
Remember me
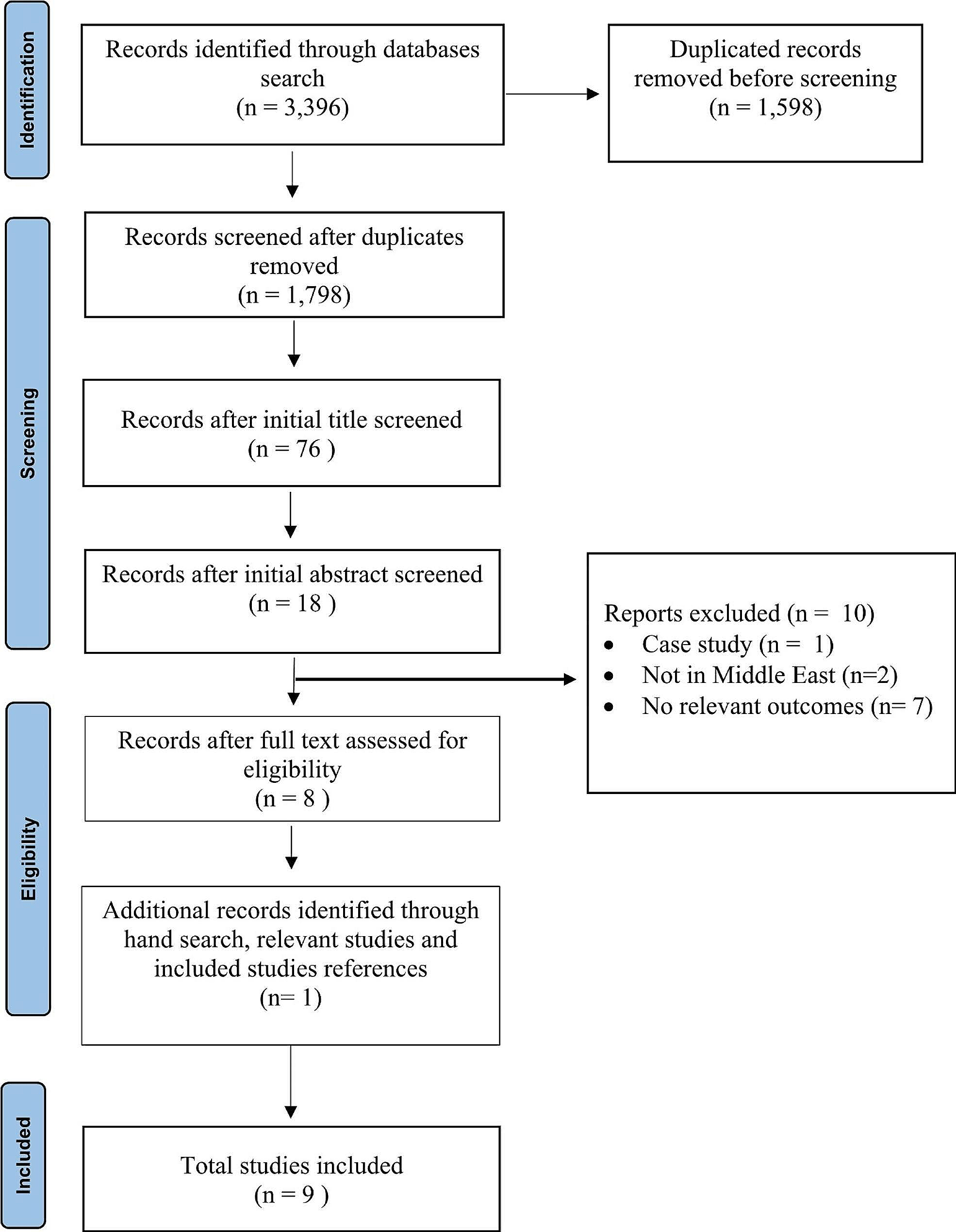

Utilizing a random grouping methodology, all patients were divided into an observation group and a control group at a 1:1 ratio. This study involved 150 advanced cancer patients who received hospice care at our hospital from January 2020 to December 2023. The participants were assigned to either the control group or the treatment group through the random number table method. No statistically significant differences were observed in the general information between the groups (P > 0.05). The control group (n = 75) received standard care, while the treatment group (n = 75) received integrated palliative care in addition to the control group's regimen, which included pain management, psychological support, humanistic care, family involvement, and other interventions.
