
Remember me
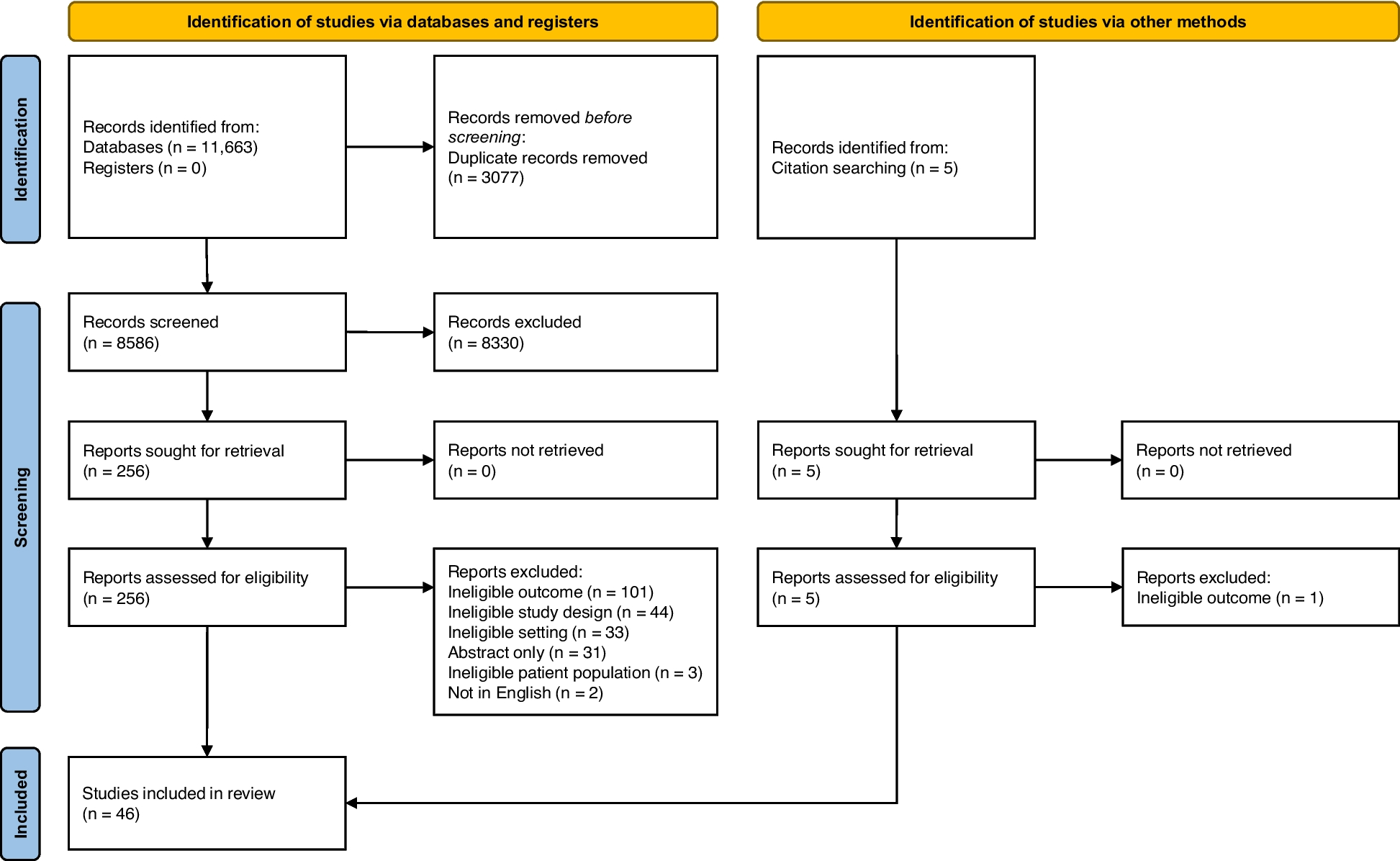
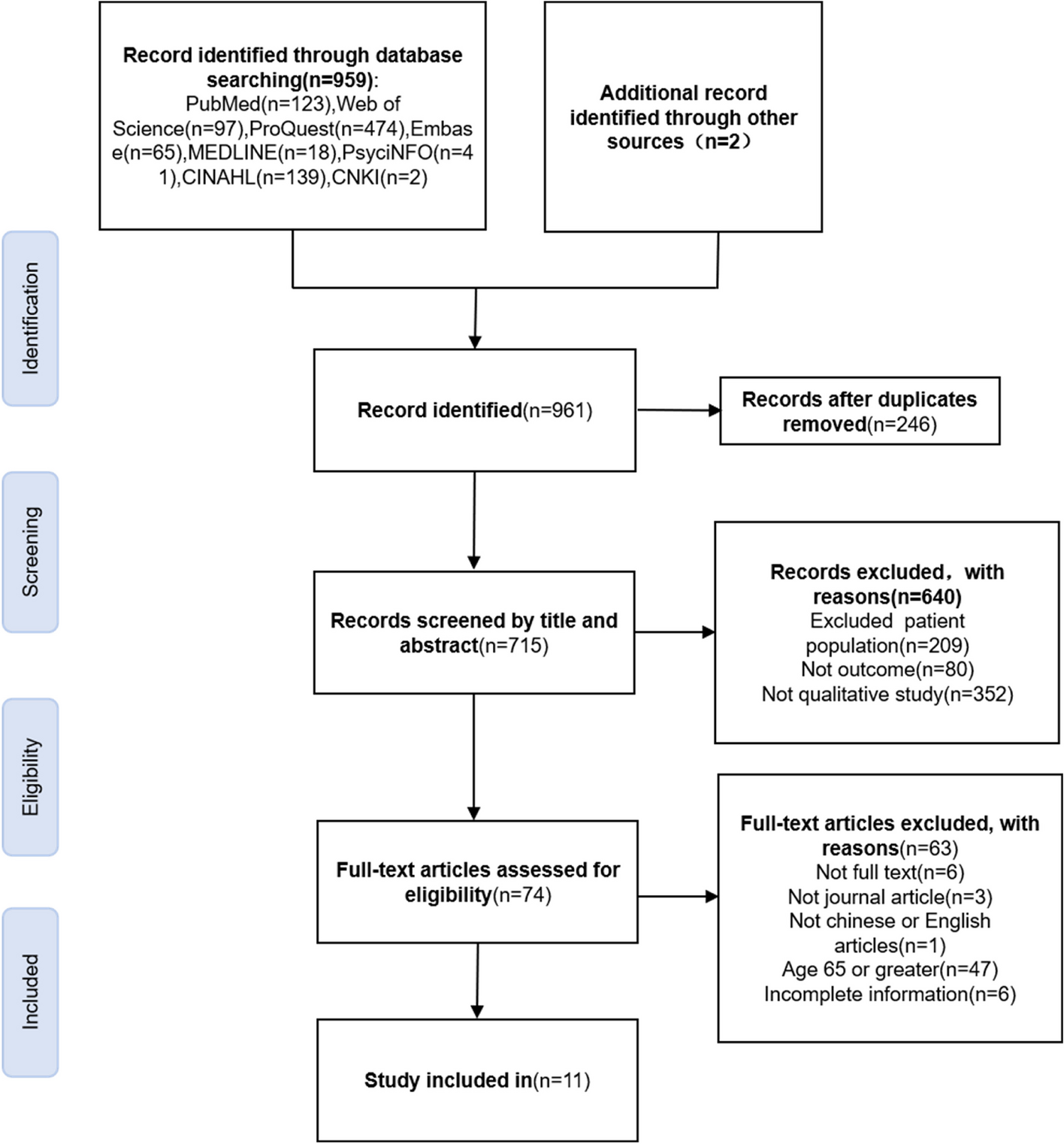
A total of 961 articles were retrieved and 11 were included after removing duplicates and articles that did not meet the inclusion criteria, as shown in Fig. 1. The 11 included studies involved 250 young and middle-aged hypertensive patients aged 18–64 years. Two studies included only females [20, 21], and one study included only males [22]. The included studies involved six countries, including two in Malaysia [23, 24], four in America [21, 22, 25, 26], two in China [27, 28], one in Brazil [29], one in Denmark [30] and one in Bangladesh [20]. Eight of the included studies used interviews [20,21,22,23,24, 29], two used focus groups [25, 26] and one was not specified [30].
