This systematic review was conducted following the Cochrane Handbook for Systematic Reviews of Interventions and reported following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Additional file 1) [15, 16]. We registered the protocol in the International Prospective Register of Systematic Reviews (PROSPERO registration number: CRD42024530305).
Criteria for considering studies for this reviewTypes of studies
The review considered both observational and experimental study designs that provide relevant information regarding the neurological outcomes of patients undergoing eCPR. Inclusion criteria for types of study were observational studies such as cohort studies, case–control studies, and cross-sectional studies that investigate neurological outcomes following eCPR; experimental studies including randomized controlled trials and quasi-experimental studies assessing the neurological outcomes of patients undergoing eCPR; and studies utilizing prospective or retrospective designs. Exclusion criteria for types of study were studies lacking information on neurological outcomes following eCPR; studies with inadequate study design or methodology to assess neurological outcomes effectively; and studies not providing relevant data or outcomes related to eCPR or neurological assessment, case reports, or case series without broader generalizable findings. To address potential overlap in study populations, studies with overlapping datasets were carefully examined. When multiple studies reported on the same cohort, priority was given to the study with the most comprehensive data, the longest follow-up, or the largest sample size. If different studies from the same dataset provided unique or complementary analyses, they were included with a careful notation of their overlap to avoid duplicate patient contributions in pooled analyses.
Types of participants
The review considered studies involving adult patients (both men and women, ≥ 18 years old, and being part of all ethnic groups), who have experienced either in-hospital or out-of-hospital cardiac arrest of any etiology and subsequently underwent eCPR. The ability to predict neurological outcomes based on information gathered from medical history, physical examination, laboratory tests, and/or imaging studies also was evaluated. Exclusion criteria for participants were studies involving patients younger than 18 years of age and studies incorporating concurrent use of additional treatment methods alongside eCPR, such as target temperature management.
Types of interventions
The intervention of interest was eCPR, utilizing ECMO to support lung and/or heart function during cardiac arrest. Specifically, studies examining the neurological outcomes of patients who have undergone eCPR were included.
Types of outcome measures
The pre-specified main outcomes of the review primarily focus on neurological status following eCPR and its predictors. These outcomes were assessed using standardized neurological scales such as the Cerebral Performance Category (CPC), modified Rankin Scale (mRS), or Glasgow Outcome Scale (GOS). Additionally, factors contributing to neurological outcome prediction were examined.
The neurological status was measured and assessed at specific time points post-eCPR, including hospital discharge, 30 days post-resuscitation, or at longer-term follow-up periods such as 90 days or 1 year post-resuscitation. Assessment variables included neurological outcome assessment using standardized scales (CPC, mRS, GOS) and variables related to neurological outcome prediction, such as factors examined (e.g., medical history, physical examination, laboratory tests, imaging studies), time of assessment, examiner, proportion of patients with favorable and unfavorable outcomes, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and cut-off points.
Search methods for identification of studiesElectronic search
The last electronic search was conducted in January 2024. In the searches, the following databases were used: PubMed, MEDLINE, Embase, CINAHL Ultimate, the Cochrane Library, and Web of Science. The search included references that have been published till the end of December 2023. Studies had to be published in English. A list of research terms used for the present review is reported in Additional file 2.
Searching other resources
For non-indexed conference proceedings, the review team searched relevant conference proceedings and websites (e.g., Google Scholar). In addition, the review team hand-searched bibliographies of relevant systematic reviews, narrative reviews, and meta-analyses found, as well as relevant citations in bibliographies of the articles included in the review.
