
Remember me
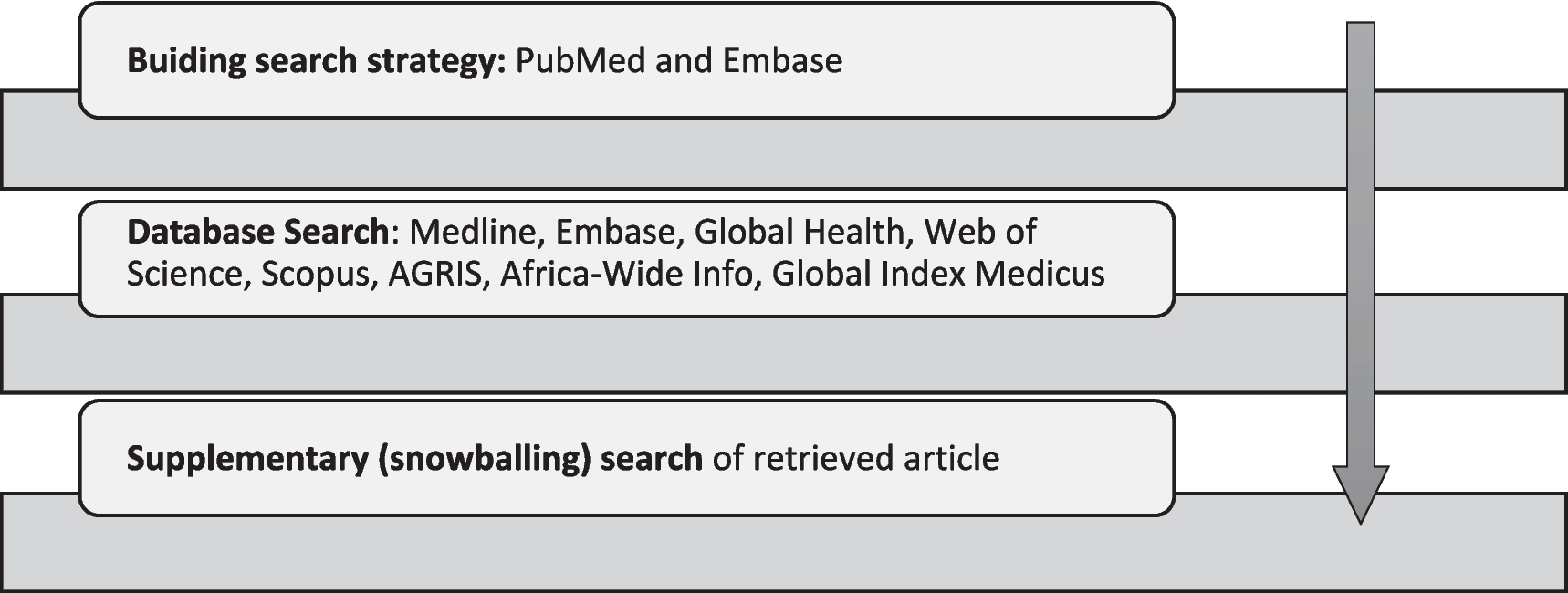
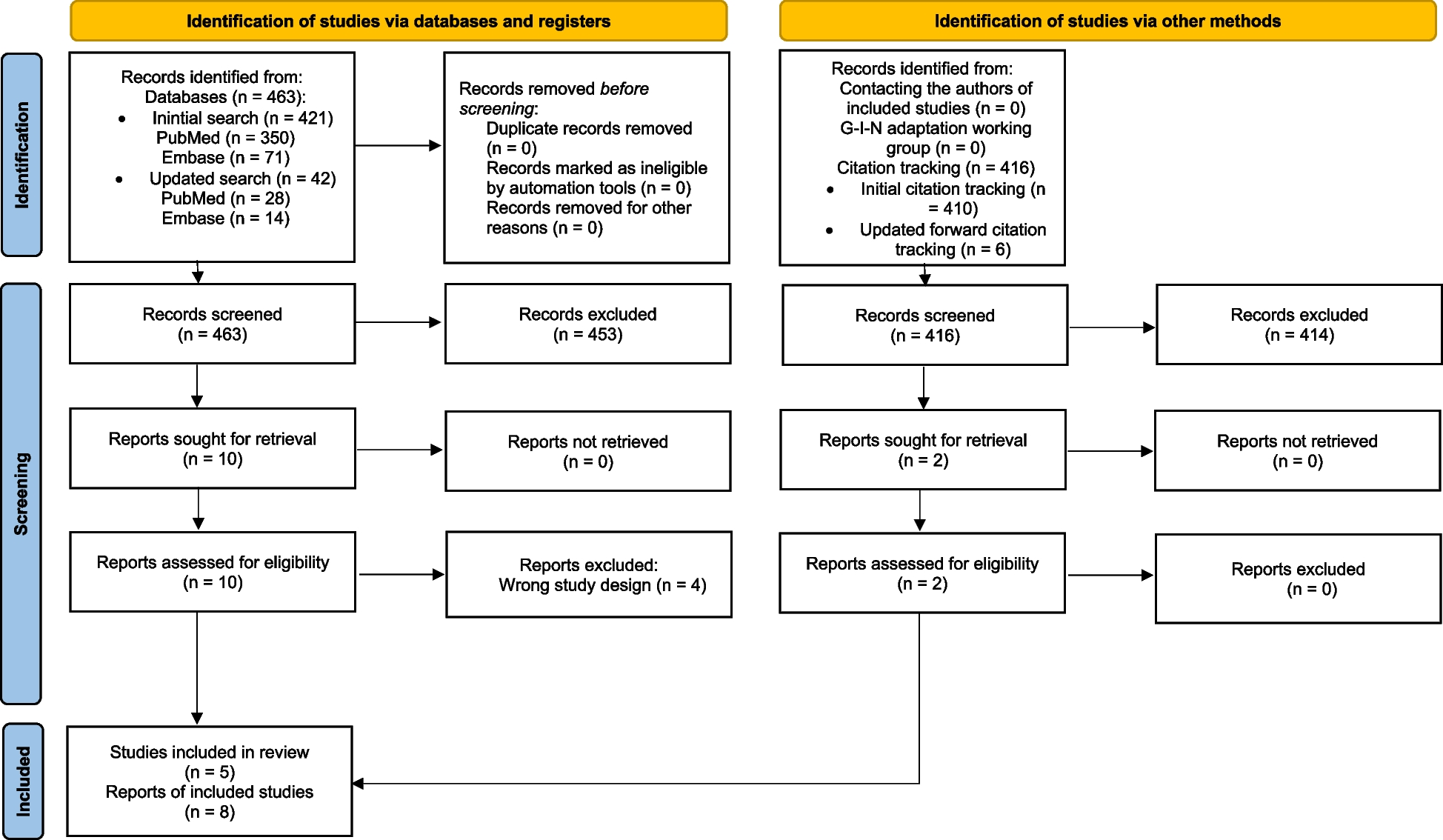
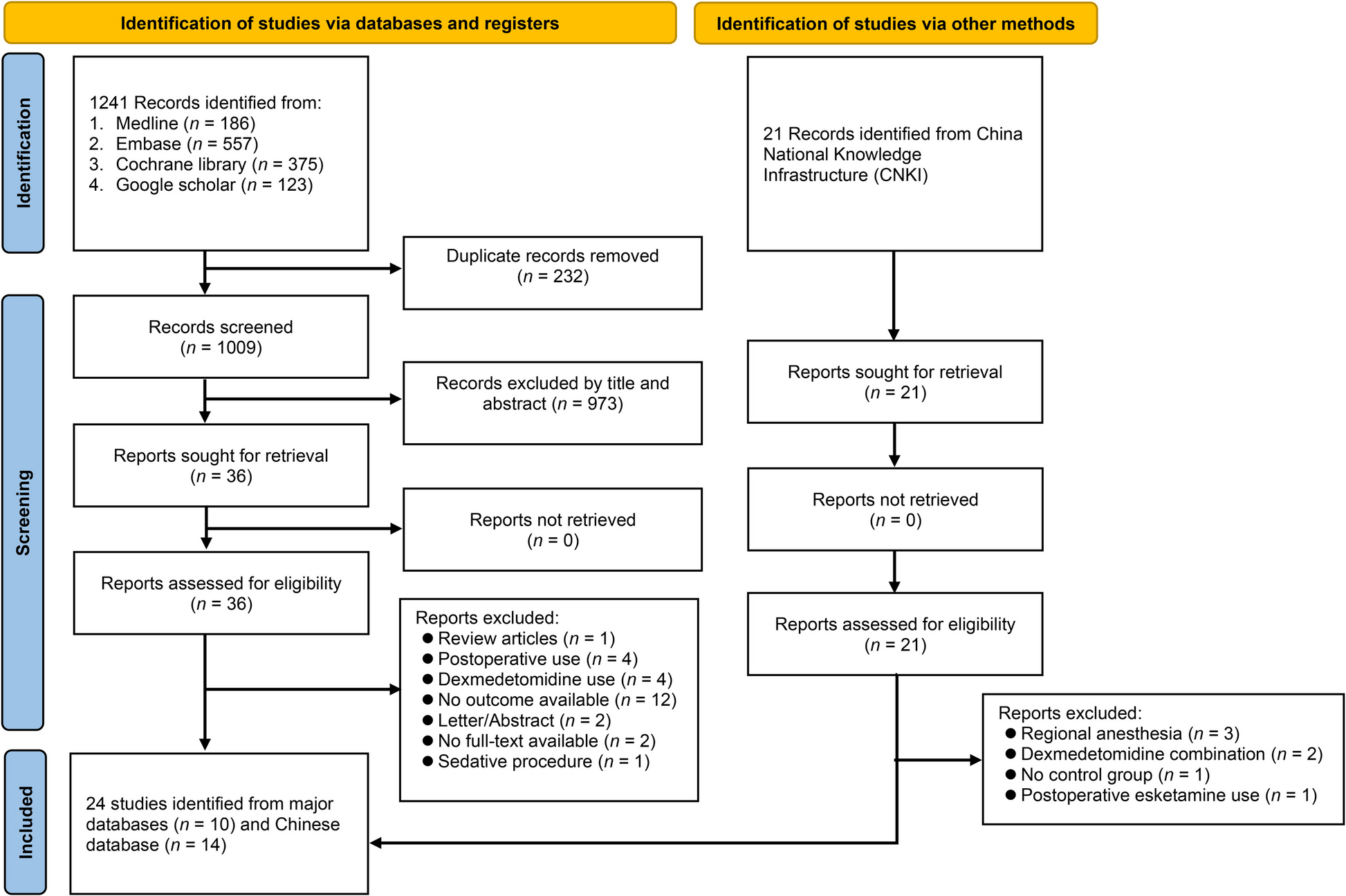
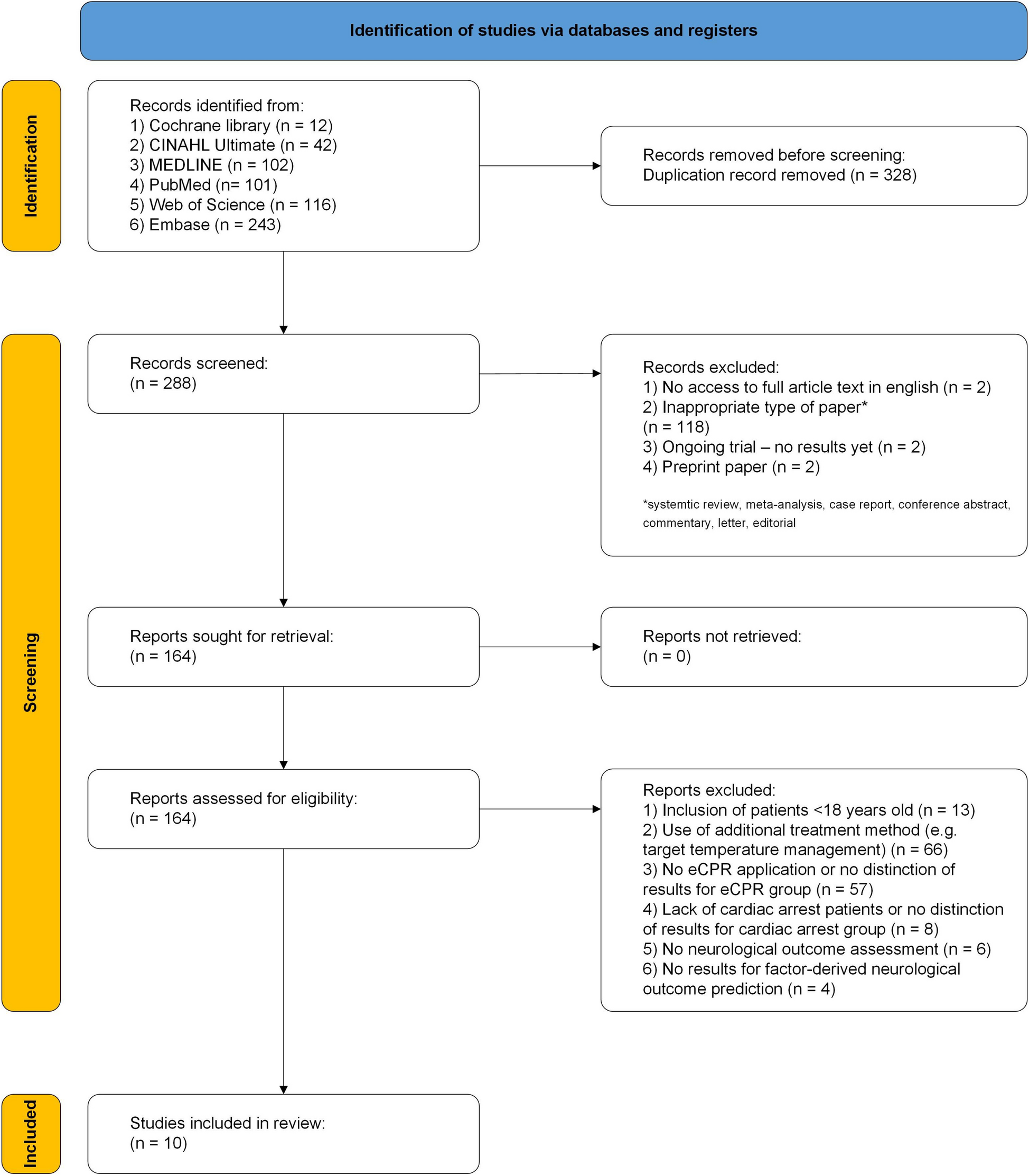
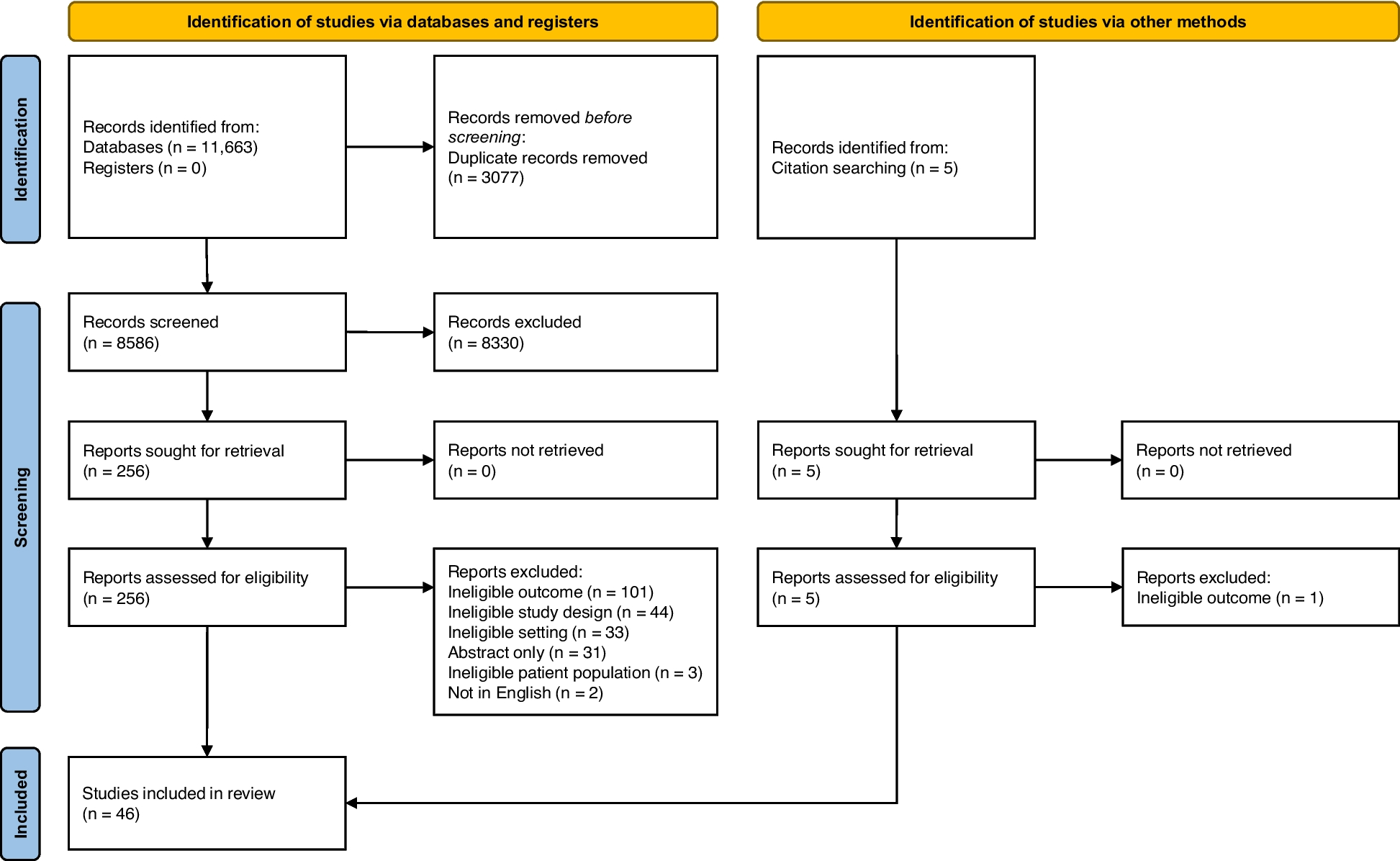
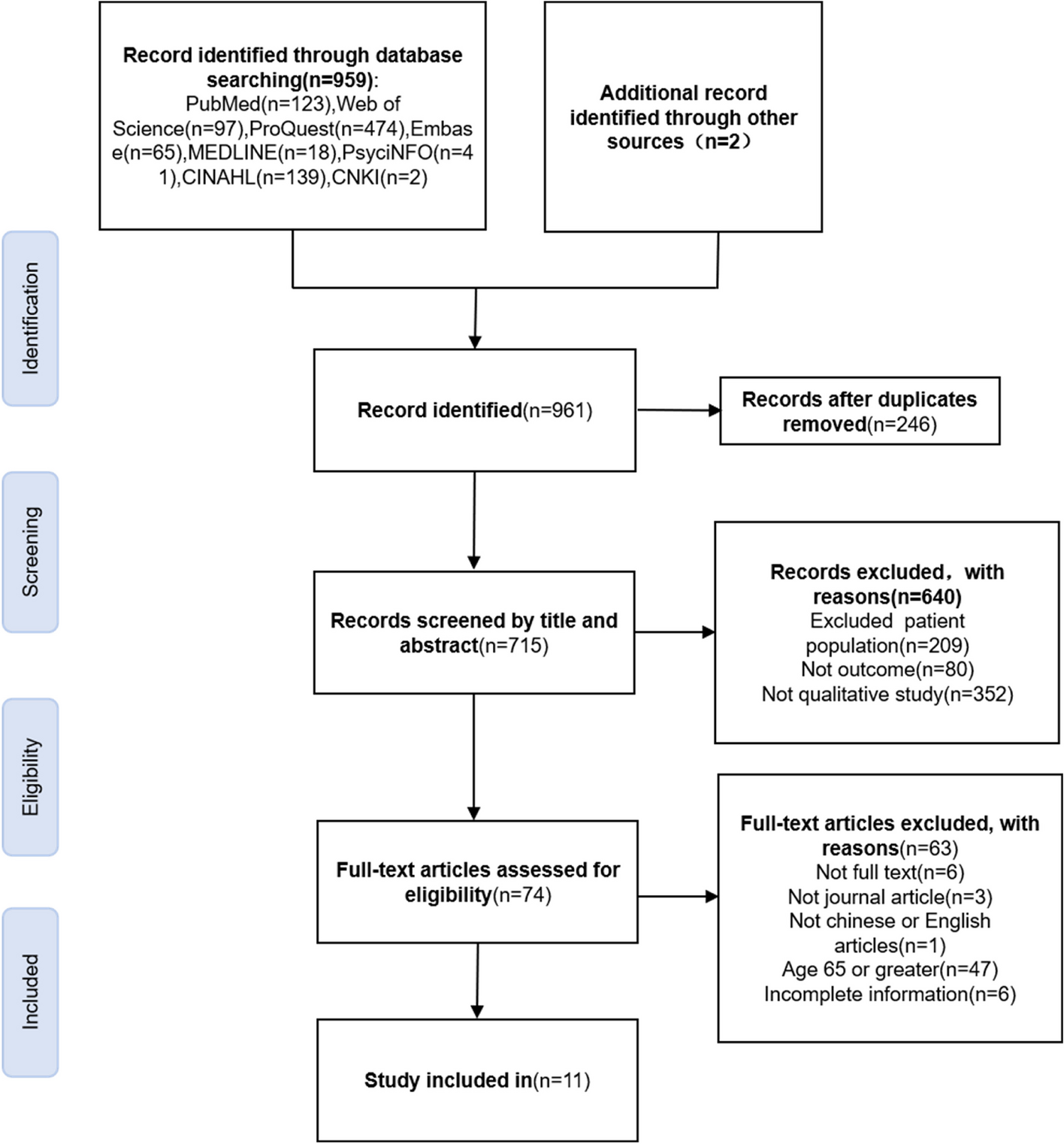
Eight hundred forty-seven records were found in the database search. After the removal of duplicates, 675 records were screened. Following the screening of titles and abstracts of identified articles, 16 articles were included as appropriate for the aim of this systematic review. After the full-text screening, 7 articles which were considered eligible according to inclusion and