Study designs, setting, and population
In this multicenter retrospective study, we enrolled deceased acute CVD patients from ten tertiary hospitals in Japan (S1 Table) admitted between January 2014 and December 2016 from Quality of PAlliative Care in the Heart Disease (Q-PACH) study, and deceased cancer patients registered in the J-HOPE3 study (S1 Figure). This work follows the guidelines of the STROBE initiative for cohort studies (S2 Table). Acute CVD patients were defined as those who were emergently hospitalized with a primary cardiac diagnosis of acute heart failure, acute coronary syndrome, acute limb ischemia, acute arrhythmia, venous thrombosis, or other acute cardiovascular conditions during the study period. The details of the primary cardiac diagnosis are listed in Table 1. Acute CVD patients were not admitted to palliative care units and hospices in Japan. Therefore, this study was limited to CVD patients admitted to university or tertiary referral hospitals, and the rest of study procedures were similar to the J-HOPE Study, except for patient selection [17, 18].
Table 1 Baseline demographics among each datasetThe J-HOPE study is a large-scale nationwide survey aimed at evaluating the quality of palliative care for cancer patients in Japan. It targets general hospitals, hospice and palliative care wards, clinics, and other healthcare facilities, using a bereaved family survey to comprehensively evaluate the quality of end-of-life care. The first J-HOPE study was conducted in 2007–2008, followed by the second J-HOPE2 study in 2010–2011, and the J-HOPE3 study in 2014. From the mentioned J-HOPE studies, the J-HOPE3 was utilized because the study date aligned with the commencement of this study. Of the 8097 effective replies of J-HOPE 3, we used data from 682 acute hospital cancer patients (non-PCU) and 6,397 PCU patients (excluding 1,018 home palliative care patients).
While this study involves merging distinct cohort data, it is important to note that this was possible due to the similar contextual backgrounds of the research participants, allowing for comparability based on temporal resemblance, geographical alignment, and uniformity of survey measurement items [19]. In this study, we conducted a bereaved family survey without considering the timing of death. Although recall bias is important, considering the ethical barriers to conducting bereaved family surveys in CVD patients from the perspective of the trade-off with sample size, we analyzed all applicable bereaved families. Regarding the sample size, it was difficult to make an a priori prediction because the design of a bereaved family survey targeting CVD patients is very challenging, and there were limited previous reports of GDI surveys targeting such a population. Considering that the overall response rate in the J-HOPE study was approximately 60%, we enrolled as many patients as possible to extract a sample size that could withstand a three-group comparison to clarify the differences in QOL between cancer patients and CVD patients.
Criteria for selection of patients and bereaved family members
The inclusion and exclusion criteria for family members of cancer patients enrolled in J-HOPE have been described in detail in previous studies [20]. Details were collected for all CVD patients from ten tertiary hospitals admitted between January 2014 and December 2016 who met the following inclusion criteria: (a) patients who died at the hospital; (b) patients aged 20 years or older; and (c) bereaved family members aged 20 years or older. The exclusion criteria were as follows: (a) no identifiable address for the bereaved family members; (b) family members with severe psychological distress as determined by their primary physician; and (c) family members incapable of completing the self-reported questionnaire [17]. This study focused on GDI and overall care satisfaction to compare the quality of death between CVD and cancer. Family members who refused to participate were excluded after collecting the responses.
Questionnaire sending protocol and consent obtaining
The set of paper copies of the questionnaires was sent to bereaved families from each participating institution, along with a letter explaining the survey, from July 2017 to August 2018. This wide range of sending schedules was due to differing timings of approval of each hospital’s institutional review board. Incentives to participate included a ballpoint pen in the envelope. The participants were asked to return the completed questionnaire to the secretariat office (St. Luke’s International Hospital) within two weeks. A month after the initial mail, non-responders were sent a reminder. In case of unwillingness to participate, they were asked to check a “no participation’’ box with the reason and return the incomplete questionnaire.
In this study, participant information was given and informed consent was asked to the families of CVD patients at the beginning of the questionnaire, and the patients’ families completing and submitting the questionnaire. As for the data from the 2014 J-HOPE3 study targeting cancer patients’ families, consent for data use had already been obtained from the patients’ families at the time of patient registration in the previous J-HOPE3 study, and new consent was obtained through an opt-out process [17, 18].