Data collection and analysisSelection of studies
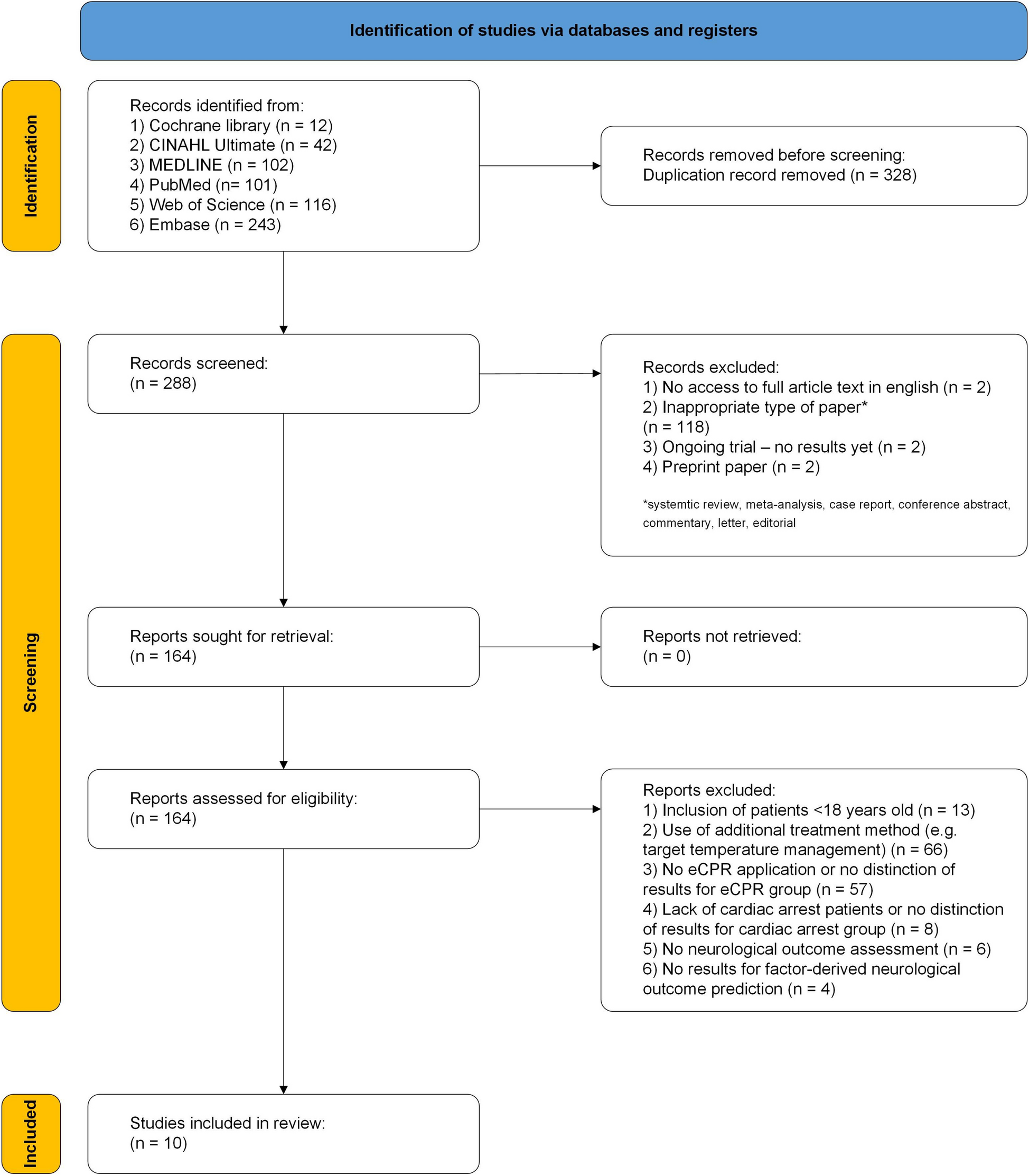
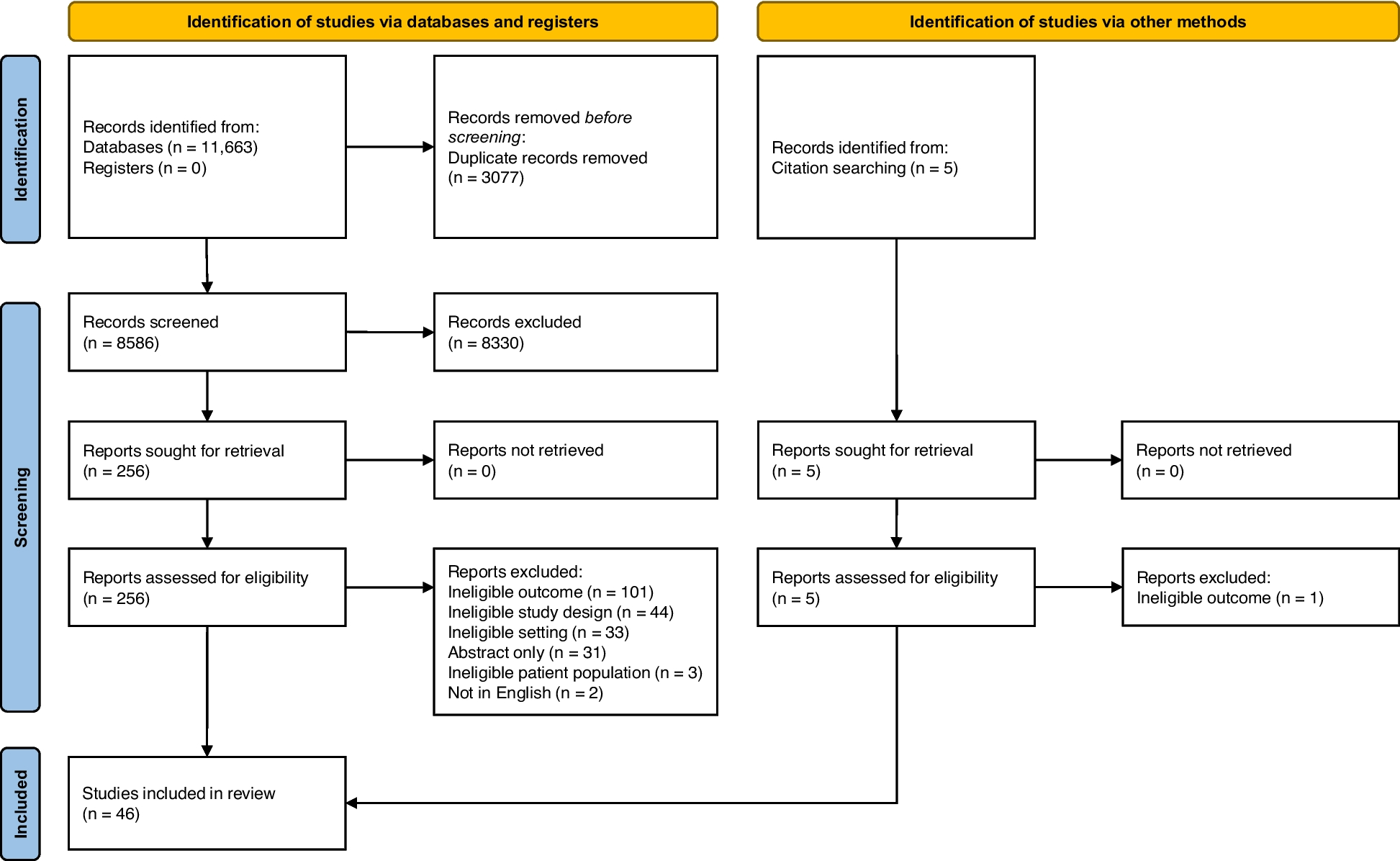
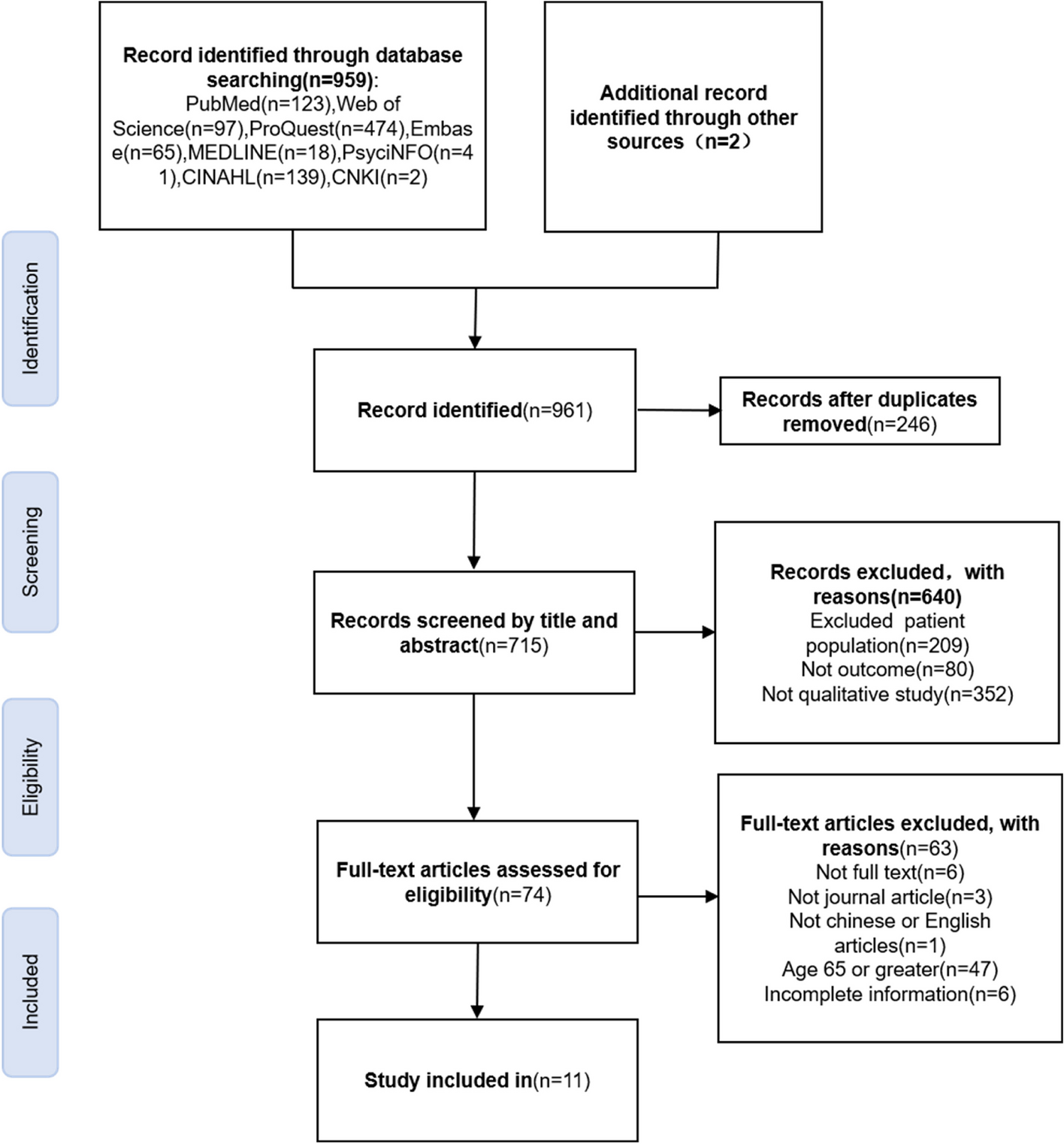
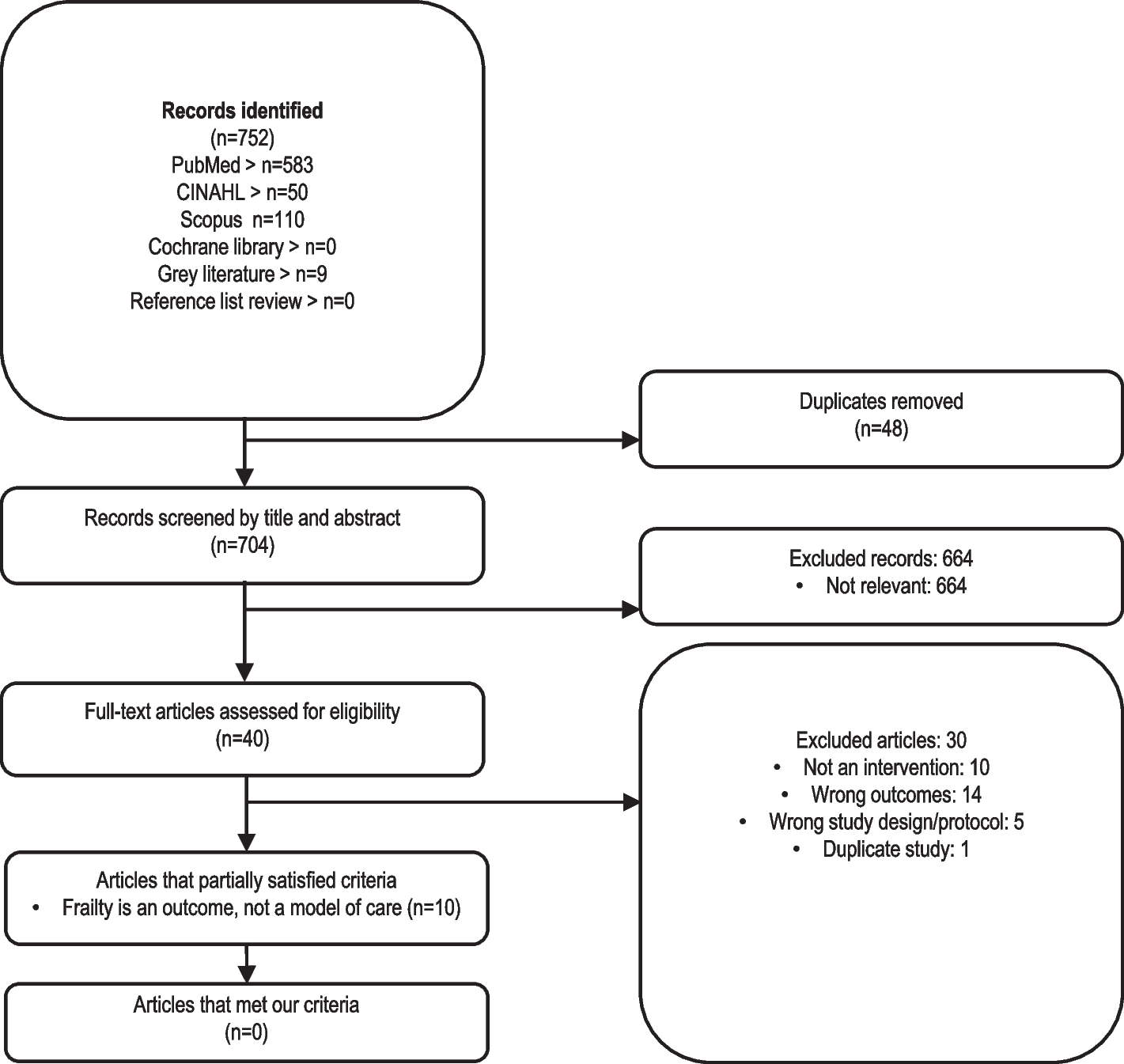
The search resulted in 288 records after removing duplicates. The references were imported into the Excel software spreadsheet to conduct screening by titles and abstracts. First, a random sample of 40 records was independently double-screened by one of the authors to assess inter-rater agreement. The inter-rater agreement was assessed using Cohen’s K was satisfactory, K = 87.5%. Any conflicts and questions related to the eligibility criteria were resolved by discussion with the co-authors before proceeding with the screening. At this stage, two different authors (one being the first author, the rest being distributed among the remaining authors) independently screened a random sample of 60% of the records. The inter-rater agreement with Cohen’s K was good (K = 85%). Questions and conflicts were discussed and resolved among the authors.
Data extraction and management
Any discrepancies between reviewers were resolved through discussion or consultation with a third reviewer. Data quality checks were conducted to ensure accuracy and consistency in recording.