exclusion criteria, were finally included for qualitative analysis [22, 25,26,27,28,29,30]. Nine records might appear to meet the inclusion criteria, but after full-text screening was finally excluded due to the following reasons: in vitro studies (3 articles); test group was cell aggregates (2 articles); non-English study (1 article); conference proceedings (2 articles) and duplicate study (1 article). The PRISMA flow diagram for the search study utilized in this systematic review is presented in Fig. 1.
Fig. 1
PRISMA flow diagram for identifying eligible studies
Study quality assessmentFor assessment of the risk of bias within individual studies, we used SYRCLE’s Risk of Bias tool. The outcomes of risk of bias assessments are summarized in Table 1 and Fig. 2. All studies are at low risk of bias but certain domains were not reported by some or all of the studies. According to the SYRCLE´s Risk of Bias (RoB) tool, 70 entries were obtained from the ten relevant signaling questions. Of them, 39 of the entries revealed a low RoB, 31 an unclear RoB, and no entry revealed a high RoB. Overall, five of the seven studies (71.4%) that were examined provided evidence that randomization was carried out. They only mentioned a random sequence generation but failed to report which randomization method was applied. All of the animal studies indicated that the subjects' baseline characteristics, including age, sex, and body weight, were matching. In Item 3, all the studies were considered to have an unclear RoB because they did not report any allocation concealment. All the studies were determined as unclear for random housing, investigator blinding, and random outcome assessment from knowledge of which intervention each animal received in Items 4, 5, and 6, respectively. Blinding of outcome assessors was applied in 85.7% (6/7) of studies. Regarding the attrition bias, all the studies had low RoB for incomplete outcome data in Item 8. All the studies were determined as unclear for selective reporting and other biases.
Table 1 Risk of bias summary: review authorssment.e studies.ondary injury processes and functiincluded study according to SYRCLEry: review authorssmFig. 2
The results of the risk of bias assessment
Characteristics of included studiesThe main characteristics of eligible studies are presented in Table 2. Five studies worked with Sprague–Dawley (SD) rats, one with Fischer 344 rats, and one with C57BL/6 mice. Complete transection (six studies) and compression (one study) were the two modes of modeling used. The spinal cord injury segments were located at T10 (five studies), T9 (one study), and T6–7 (one study). Among the included studies, the sample sizes ranged from 18 to 60. The follow-up duration in most of the studies lasted 8 weeks from the stem cell sheet implantation. Two studies ended after 60 days from the surgery, and another study after 7 weeks. The types of stem cells included stem cells from human exfoliated deciduous teeth (SHED) (two studies), adipose-derived mesenchymal stem cells (ADSCs) (one study), and bone marrow mesenchymal stem cells (BMSCs) (four studies). The transplantation types included four allogeneic and three xenogeneic studies.
