
Remember me
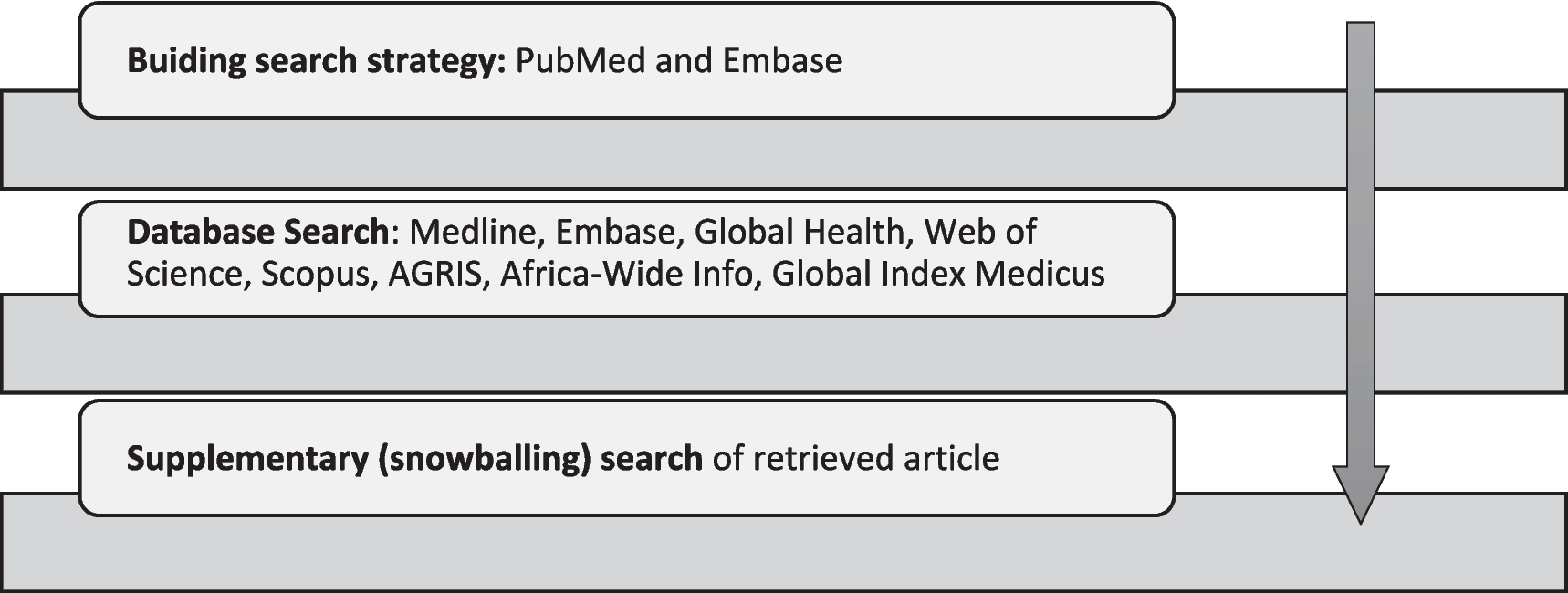
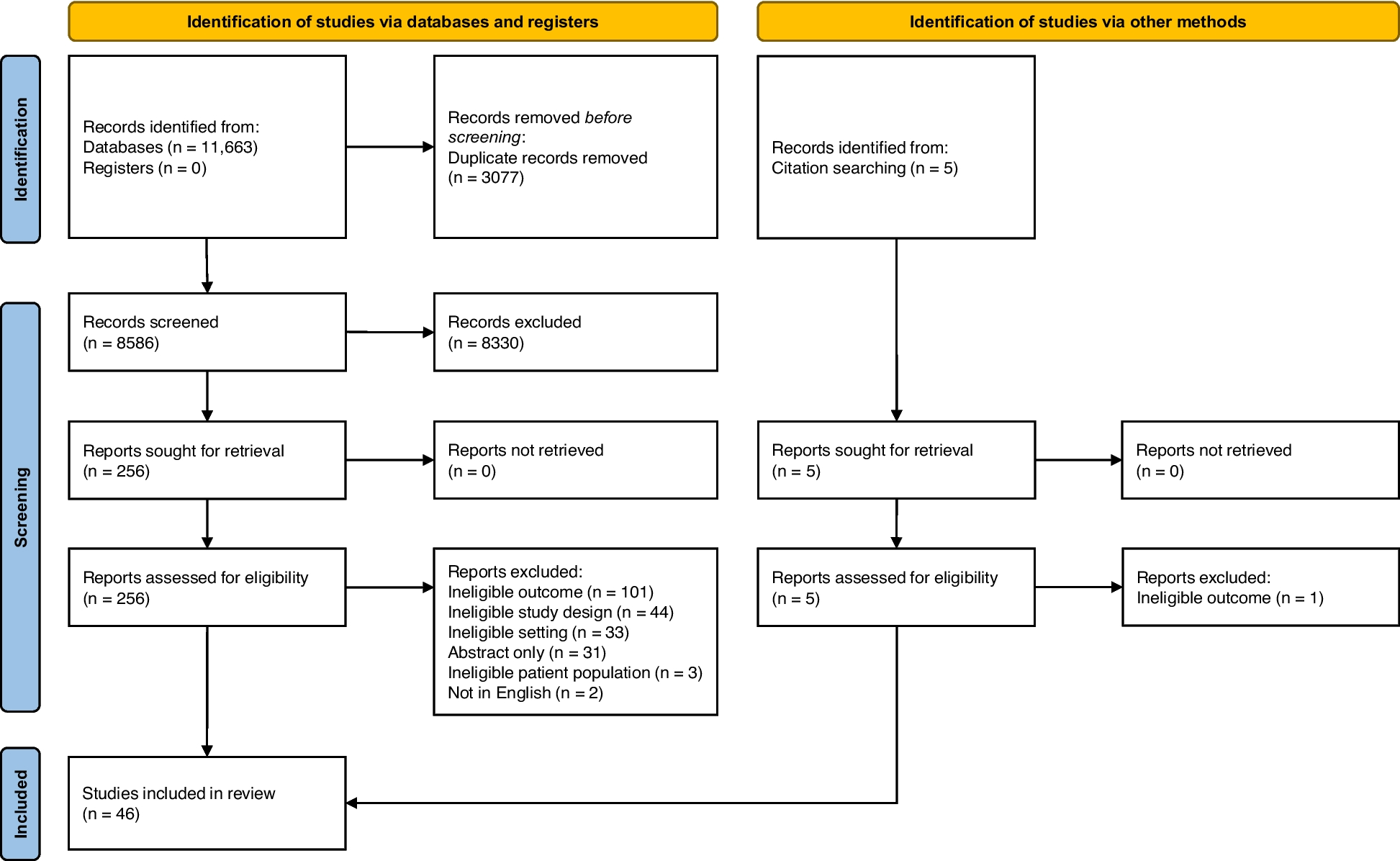
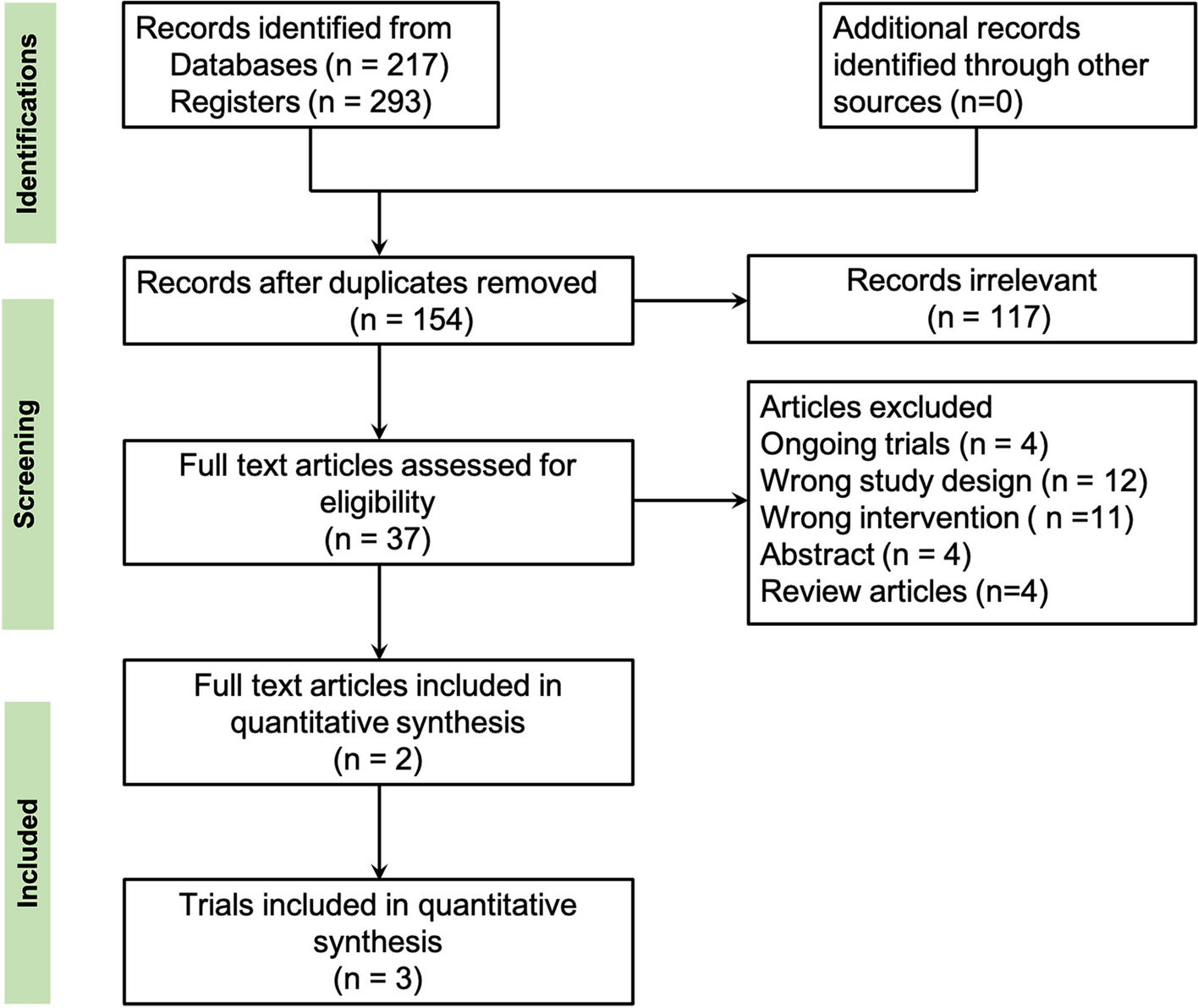
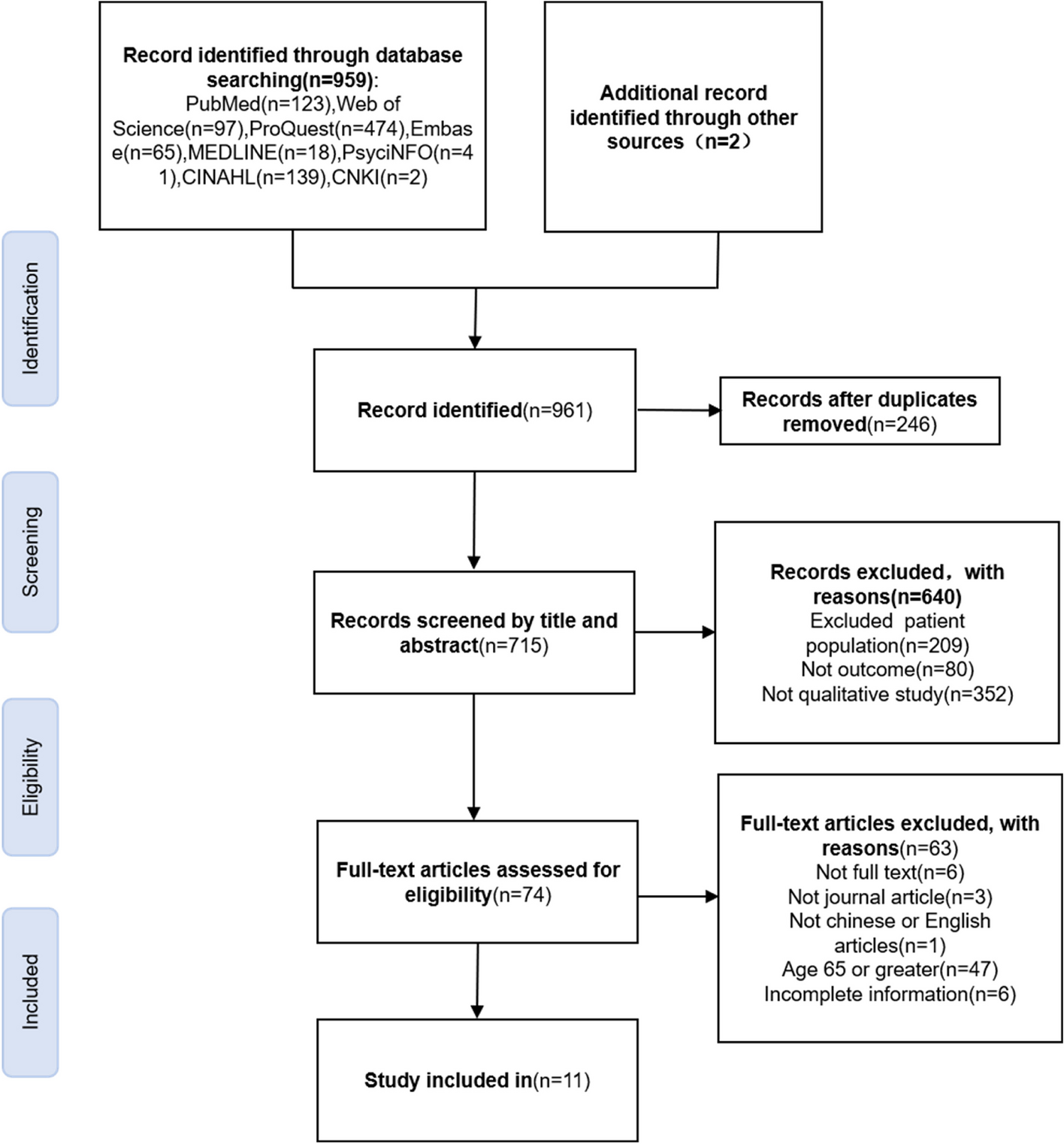
A systematic search was conducted, resulting in the identification of 217 records from multiple databases. Additionally, 293 records were obtained from trial registration sources. After removing duplicate records and screening the titles and abstracts, a total of 117 records were excluded based on predetermined criteria. Subsequently, the full-text articles of the remaining records underwent a thorough assessment, ultimately leading to the inclusion of three trials reported in two studies for the meta-analysis (Fig. 1).