Outcome measures and questionnaires
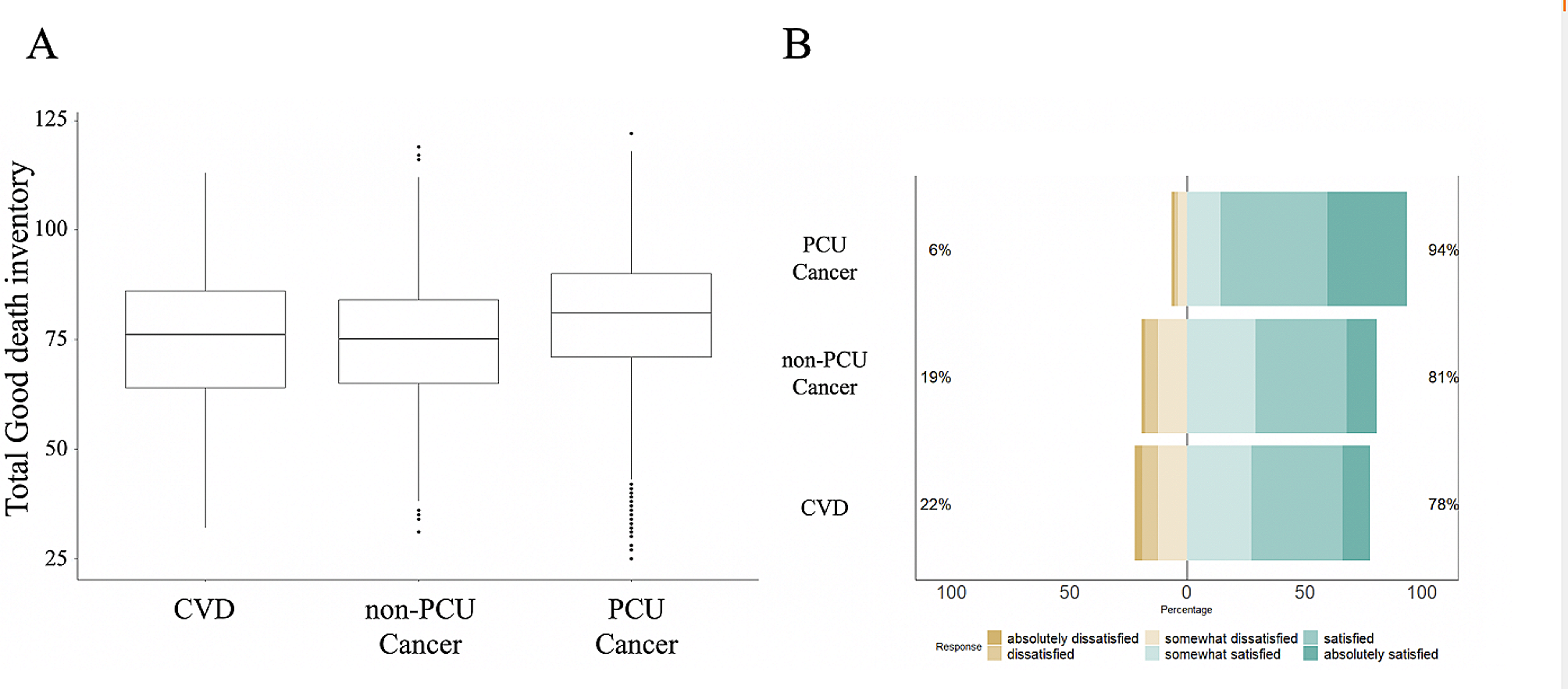
The primary outcomes were the total GDI score (continuous variable from 18 to 126), overall care satisfaction (satisfied or not), by bereaved family members, and the achievement (achieved or not) of the core ten attributes of the GDI by bereaved family members.
The questionnaires of this bereaved family survey is composed of the same content as previously used in the J-HOPE study, and common questionnaires, including the GDI [13, 17] and other popular validated questionnaires including, the Care Evaluation Scale (CES) [21, 22], Patient Health Questionnaire 9 (PHQ-9) [23], and the Brief Grief Questionnaire (BGQ) [24, 25], were collected as original forms in the survey. To maintain consistency with the questionnaire conditions in the previous J-HOPE3 study, we conducted a bereaved family survey consisting of the aforementioned questionnaires and utilized the “GDI” and “overall care satisfaction” from the survey. Regarding the questionnaires for GDI and overall care satisfaction, we used the exact same questionnaire content as in the previous J-HOPE3 study. The questionnaire comprised 15 pages (120–140 items in total) and took approximately 20–30 min to complete. Additionally, the participating institutions were requested to collect data on age, gender, and the chief cardiovascular diagnosis.