Table 2 Summary of articles included in the systematic reviewLocomotor function recoveryDetailed characteristics of outcomes of the included studies were summarized in Table 3. In almost all included studies the application of stem cell sheets in SCI rat models led to a significant increase in the values of BBB score (or result of grip strength test) compared with no-treated SCI rats, which indicates marked improvement of locomotor function.
Table 3 Summary of main outcomes and conclusions of the included studiesCompared to untreated and directly intramedullary injected BMSC treatment after SCI, the implantation of BMSC sheets showed significant improvement in motor function based on BBB scores (p < 0.01 for all comparisons). Moreover, BMSC sheets achieved more significant motor improvement within 1 week after implantation compared to the intramedullary injection group and the control group, while the intramedullary injection group did not show significant recovery until 6 weeks after transplantation (mean 11.50 ± 0.60 points for the BMSC sheets group, 9.18 ± 0.76 points for the intramedullary injection group, 6.99 ± 0.72 points for the control group) [28]. The BBB score results from another study indicated that BMSC sheets can also improve motor function after SCI, with significant differences observed compared to the control group starting from the 4th week after transplantation (mean 5.25 ± 0.14 points for the BMSC sheets group, 3.00 ± 0.29 points for the control group, p < 0.05 for all comparisons) [30].
Li et al. also demonstrated a significant improvement in motor function with BMSC sheets compared to the control group (mean 7.73 ± 1.28 points for the NC-overexpressing BMSC group, mean 3.22 ± 0.71 points for the control group, p < 0.0001). Furthermore, their study revealed that overexpressing the NGF gene in BMSC sheets using lentiviral technology led to further enhancement of motor function compared to the NC-overexpressing BMSC group (mean 9.40 ± 0.90 points for the NGF-overexpressing BMSC group, p < 0.0001) [27]. Moreover, culturing human umbilical vein endothelial cells (HUVECs) on the surface of BMSC sheets enabled the introduction of microvessels into the stem cell sheets, thereby providing increased blood, oxygen, and nutrient supply to the cells present in neural tissue. This approach demonstrated a significantly superior effect on the recovery of motor function compared to other comparison groups (mean 9.58 ± 2.53 points for the BMSC + HUVEC group, mean 7.52 ± 2.29 points for the BMSC group, mean 7.01 ± 2.01 points for the control group, p < 0.05 for all comparisons) [29].
In addition to using BMSCs for cell sheet culture, it has been shown that cell sheets formed from SHED, which exhibit stronger neurotropic properties, can also enhance motor function after SCI. Mi et al. demonstrated that by co-culturing SHED sheets with homogenate proteins of the spinal cord, SHED cells were induced to differentiate into neural cells before being transplanted into rats with spinal cord injury. On the 60th day post-SCI, a significantly greater recovery of motor function was observed compared to the control group and SHED suspension group (mean 8.20 ± 0.84 points for the hp-SHED group, mean 6.40 ± 1.14 points for the SHED suspension group, mean 3.20 ± 0.84 points for the control group, p < 0.001 for all comparisons). Similarly, SHED cells induced to differentiate with homogenate proteins of the spinal cord exhibited higher maximum grip strength values compared to all other study groups (mean 235.40 ± 27.93 g for the hp-SHED group, mean 173.00 ± 16.70 g for the SHED suspension group, mean 107.80 ± 14.81 g for the control group, p < 0.05 for all comparisons) [25]. Another study showed that co-culturing stem cell sheets formed from neuro-induced SHED with undifferentiated SHED resulted in more significant improvements in motor function scores in the grip strength test compared to single-type SHED cell sheets and the control group (mean 11.60 ± 1.14 points for the SHED + iSHED group, mean 7.60 ± 1.14 points for the SHED group, mean 2.60 ± 0.89 points for the control group, p < 0.001 for all comparisons) [22].