Data was extracted from included studies using a standardized data extraction form. The following data was extracted: author(s), year of publication, country, and study design; inclusion and exclusion criteria; number of patients included in the study; mean age of patients and female-to-male ratio; characteristics of cardiac arrest (location, shockable rhythm); key time intervals (mean no-flow time, mean low-flow time, mean eCPR duration, mean hospital stay duration); outcome measures (survival to eCPR withdrawal, 24-h survival rate, survival-to-discharge rate, 30-day survival rate, mean time of follow-up); neurological outcome assessment details (used scale, time of assessment, examiner, the proportion of patients with favorable and unfavorable outcomes); examined factors for neurological outcome prediction; measures of effect (relative risks, odds ratios, risk differences, number needed to treat); and measures of accuracy (sensitivity, specificity, PPV, NPV).
Assessment of risk of bias in included studies
The risk of bias was assessed using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool, which is specifically designed to evaluate bias in non-randomized studies, including cohort studies, case–control studies, and quasi-experimental designs. This tool provides a structured framework for assessing bias across seven key domains: confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported results. Confounding was evaluated to determine whether other variables might have influenced the observed association between the intervention and outcome. The selection of participants was assessed to ensure appropriate comparability between groups. The classification of interventions was examined to determine whether intervention classification was accurate and free from misclassification bias. Deviations from intended interventions were identified to detect any systematic departures from the intervention protocol that could introduce bias. The extent of missing data was analyzed to assess its potential impact on study results, whereas the measurement of outcomes was evaluated for objectivity and reliability. The selection of reported results was assessed to identify any evidence of selective outcome reporting that might influence study findings.
Each included study was systematically evaluated across these domains, with an emphasis on identifying potential sources of bias that could affect internal validity and overall reliability. Bias assessments were conducted independently by two reviewers to ensure a rigorous and objective evaluation process. Any discrepancies in judgment were resolved through discussion, and when necessary, a third reviewer was consulted to reach a consensus. The overall risk of bias for each study was determined based on the cumulative impact of biases identified across the domains, with studies categorized as having low, moderate, serious, or critical risk of bias according to ROBINS-I criteria. Several challenges were encountered during the assessment process. One common difficulty was distinguishing between confounding and selection bias, particularly in observational studies where baseline differences between intervention and control groups were not always adequately accounted for. To address this, we closely examined the statistical methods used for confounder adjustment, giving preference to studies employing propensity score matching, inverse probability weighting, or multivariable regression models with comprehensive covariate adjustments. Another challenge was the potential for misclassification bias, especially in studies relying on administrative databases or self-reported measures. In such cases, we assessed whether the studies validated their exposure and outcome classifications against objective clinical criteria or independent verification methods.
The handling of missing data presented additional complexity, as many studies lacked explicit descriptions of how missing values were addressed. We classified studies with high rates of missing data and inadequate handling methods (e.g., complete case analysis without justification) as having a higher risk of bias. When studies employed appropriate imputation techniques or sensitivity analyses to account for missing data, the risk of bias was downgraded accordingly.
In cases where studies included overlapping populations, additional steps were taken to prevent duplication of data and ensure the integrity of the analysis. When multiple studies were identified as using the same or substantially overlapping patient cohorts, priority was given to the study with the most comprehensive dataset, longest follow-up, or highest methodological quality. If studies reported different but complementary outcomes from the same population, they were included in a way that minimized redundancy while preserving the breadth of relevant findings. Sensitivity analyses were performed to assess whether the inclusion or exclusion of overlapping studies affected overall conclusions. Decisions regarding the handling of overlapping populations were transparently documented to enhance reproducibility and methodological rigor.
To ensure full transparency, all bias assessments were comprehensively documented (see Additional file 3), including the rationale for each judgment, considerations regarding domain-specific risks, and any uncertainties encountered during the evaluation. Graphical representations of bias distribution across studies were generated using Robvis, allowing for a clearer understanding of potential biases influencing the overall findings of the review.
Measures of treatment effect
The effect measures for the main outcomes, focusing on neurological status following eCPR) and its predictors, included relative risk (RR), odds ratio (OR), risk difference (RD), and number needed to treat (NNT).
