
Remember me
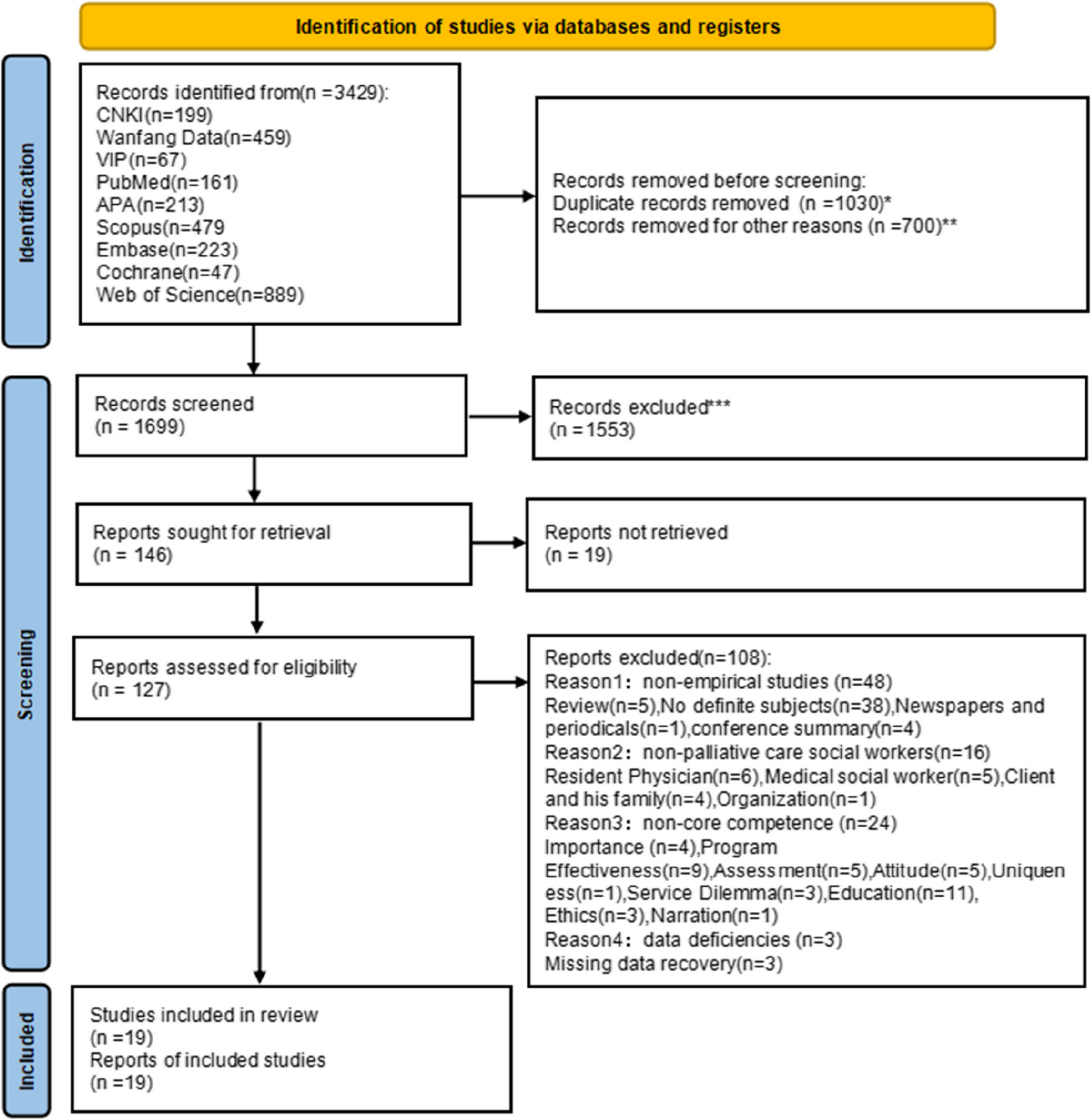
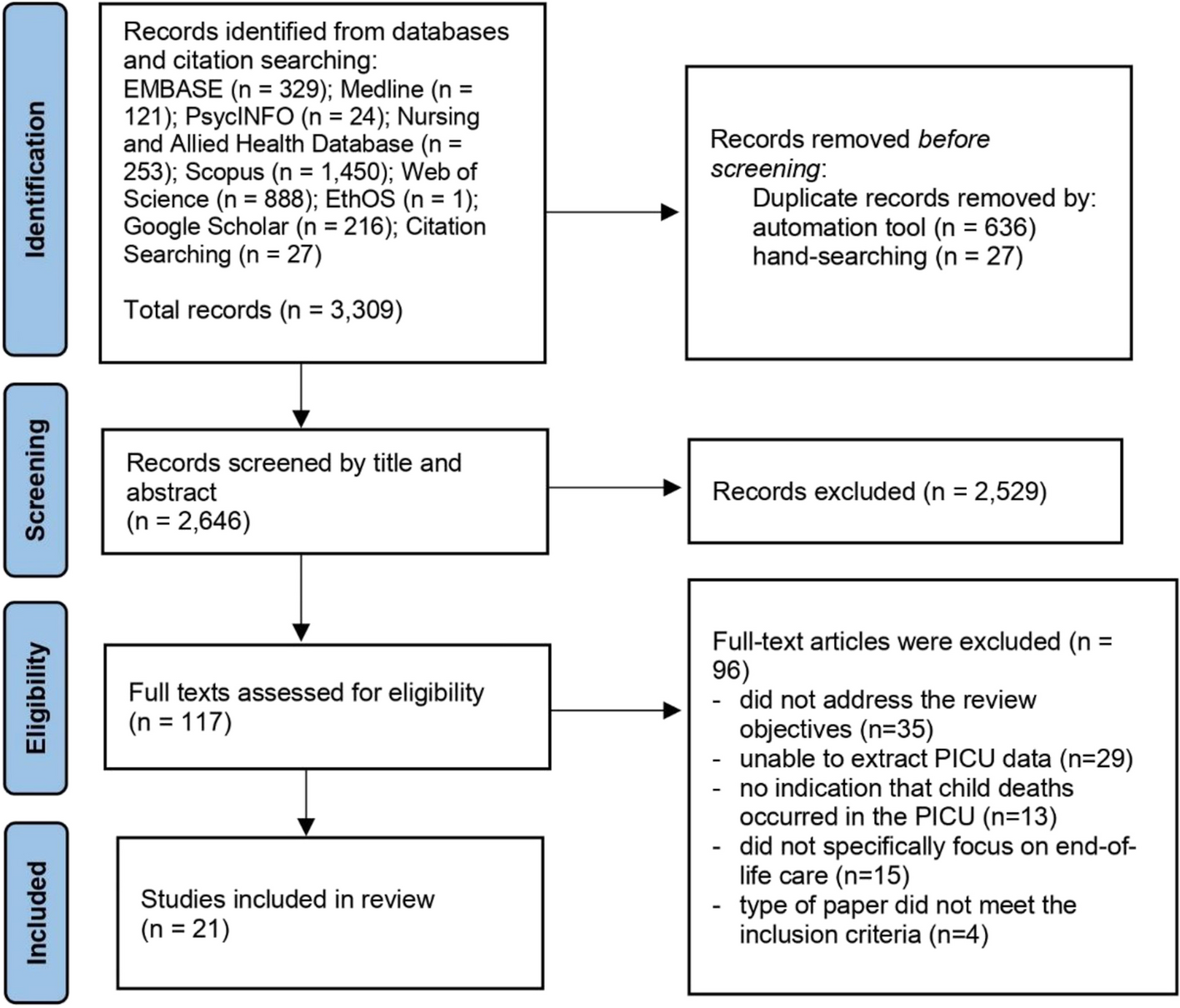
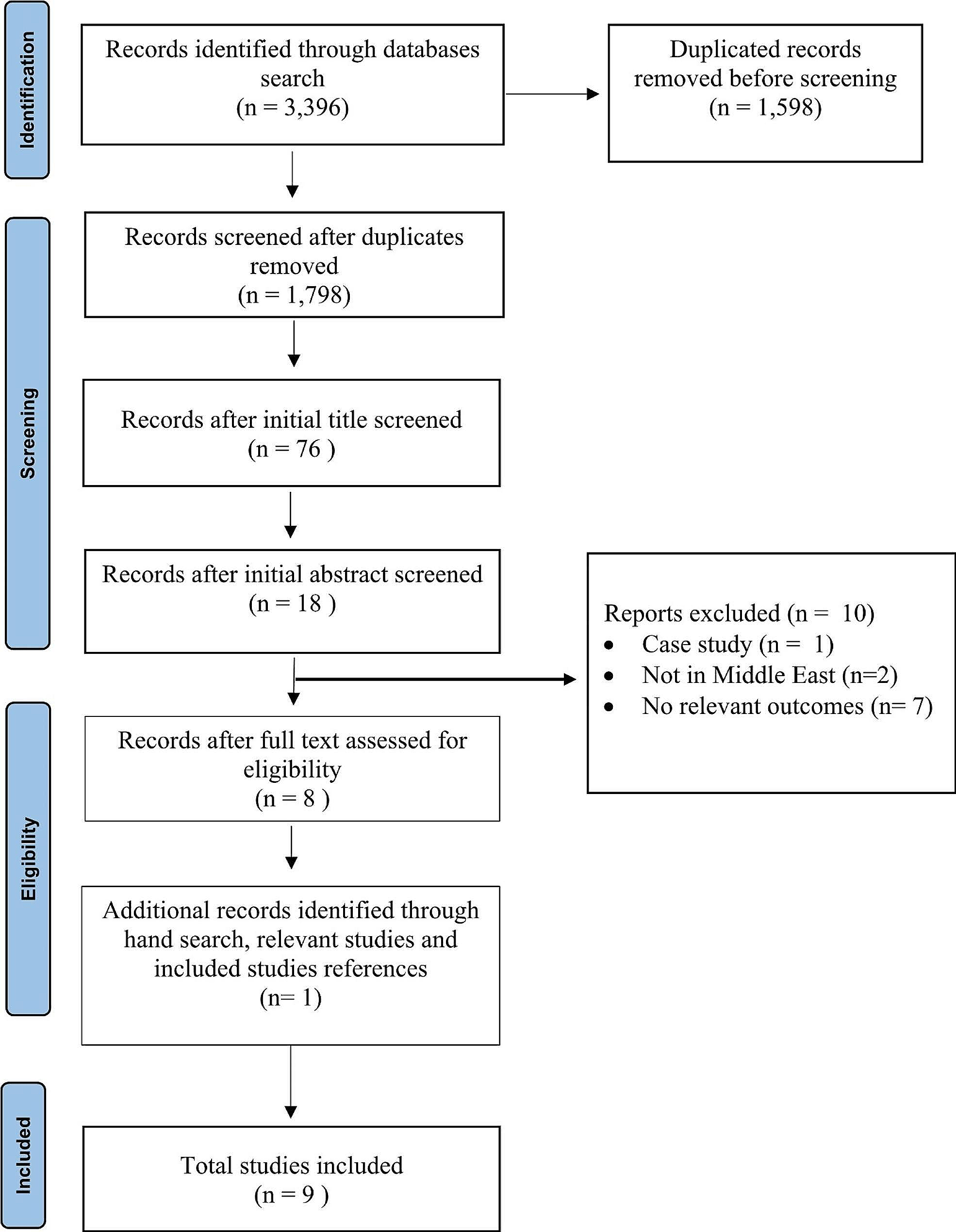

A total of 3,309 papers were retrieved from databases and citation searching. After removing duplicates, 2,646 remained. Of these, 2,465 papers were discarded at title/abstract screening level. The remaining 117 papers were examined at full text level. Ninety-six did not meet inclusion criteria, which left 21 papers to be included in the review (Fig. 1).
Fig. 1 Study characteristics
Study characteristicsThe 21 papers included in this review (Table 3) reported findings from across the globe: 5 (23.8%) from Europe, 5 (23.8%) from Asia, 4 (19%) from South America, 4 (19%) from North America, and 3 (14.3%) from Australia. Twelve (57.1%) articles reported studies that had used a qualitative approach, 7 (33.3%) were quantitative studies, and 2 (9.5%) were mixed-methods studies. In 12 (57.1%) studies, participants were healthcare professionals, in two (9.5%) studies participants were bereaved parents, six (28.6%) studies had paediatric patients as participants, and one (4.7%) study had healthcare professionals and family as participants (Table 4). Most of the included papers (18 out of 21) were of very good quality (meeting 90–100% of the critical appraisal criteria). The remaining papers were of good quality (meeting 71–77% of the critical appraisal criteria). (Table 3, available at the end of the manuscript, and Table 4 around here).