Sensory function recoveryThe recovery of motor function was consistently accompanied by sensory function recovery. Three studies evaluated sensory function recovery using the Von Frey test [22, 25, 28]. Among them, two studies utilized a complete spinal cord transection model, which often resulted in severe sensory dysfunction due to the complete disruption of spinal cord conduction pathways [22, 25]. In this model, rats typically exhibited significant sensory deficits. The third study employed a spinal cord compression model, commonly used for studying neuropathic pain after spinal cord injury [28]. In this model, impairments in ion channel function, excessive inflammatory mediators, and disruption of the descending antinociceptive serotonergic tract can lead to abnormalities in afferent nerve sensitization, causing severe neuropathic pain (hyperalgesia) in rats 1 week after modeling.
In the complete spinal cord transection model, SHED + iSHED sheets significantly increased the number and proportion of rats showing sensory function recovery compared to the control group, promoting improvements in sensory function (at a total of 20 days after surgery, 100% rats recovered sensation in the SHED + iSHED group, 80% rats recovered sensation in the SHED group, only 20% rats recovered sensation in the control group) [22], hp-SHED sheets also produced similar results, with 80% of rats recovering sensation in the hp-SHED group compared to 40% in the SHED suspension group and 20% in the control group (a total of 30 days after surgery) [25].
In the spinal cord compression model, direct intramedullary injection of BMSCs did not show improvements in neuropathic pain thresholds (hyperalgesia) within a 7-week observation period. However, significant improvement in pain hypersensitivity was observed in rats transplanted with BMSC sheets at 4 weeks post-transplantation, and this improvement became more pronounced over time (mean 48.60 ± 12.60 g for the BMSC sheets group, 3.19 ± 1.30 g for the intramedullary injection group, 1.60 ± 0.59 g for the control group, p < 0.01 for all comparisons) [28].
Axonal regenerationThe functional recovery observed in the included studies was consistent with the changes observed in the histological analysis of the injury site. In most studies, the use of stem cell sheets showed significantly better results compared to the control group in terms of reduction in atrophy and presence of cavities at the injury site [26,27,28,29]. Additionally, Nissl staining results from a mouse model of complete spinal cord transection injury revealed a significant increase in Nissl bodies in mice after implantation of BMSC sheets, and a further significant increase in the number of Nissl bodies was observed after overexpression of the NGF gene in BMSC sheets.
Immunofluorescence and immunohistochemical staining demonstrated that implanted stem cell sheets promoted axonal regeneration and neuronal differentiation in the complete transection model. In most included studies, rats with implanted stem cell sheets exhibited the highest numbers of cells labeled with specific markers for neurons or axons (such as NF [22, 25], NeuN [25], Tuj-1 [27, 29, 30], GAP43 [27, 30], β-tubulin III [26], and CGRP [22, 25]) compared to the control group, indicating successful neural and axonal regeneration at the injury site. However, in the compression model, Yamazaki et al. found that the expression of FR was significantly higher compared to the negative control group but showed no significant difference compared to the BMSC cell suspension intramedullary injection group. Additionally, the study also found no difference in the staining of CGRP among all groups.
Both in the complete transection and compression model, stem cell sheets significantly promoted the regeneration of myelinated axons and inhibited the formation of glial scar. Two studies demonstrated that the area stained by luxol fast blue (LFB) was significantly larger in the groups treated with stem cell sheets compared to other comparison groups [28, 29]. Furthermore, in all studies examining the presence of myelin basic protein (MBP) using immunofluorescence, a greater number of MBP-positive myelin sheath structures were observed in animals implanted with stem cell sheets compared to other groups [22, 25], and a more pronounced linear staining pattern of MBP was also observed [29]. In studies evaluating glial scar formation using glial fibrillary acidic protein (GFAP) staining, the animals treated with stem cell sheets consistently exhibited significantly fewer GFAP-positive cells compared to other groups [22, 25, 26, 28,29,30]. Additionally, inducing neural differentiation of SHED sheets [22, 25] and introducing HUVECs into BSMC sheets further inhibited glial scar formation beyond the original stem cell sheets [29].
Adverse effectsTwo studies reported no immunotoxicity to major organs such as the heart, liver, spleen, lung, and kidney [22, 25]. One study observed a lower inflammatory reaction after implanting the stem cell sheet into the subcutaneous pocket, indicating either no or low immunoreactivity to the host animal [29]. However, other trials did not provide information regarding the safety of the intervention.
Comments (0)