Inclusion criteria: (1) Condition assessment: patients must have irreversible diseases, such as advanced cancer or chronic organ failure. (2) Examination indicators: the trend and comprehensive evaluation of the patient's recent laboratory and imaging results, indicating the degree of acute progression, metastasis, and short-term condition deterioration. (3) Expected survival: patients should have an anticipated survival time of less than 6 months or shorter survival expectations. (4) Medical ethics indicators: participation and informed consent must be independently provided by the family or the patient. (5) Estimated survival of at least a month.
Exclusion criteria: (1) Patients with non-terminal diseases: those with non-terminal tumors are excluded from hospice care. (2) Patients undergoing active treatment: individuals still receiving active treatment for their primary disease, such as radiotherapy or surgery, are excluded. (3) Patients with severe neurological or communication disorders: these patients may not fully comprehend the philosophy and services of hospice care or effectively communicate their wishes and needs. (4) Patients who are unwilling recipients of hospice care: if the patient or their family expresses resistance or uncertainty regarding hospice care, they may not be suitable candidates for this service. (5) Dying patients or patients unable to complete the study or care plan in a timely manner: individuals with severe violent tendencies, psychiatric disorders, or other conditions that could hinder the implementation of hospice services will be excluded. Experiments were approved by the Ethics Committee of Nanjing First Hospital and were conducted in compliance with the Helsinki Declaration. (6) Patient data will not be collected and analyzed if they cannot complete integrated palliative care due to death.
MethodsThis research employed a mixed-methods approach, integrating both qualitative and quantitative methodologies. A specialized assessment team was established, comprising physicians, nurses, psychological counselors, social workers, and other relevant professionals, to evaluate physical, emotional, and social functioning, along with additional indicators utilizing the EORTC QLQ-C30 scale [10]. Mental health status was also evaluated, with anxiety and depression levels quantified through the GAD-7 (Generalized Anxiety Disorder Scale) and PHQ-9 (Patient Health Questionnaire-9) [11, 12]. Furthermore, a tailored family satisfaction survey was administered to gauge family members' contentment and support regarding the patient care process. Interviews and focus group discussions were conducted to gain insights into the experiences and emotions of both patients and their families, facilitating qualitative data analysis. The research adhered strictly to ethical guidelines, ensuring the confidentiality of participants. Experiments were approved by the Ethics Committee of Nanjing First Hospital and were conducted in compliance with the Helsinki Declaration. Informed consent was obtained from all participants before they participated in this study.
In the control group, standard nursing care protocols were implemented, which included routine health education, addressing patients' negative emotions, nutritional and medication guidance, monitoring vital signs and condition changes, and providing timely, targeted interventions for any abnormalities.