- good death inventory—short version
The GDI was originally developed for families of cancer patients and has demonstrated high reliability and validity. The total GDI score was calculated by summing the scores for all attributes. The total GDI score, which has been validated in previous reports to evaluate the degree of achievement of a good death from the perspective of bereaved family members in Japan, has been demonstrated to indicate the attainment of a good death when scores are high [26, 27]. Moreover, preliminary investigations of the research have also shown high reliability and validity when applied to families of non-cancer patients [13, 28]. We used the short version of GDI to measure whether patients experienced good death from the perspective of the bereaved family members. The original version of the GDI consists of ten core and eight optional domains and 54 attributes. The 10 core domains evaluate the attributes that Japanese people consistently rated as important, and the eight optional domains assess the attributes that are rated as important inconsistently and depend upon individual values [13, 17]. The short version comprised 18 representative items from each domain, and the validity and reliability of the scale were confirmed. The participants evaluated each attribute using a seven-point Likert-type scale (1 = absolutely disagree to 7 = absolutely agree).
- overall satisfaction
The question to the participants about their overall care satisfaction to examine concurrent validity was: “Overall, were you satisfied with the care in the hospital?” Using a six-point Likert scale, they answered from one (absolutely dissatisfied) to six (absolutely satisfied).
Statistical methods
Continuous variables are presented as the mean ± standard deviation (SD), and categorical variables are presented as proportions (counts). Baseline covariate distributions were compared between the CVD, non-PCU cancer, and PCU cancer patients, using the Student’s t-test for continuous variables and one-way ANOVA for categorical variables.
For overall care satisfaction perceived by bereaved family members, ‘‘somewhat satisfied,’’ ‘‘satisfied,’’ and ‘‘absolutely satisfied’’ were collapsed into “satisfaction with overall care;” and for each component of GDI, ‘‘somewhat agree,’’ ‘‘agree,’’ and ‘‘absolutely agree’’ were collapsed into “achieved good death” to illustrate the distribution of scores and perform binary logistic regression later.
First, as an univariable model, GDI total scores and overall care satisfaction were compared among the bereaved families of CVD and cancer patients (in PCU and non-PCU), using a Kruskal-Wallis test to detect differences in median values across these three groups. Post-hoc pairwise comparisons were conducted using Dunn’s test with Bonferroni correction (p-value adjusted) to identify which groups differed significantly from each other.
Second, to estimate the difference of perceptions by bereaved families between CVD and cancer patients (in PCU and non-PCU), multivariable linear regression was performed for the total GDI score adjusted by covariates; the baseline patient characteristics (patient age, gender, disease duration, and physical status before admission) and baseline participant characteristics (participant age, gender, relationship to the patients, health status during the caregiving period, frequency of attending to the patient, and presence of other caregivers) [14].
Third, binary logistic regression models were performed for overall care satisfaction (“satisfied with overall care”) and for each component of GDI domains (“achieved good death” in core ten and optional eight attributes) perceived by bereaved family members to evaluate the impact of CVD on each GDI domains, adjusting the same covariates in the multivariable linear regression.
Furthermore, we performed sensitivity analyses by categorizing the patients into several cohorts to account for the unique trajectory of disease progression among CVD patients. In particular, since the responses to GDI, and overall care satisfaction may differ depending on the relationship between patients and the bereaved family, stratification by the target family was fundamentally important. Sensitivity analyses were conducted for patients who had received CVD/cancer treatment for over one year, patients with CVD limited to heart failure or cancer, patients with bereaved family members restricted to spouses or children, and an additional sensitive analysis focused on patients who had not received palliative care.
To confirm the robustness of the results, we performed propensity score matching using patient age and sex, and bereaved family member age and sex among the three groups: CVD, PCU cancer, and non-PCU cancer. Excluding two CVD patients with missing data on bereaved family members’ age, propensity scores were calculated and matching was performed for two comparisons: Bereaved family members of Cancer non-PCU vs. Cardiology, and Bereaved family members of Cancer PCU vs. Cardiology. Propensity scores were estimated using a non-parsimonious multivariable logistic regression model that included the variables Patients’ age, Patients’ sex, Families’ age, and Families’ sex. Matching was performed using the one-to-one matching protocol without replacement within a caliper width equal to 0.2 of the standard deviation of the logit of the propensity score. A total of 241 pairs of patients were successfully matched. Analyses were performed using R version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria), and a two-sided P-value < 0.05 threshold was used to determine statistical significance.


Comments (0)