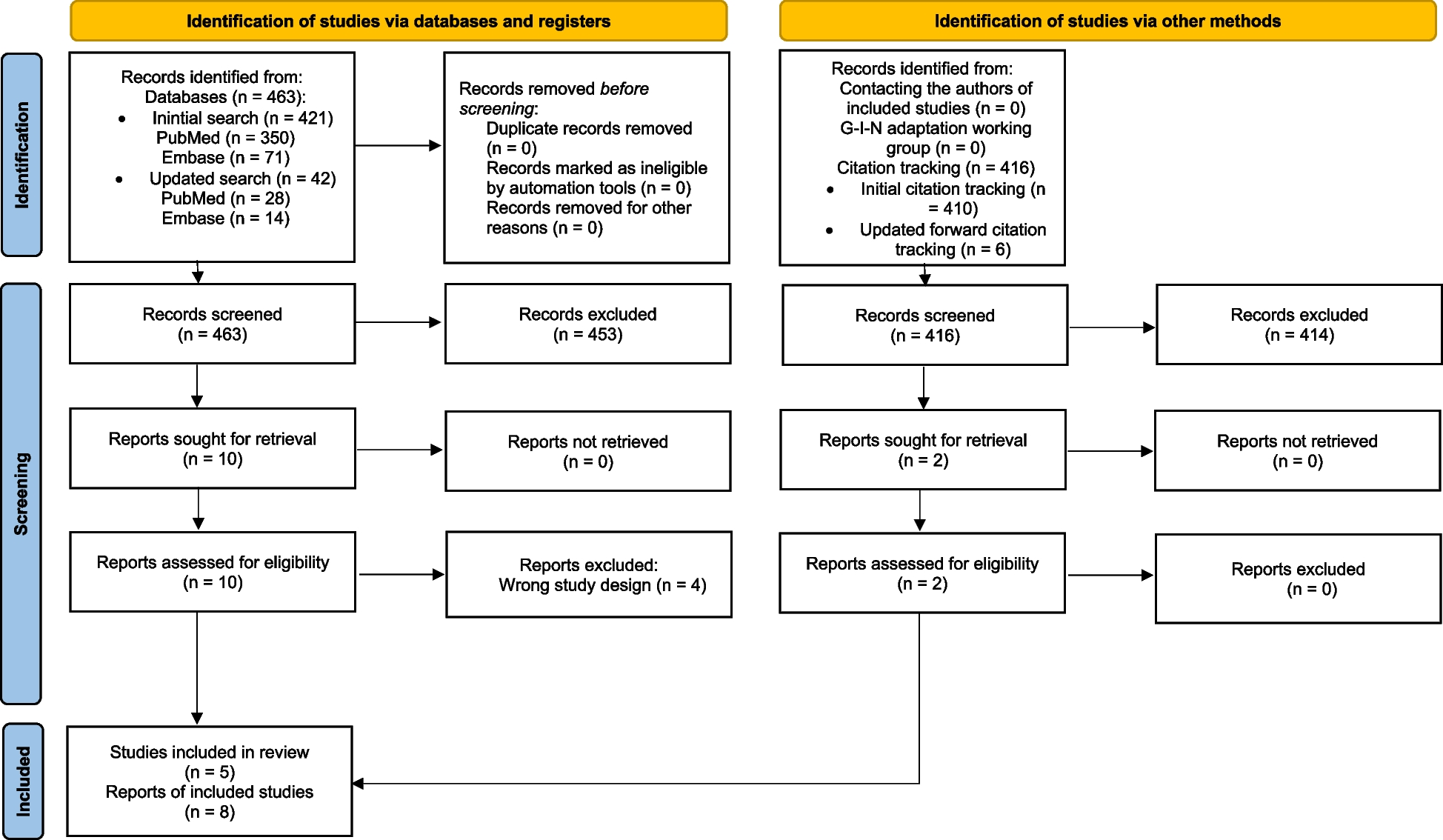
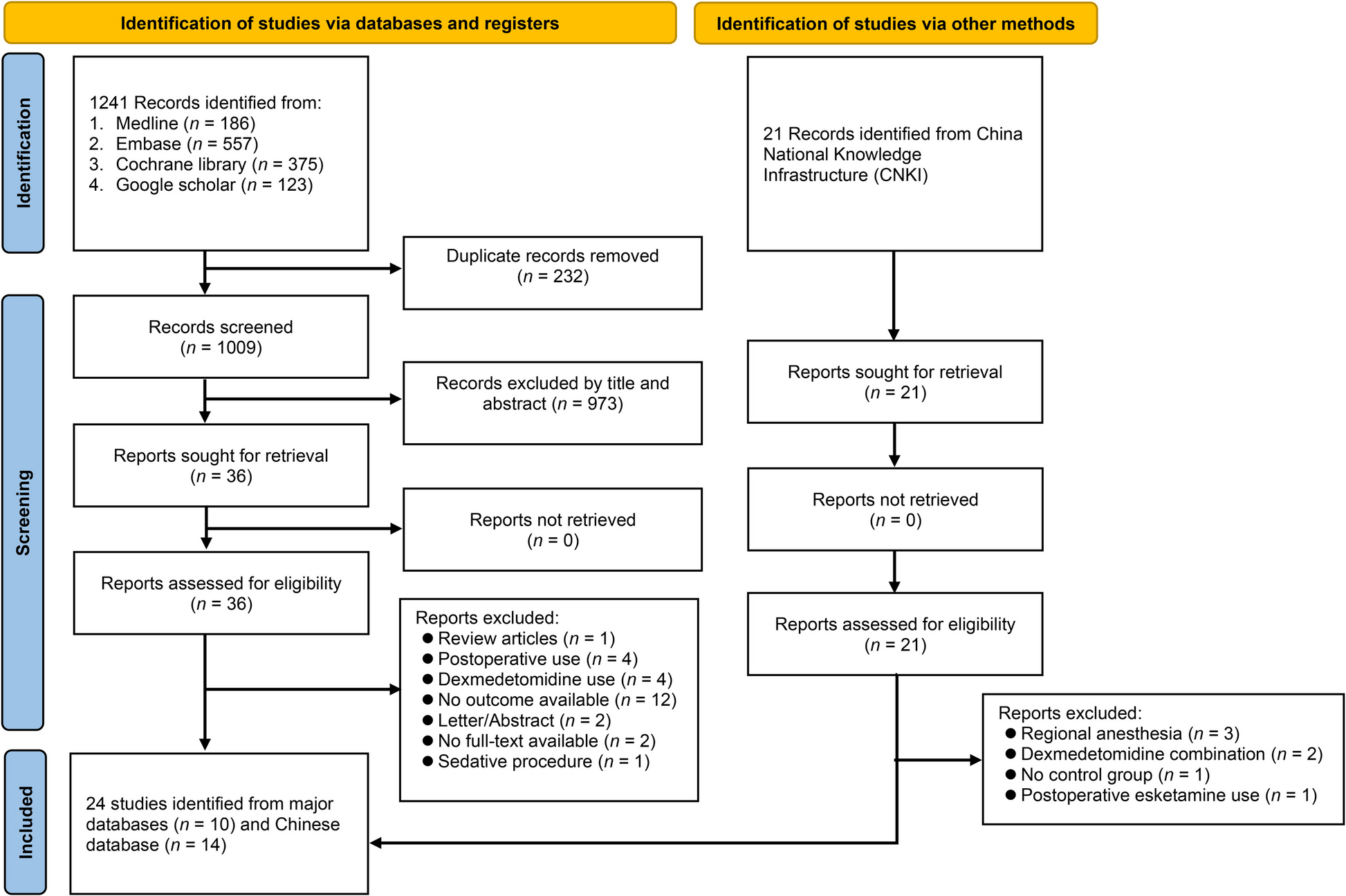
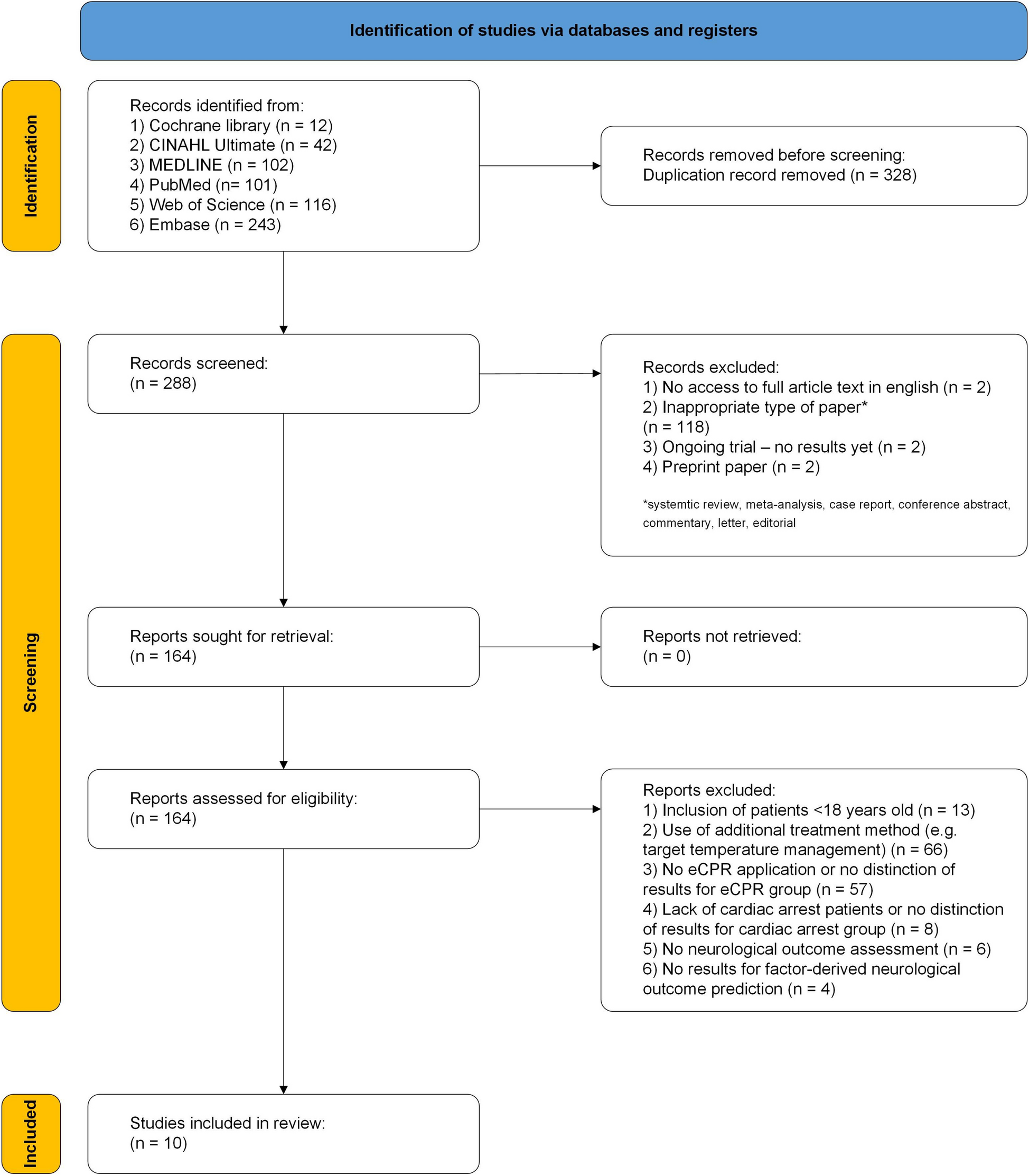
Fig. 1
Literature screening flow chart
Of the data analysis methods, four used thematic analysis [20,21,22, 26], two used Colaizzi’s seven-step analysis, two used content analysis [24, 25], one used descriptive-reductive-interpretive schema [23, 30], one used interpretive phenomenological analysis [25] and one used grounded theory analysis [29]. Subjects included in the study and study characteristics are shown in Table 1. We used the JBI Qualitative Research Inventory to assess the quality of the 11 included articles, and the results showed that all selected articles were of medium and high quality, as shown in Table 2.