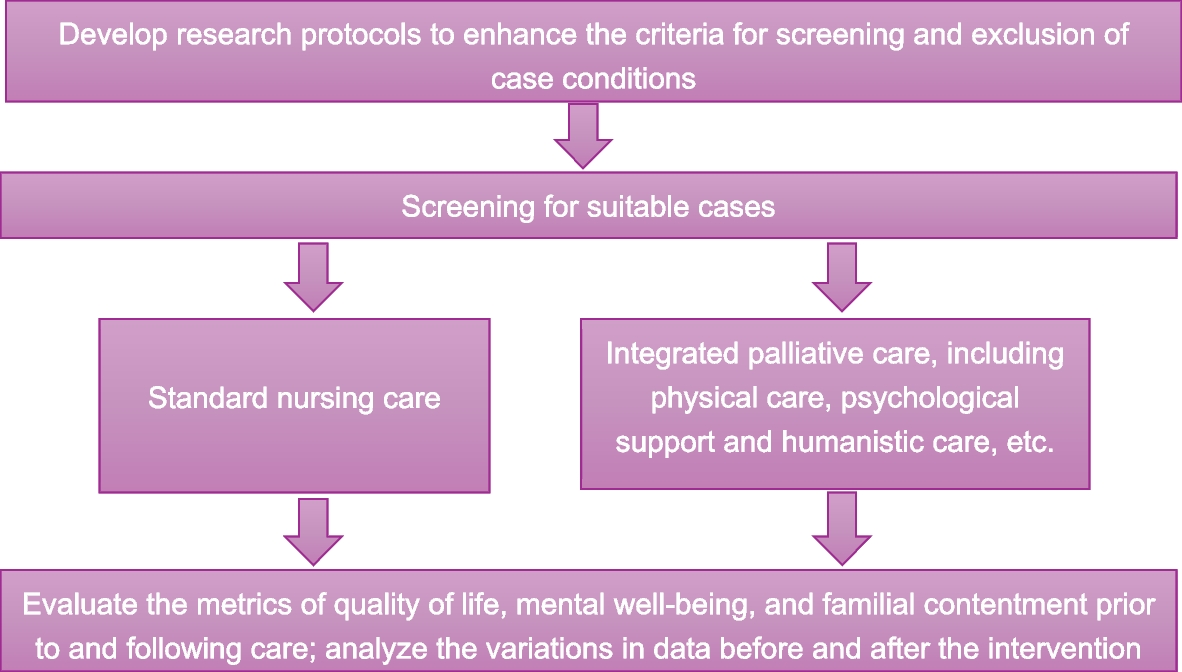
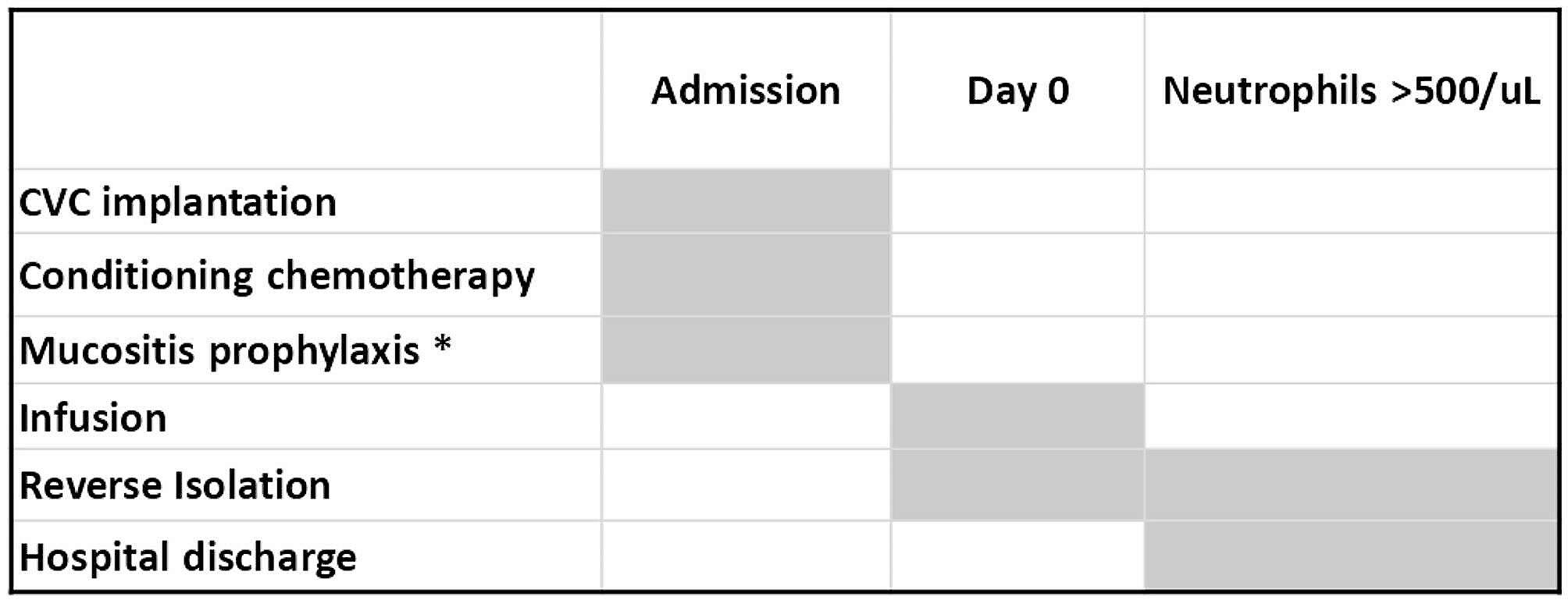
The treatment group received integrated palliative care in addition to the standard care provided to the control group. This included pain management, psychological support, compassionate care, and family involvement, among other strategies: (1) Physical care involved managing pain based on its characteristics—nature, location, intensity, duration, and episodic patterns—selecting appropriate pharmacological and non-pharmacological interventions such as music therapy, massage, and relaxation techniques. Continuous pain assessment was conducted to monitor pain control, allowing for timely adjustments to the analgesic regimen to maintain pain levels within an acceptable range. Daily personal care was provided, guiding patients to find comfortable positions, ensuring airway patency, maintaining oral hygiene, attending to skin care, and offering dietary support aligned with patients' preferences, thereby balancing pain management with overall life care. (2) Psychological support focused on emotional and spiritual comfort, employing empathy, reassurance, and encouragement to communicate with patients and stabilize their emotional state. Techniques such as cognitive behavioral therapy, supportive psychotherapy, and music therapy were utilized to provide psychological guidance, assisting patients in adjusting their mindset and positively confronting their circumstances. When patients' physical conditions allowed, efforts were made to fulfill their reasonable wishes and desires, such as family reunions and completing unfinished tasks, thereby enhancing their sense of life meaning and alleviating feelings of regret and anxiety. (3) Humanistic care involves honoring the patient's rights to autonomy, privacy, and dignity, ensuring