Table 3 Summary table of the studiesTable 4 Study characteristicsElements of end-of-life care in PICUThe analysis of the papers’ findings resulted in identifying three elements in end-of-life care provision for children in the PICUs: (1) Assessment of entering the end-of-life stage, (2) Parental decision-making at the end-of-life, and (3) End of life care processes consisting of care provided during the dying phase, care provided at time of death, and care provided after death. The roles of HCPs were mentioned in every stage in the care provision.
Assessment of entering the end-of-life stageThree papers [48, 49, 51] raised issues on the recognition of end-of-life and concluded that a consensus is required among the HCPs involved to determine a patient entering end-of-life. Nevertheless, different approaches to end-of-life assessment and recognition were reported in each study. According to Mitchell and Dale [51] nurses were commonly the first HCP to recognise deterioration in the condition of children towards the end-of-life. Nurse participants in the study by Poompan et al. [48] conveyed that all children admitted to the PICU were assessed daily by nurses using the Palliative Performance Scale of Children (PPSC) to allow them to initiate appropriate care plans. However, nurse participants also mentioned that they could not provide care as planned because they had to wait for doctors’ decisions. In the same study, doctors used more subjective methods of evaluation when deciding on a patient’s prognosis, for example the patient’s response to treatment, likelihood of survival or minimal probability of survival. Mitchell and Dale [51] revealed that gaining HCP agreement on the recognition of end-of-life is a key obstacle to the advance care planning (ACP) process. In a study by Jongaramraung et al. [49], an end-of-life diagnosis was based on the consideration of ‘2Cs’; the Clinical symptoms of patients who failed to thrive with continued medical treatment (including deteriorating diseases), and a Consultation with other medical specialists, such as neurologists, urologists, and endocrinologists. Indeed, consultation with other medical specialists is necessary for children with complex metabolic and neurodegenerative diseases which may create challenges in recognising end-of-life [51]. The different approaches to recognising end-of-life can challenge the continuity of care and delay initiation of end-of-life care.
Shared decision-making with parent(s) at the end of the child’s lifeShared decision-making was considered an important element in the provision of end-of-life care. Yet no studies examining this (n = 14) reported any guidance or framework to underpin discussions and decision-making with parents. However, a study in Thailand by aimed to develop palliative care guidelines for doctors and nurses working in PICU in a university hospital [50]. According to this study, family meetings to discuss transitioning to end-of-life care should take place in a private area of the unit, with the conversation emphasising the child’s prognosis and the risk of adverse outcomes.
Discussions about end-of-life care decisions required interprofessional collaboration, [42] following a doctor’s confirmation of a child entering the end-of-life stage. Nurses had the responsibility to coordinate the meeting between HCPs and parents [49] and the discussion of transitioning to end-of-life care was initiated by the treating doctor [53]. Before making end-of-life care decisions, doctors discussed with parents the most appropriate options for their child. The most common options given were life-sustaining treatment (LST) withholding or withdrawing, and maximum therapeutic care [49, 53].
Several studies indicated the involvement of palliative care teams in the end-of-life care discussion. A Taiwanese study [47] concluded that incorporating a palliative care consultation service resulted in higher willingness to consent to withdrawal of LST and decreased PICU care intensity at the end-of-life. Bobillo-Perez et al. [45] examined how end-of-life care is administered when the decision is made to limit life-support in a PICU and assessed the impact of the further involvement of the Palliative Care Unit. Palliative care doctors and intensivists work together in situations where intensive care could facilitate comfort at the end of a patient’s life and enhance the quality of care. Moreover, doctors as participants in the study by Richards et al. [56] described the benefit of a Paediatric Advance Care Team (PACT) that has the capability of developing a trustworthy connection with the patient’s family, providing psychological support, and organising treatment plans that incorporate the family’s values, concerns, and point of views. This aligns with findings from Ramelet et al. [46], who conveyed that early collaboration between a specialised paediatric palliative care team and the ICU team ensure that care delivered to dying children with complex chronic conditions and their families aligns with their needs and values.
Several considerations were identified in shared decision-making with parents. In discussing end-of-life care with children and their families, both nurses and doctors have a responsibility to use effective communication [50]. In addition, HCPs perceived that parents’ comprehension of their child’s prognosis might challenge the decision-making process [52]. HCPs recognised that shared decision-making, incorporating family’s values, and goals in end-of-life decisions required parents or family members to comprehend the likely course of their child’s condition [42, 49].