Table 1 Extraction of original research dataTable 2 Quality appraisal of studies using JBI Checklist for Qualitative ResearchSynthetic resultsWe have identified four themes with ten sub-themes: Poor disease recognition (low disease perception, fuzzy disease knowledge); Barriers to doctor-patient interactions (short communication time, unmet knowledge needs, incomplete guidance for disease management); Living in a hostile environment (heavy workload, lack of companionship, ignorance of families); Expectations for a healthy body (responsibility of family roles, witness the cruelty of illness), as shown in Table 3.
Table 3 Themes and sub-themesPoor disease recognitionLow disease perceptionLow disease perception is mainly reflected in poor medication adherence and difficult lifestyle changes. Poor medication adherence is mainly reflected in patients’ own minimisation of the disease and resistance to taking medication. Medication was not a ‘priority’ [23]. In young and middle-aged patients, clinical symptoms were not obvious [20, 22, 25, 30], and therefore most patients in the study cited ‘busy schedules’ and ‘missing’ medication as reasons for not taking their medication regularly [22, 25, 23, 26], and believed that medication was not a ‘priority’ [23]. Some patients are so confident about their health that they believe they ‘don’t need’ medication [23, 25] or that they can ‘control’ the disease [30, 23]. The difficulty of lifestyle change is reflected in the fact that the vast majority of patients ‘know’ that a healthy lifestyle is good for the disease, but are unable to do so [20, 22, 23, 25, 27, 28]. Daily activities such as diet [20, 21, 27], exercise [27] and blood pressure measurement [20, 23] were only marginally improved when there was a change in disease or clinical symptoms. We also found that exercise was a ‘more acceptable goal’ for young and middle-aged patients compared to dietary changes [23, 25, 29]. Lifestyle changes require a long period of adherence, but most patients adhere to management only briefly at the time of diagnosis and often abandon it later due to laziness or lack of motivation, and they want to have clear goals and be monitored [20, 25, 23, 27, 28]. In addition, home blood pressure monitoring is not encouraging, as patients support the benefits of regular blood pressure monitoring for disease control, but most continue to monitor their blood pressure only when they feel ‘unwell’or have symptoms of hypertension [20, 23].
Fuzzy disease knowledgeMost young and middle-aged patients understand some basic knowledge about blood pressure management and what conditions may ‘trigger’ the disease, and will consciously avoid them in their daily life. However, due to the lack of accurate knowledge about the disease, they often follow the wrong advice or are unable to manage the disease effectively [20,21,22,23, 25,26,27,28, 30]. Some patients lack knowledge about the complications of hypertension and the medications used to treat it, leading to minimisation of the condition and resistance to the medications used to treat it [20, 25, 27,28,29, 23]. As one patient put it, ‘I don’t know the dangers of high blood pressure and targeted, individualised medication [27]’.
Barriers to doctor-patient interactionsShort communication timeMost patients want to provide their doctors with complete information about themselves and receive appropriate responses, but due to the high volume of outpatient visits, communication time is too short, resulting in inadequate access to information for patients [21,22,23,24,25, 27,28,29]. As one patient put it, ‘I don’t tell my doctors about my problems with taking my medication. They usually say something like, “OK, just take your medicine, you can go now”. It’s not even five minutes compared to the long wait [23]’.
Unmet knowledge needsThey are very concerned about the side effects of therapeutic drugs, and the side effects of drugs are one of the reasons why they are resistant to taking drugs, and they hope that their doctors can inform them about the side effects of drugs and how to deal with them when they occur, but they are rarely satisfied with the process of medical consultation [22, 24, 25, 27, 28, 23, 26, 29]. In addition, due to a lack of knowledge about antihypertensive drugs, they are very resistant to prescription drugs, especially in Asia, and most of them try to use other treatments (e.g. traditional medicines) instead of prescription drug therapy [20, 21,
Comments (0)