that all nursing actions are grounded in a profound respect for the patient's preferences. This is achieved through compassionate and transparent communication, which not only conveys medical information but also prioritizes listening to the patients' emotions and needs, fostering a nurturing and empathetic environment. It is essential to equip family members with pertinent information regarding the illness, offer emotional support, and provide training in caregiving skills, enabling them to comprehend the patient's condition and actively participate in shared decision-making to deliver optimal care. Following the patient's passing, it is important to attend to the body respectfully and allow the family and the deceased the opportunity for a final farewell. Additionally, offering essential grief counseling and support is crucial to assist the family during this challenging period (Fig. 1).
Fig. 1 Observation indicators
Observation indicators(1) Comparative analysis of patients' quality of life assessments across groups, where quality of life encompasses physical, emotional, and social functioning; a higher score indicates a better quality of life. (2) Evaluation of mental health status across groups, with higher GAD-7 and PHQ-9 scores reflecting increased severity of negative emotional states in patients. (3) Assessment of family satisfaction and support across groups, where higher scores in family satisfaction and support indicate more favorable assessment outcomes.
Statistical analysisData were statistically analyzed using SPSS 19.0, with categorical data presented as n (%), employing chi-square and rank-sum tests; continuous data, such as quality of life metrics, were expressed as (mean ± standard deviation), utilizing t-tests. Statistical significance was determined at P < 0.05.
Comments (0)