RR compared the risk of a neurological outcome (e.g., favorable vs. unfavorable) between patients who underwent eCPR with favorable neurological outcomes and those who did with unfavorable neurological outcomes. OR assessed the odds of a particular neurological outcome (e.g., favorable vs. unfavorable) in patients who underwent eCPR compared to those who did not or between different predictor groups. RD quantified the absolute difference in the risk of a neurological outcome (e.g., favorable vs. unfavorable) between patients who underwent eCPR and those who did not or between different predictor groups. NNT estimated how many patients need to undergo eCPR to prevent one unfavorable neurological outcome or to achieve one favorable neurological outcome, compared to alternative interventions or exposures.
Effect size calculation
Effect sizes were computed for each study based on relevant outcome measures and sample sizes. Variance estimates were derived from reported standard errors, confidence intervals, or calculated from raw data.
Meta-analysis
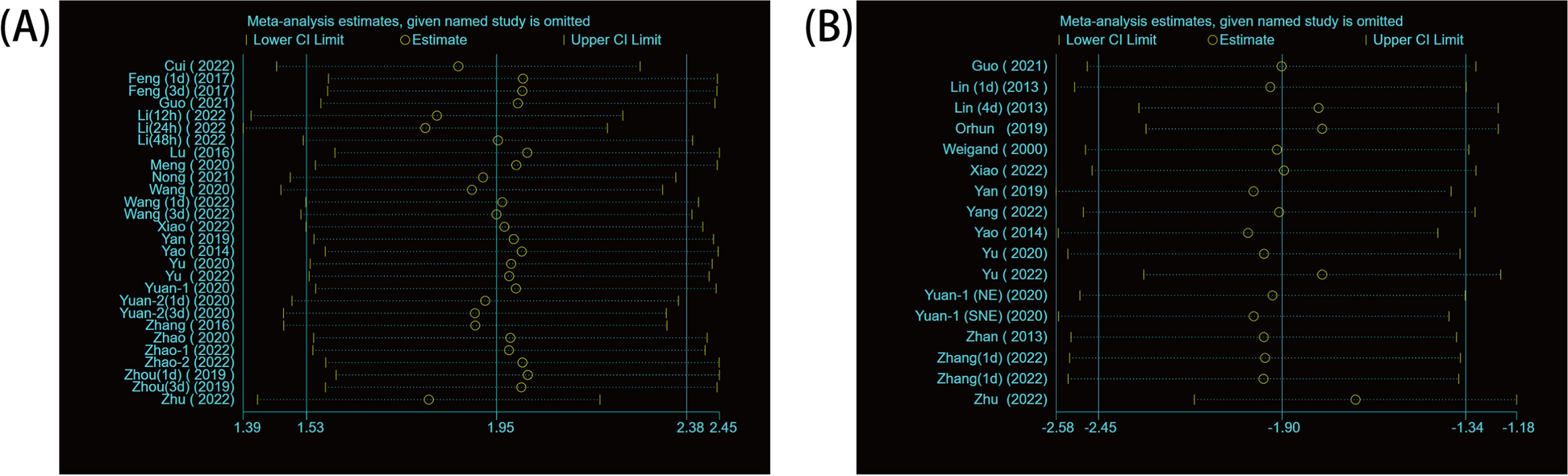
A random-effects model with inverse variance weighting and Hartung-Knapp adjustment was employed to pool effect sizes across studies. Forest plots were generated to visualize individual study effects and the pooled estimate with 95% confidence intervals (CI). Heterogeneity was assessed using Cochran’s Q statistic and Higgins & Thompson’s I2 statistic. Publication bias was examined using funnel plots and tested using Egger’s regression test or Begg’s rank correlation test.
Statistical software
All statistical analyses were performed using Python (version 3.14, libraries: pandas, numpy, statsmodels). P-values less than 0.05 were considered statistically significant. Sensitivity analyses were conducted to assess the findings, exploring study quality, sample size, and methodological differences.
Data synthesis
For data synthesis in this systematic review, a multi-faceted strategy was implemented. Firstly, a narrative synthesis approach was adopted, grouping studies by design, patient characteristics, interventions, and outcomes. Key findings were qualitatively summarized, with an emphasis on identifying patterns and discrepancies. Subgroup analyses were conducted to explore heterogeneity, examining factors such as study design and patient demographics.

Comments (0)