End-of-life care processesThe elements of end-of-life care processes included care provided during the dying phase, at the time of death, and after the death of the child.
Care provided during the dying phaseSeveral common features of care for children in the dying phase were identified from nine studies, including providing comfort care [42, 48], psychosocial care to children and their families [48, 50], pain management [46, 50, 55], spiritual care [44, 48, 50, 57], continuity of care [38, 42, 50], imminent death care [50], and collecting mementoes [38].
Comfort care was interpreted differently by participants in the studies included in the review, but it was evident that in most cases it included removal of unnecessary interventions. For example, a participant in Rubic et al. [42] stated: “…to leave them on a ventilator, to turn off all inotropic support, maybe to leave some minimal infusion…” [42].
Psychosocial care for children and their families during the dying phase was specifically mentioned in two studies [48, 50]. This included regular assessments of children’s and families’ psychological reactions to illness using standard tools, documentation of information in patient charts, management of psychological problems, symptoms’ reassessment, observations for complications, and referrals to specialised HCPs as needed. Mesukko et al. [50] in their study stated that only nurses could recognise and address the psychosocial needs of children and their families during this stage. In addition, there were no guidelines on how to communicate with children about their end-of-life care, and the provision of psychosocial support relied on the understanding of individual nurses.
Some studies focused on pain management, as a core part of end-of-life care [46, 50, 55]. However, there was variation in how HCPs conceptualised, recognised and responded to pain experienced by children. It was evident that pain and other distressing symptoms were frequently disregarded, especially by doctors [50]. Although nurses appeared to be attentive to patients’ pain, by for example utilising standardised instruments, doctors were dubious of pain scores recorded by nurses and preferred to make their own conclusions about children’s pain levels. Pain medications were frequently prescribed and given to children at the end of their lives, with Ramelet et al. [46] reporting them given to 42% of dying children in the last four weeks of their life. In addition, careful consideration was given to titrating pain medication based on age and other factors to ensure personalised comfort [55].
Spiritual care was considered by healthcare professionals [44, 48, 50, 57]. Interestingly, the papers reporting on spirituality as a focus of care for children and their families in the end-of-life phase in the PICU were from Saudi Arabia [44] and Thailand [48, 50, 57]. Healthcare participants in the Mutair et al. [44] study highlighted the significance of comprehending and preparing for the religious and cultural needs of families before and following the death of a child [44]. Different approaches were reported in relation to spiritual care and in most cases HCPs considered the religion of the patient and their family to provide individualised care that would alleviate their suffering [57]. For example, involving a priest or monk to organise the ritual of making merit (Thailand) [48], and reciting Qur’an and utilising Zamzam water (Saudi Arabia) [44]. Bloomer et al. [38] point out nurses’ efforts to create normalcy amidst the sadness and grief of a child’s mortality in PICUs and NICUs such as respecting the child as a person, creating opportunities for family involvement/connection, and collecting mementoes.
Care provided at the time of deathThree papers reported on the care provided at the time of the child’s death. When the child dies, HCPs assist parents to say goodbye to their child [36], preserve important mementoes of the child, spend time with their child in a private setting and perform cultural and religious rituals [50]. Mutair et al. [44] specifically described certain rituals that were followed when the child dies within the Muslim context, for example orientating the child’s body towards Mecca and placing the child’s hands together to replicate praying in Islam.
Care provided after deathOnly two papers raised matters on the care provided after the child’s death. Grunauer et al. [43] within their study incorporating 34 PICUs from 18 countries, discovered that the availability of appropriate services to support family grief and bereavement was greater in high income countries (HICs) than in low income countries (LICs). Moreover, this international multicentre study reported a statistically significant correlation between the country income level and the availability and quality of grief and bereavement care (GBC) for PICU patients, their families, and HCPs, meaning that the higher the income of the country, the higher the provision of GBC.
Mesukko et al. [50] described components that should be considered in providing bereavement care for parents/family members and healthcare professionals. This included helping parents come to terms with the reality of their loss, offering condolences to grieving parents or family members by attending memorial services and connecting families with other parents who have encountered a similar loss, self-help organisations, or professional counselling or bereavement services. The authors also suggested bereavement care for healthcare professionals, including peer support, group debriefings, psychological and spiritual counselling, and educational programs [50].
Comments (0)