countries, efforts have been made to integrate palliative care into PHC. For example, Iran’s health system network provides basic health services and has the necessary infrastructure to implement these services nationwide.
Investigations by experts on palliative care structures in Iran indicate that community-based approaches, such as home care, are prioritized [72]. Currently, approximately 1200 home care centers are active across the country. However, the existing structures for providing community-based health services face challenges such as shortages of specialists and high costs due to lack of insurance coverage and limited access, which reduce the provision of these services at the community level [50, 73, 74].
Therefore, the proposed model in this study appears capable of addressing the challenges of home care in Iran and making its implementation more systematic.
Table 2 illustrates one such model, highlighting its challenges and proposed solutions. Palliative care at PHC can be delivered in different ways, e.g., Out patient clinics, day care i.e., admission for several hours, as well as home care, usually conducted by outreach teams or by community nurses in some settings.
Table 2 Current situation of home care by community nurses: lessons learnt from IranIn another example from Saudi Arabia, palliative care was initially available only in some tertiary and secondary hospitals, but not at the primary care level. However, in 2018, the palliative care team at King Fahad Medical City Hospital (KFMC) began integrating palliative care at a Primary Health Care Center (PHCC). Family physicians working at the PHCC were trained in primary palliative care for three months before they started providing services [75]. Therefore it seems that the proposed model is practical for creating multidisciplinary palliative care teams at the primary care level which was recognized as an obstacle.
Comments (0)