Fig. 1
Flow diagram of article selection for the meta-analysis
Study characteristicsThree trials, involving a total of 830 participants with vitiligo from nine countries, were included in the analysis. Detailed inclusion and exclusion criteria for patient selection can be found in Supplementary Table S2. Table 1 and Supplementary Table S3 provide a summary of the characteristics of the included trials. Of the participants, 388 (46.7%) were female, while 442 (53.3%) were male, with the mean age ranging from 38.9 to 48.3 years and the mean duration of vitiligo ranging from 9.7 to 15.9 years. Among the participants, 11 (1.3%) had segmental vitiligo, while the remaining 819 (98.7%) had non-segmental vitiligo. The treatment interventions included the use of a vehicle and four different doses of topical ruxolitinib cream: 0.15% (once a day), 0.5% (once a day), 1.5% (once a day), and 1.5% (twice a day).
Table 1 List of included trials and baseline characteristicsRisk of bias assessmentThe risk of bias assessment for each domain and the overall level can be found in Supplementary Table S4. Notably, for every outcome reported in the three trials, the risk of bias was determined to be “low.”
Findings on symptomsF-VASI90, F-VASI75, F-VASI50, and F-VASI25Three trials, involving a total of 830 patients, were included in the meta-analysis to assess the effectiveness of ruxolitinib compared to the vehicle by F-VASI90, F-VASI75, F-VASI50, and F-VASI25. The meta-analysis demonstrated a significant increase in the likelihood of participants achieving F-VASI90 (OR 9.61 [95% CI 3.67–25.19]; I2 = 0%; GRADE assessment: moderate certainty), F-VASI75 (OR 4.34 [95% CI 2.67–7.06]; I2 = 0%; GRADE assessment: high certainty), F-VASI50 (OR 4.71 [95% CI 3.24–6.84]; I2 = 0%; GRADE assessment: high certainty), and F-VASI25 (OR 4.74 [95% CI 3.28–6.86]; I2 = 35%; GRADE assessment: high certainty) when compared ruxolitinib to vehicle (Fig. 2; Table 2).
Fig. 2
Ruxolitinib vs vehicle cream on F-VASI90, F-VASI75, F-VASI50, F-VASI25, T-VASI90, T-VASI75, T-VASI50, T-VASI25 and VNS-4 or 5
Table 2 GRADE summary of findings for ruxolitinib versus vehicle cream treatment for vitiligoT-VASI90, T-VASI75, T-VASI50, and T-VASI25Three trials, involving a total of 830 patients, were included in the meta-analysis to assess the effectiveness of ruxolitinib compared to the vehicle by T-VASI90, T-VASI75, T-VASI50, and T-VASI25. The meta-analysis results demonstrated that the use of ruxolitinib did not significantly increase the likelihood of participants achieving T-VASI90 compared to vehicle (OR 1.47 [95% CI 0.24–9.09]; I2 = 0%; GRADE assessment: moderate certainty). The meta-analysis demonstrated a significant increase in the likelihood of participants achieving T-VASI75 (OR 2.78 [95% CI 1.10–7.00]; I2 = 0%; GRADE assessment: moderate certainty), T-VASI50 (OR 4.47 [95% CI 2.52–7.92]; I2 = 0%; GRADE assessment: high certainty), and T-VASI25 (OR 3.45 [95% CI 2.40–4.96]; I2 = 3%; GRADE assessment: high certainty) when compared ruxolitinib to vehicle (Fig. 2; Table 2).
VNS-4 or 5The meta-analysis of two trials, involving a total of 673 patients, demonstrated that the use of ruxolitinib led to a higher proportion of participants achieving VNS-4 or 5 (OR 6.15 [95% CI 3.14–12.05]; I2 = 0%; GRADE assessment: moderate certainty) in comparison to vehicle (Fig. 2; Table 2).
F-VASI and T-VASIThree trials, which included 830 patients, reported the outcome of percentage change from baseline of F-VASI scores. The results showed that ruxolitinib was associated with more lowered percentage change of F-VASI scores from baseline (MD − 32.79 [95% CI − 36.37 to − 29.21]; I2 = 97%; GRADE assessment: moderate certainty) compared to vehicle. Three trials, which included 830 patients, reported the outcome of percentage change from baseline of T-VASI scores. The results showed that ruxolitinib was associated with more lowered percentage change of T-VASI scores from baseline (MD − 20.22 [95% CI − 23.11 to − 17.33]; I2 = 98%; GRADE assessment: moderate certainty) compared to vehicle (Fig. 3; Table 2).
Fig. 3
Ruxolitinib vs vehicle cream on F-VASI, T-VASI, F-BSA, and T-BSA
F-BSA and T-BSATwo trials, which included 673 patients, reported the outcome of percentage change from the baseline of F-BSA scores. The results showed that ruxolitinib was associated with more lowered percentage change of F-BSA scores from baseline (MD − 19.40 [95% CI − 19.91 to − 18.89]; I2 = 0%; GRADE assessment: high certainty) compared to vehicle. Two trials, which included 673 patients, reported the outcome of percentage change from baseline of T-BSA scores. The results showed that ruxolitinib was associated with more lowered percentage change of T-BSA scores from baseline (MD − 10.50 [95% CI, − 13.34 to − 7.67]; I2 = 99%; GRADE assessment: high certainty) compared to vehicle (Fig. 3; Table 2).
Findings on quality of lifeTwo trials, which included 673 patients, reported the outcome of change from baseline DLQI scores. The results showed that ruxolitinib was associated with more lowered change of DLQI scores from baseline (MD − 0.46 [95% CI − 0.73 to − 0.19]; I2 = 95%; GRADE assessment: moderate certainty) compared to vehicle (Supplementary Figure S1; Table 2).
Findings on safetyThree trials, which included 830 patients, reported these outcomes of TEAEs, SAEs, and discontinuation due to AEs. The meta-analysis results indicated that there may not be a significant difference in the occurrence of TEAEs (RR 1.46 [95% CI 0.85–2.49]; I2 = 53%; GRADE assessment: high certainty), SAEs (RR 2.25 [95% CI 0.59–8.67]; I2 = 0%; GRADE assessment: moderate certainty), and discontinuation due to AEs (RR 0.38 [95% CI 0.10–1.48]; I2 = 0%; GRADE assessment: high certainty) between ruxolitinib and vehicle (Supplementary Figure S5; Table 2).
Another analysesSubgroup analyses and assessments of publication bias were not conducted due to the limited number of clinical trials included in the analysis (only three trials) and the fact that all trials were conducted by the same research group, performing subgroup analyses and assessing publication bias may not be appropriate or informative.
Comments (0)