
Remember me
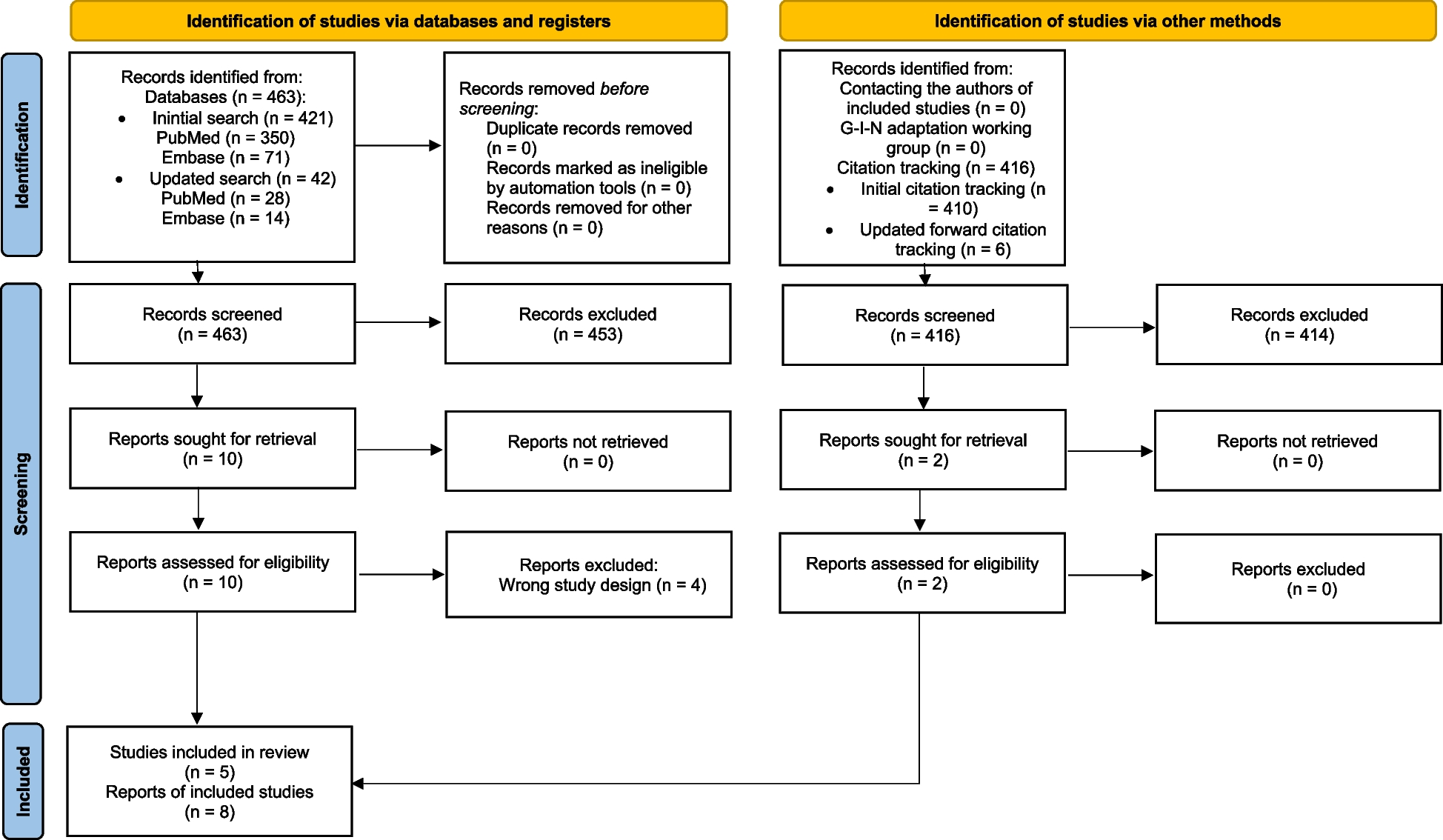
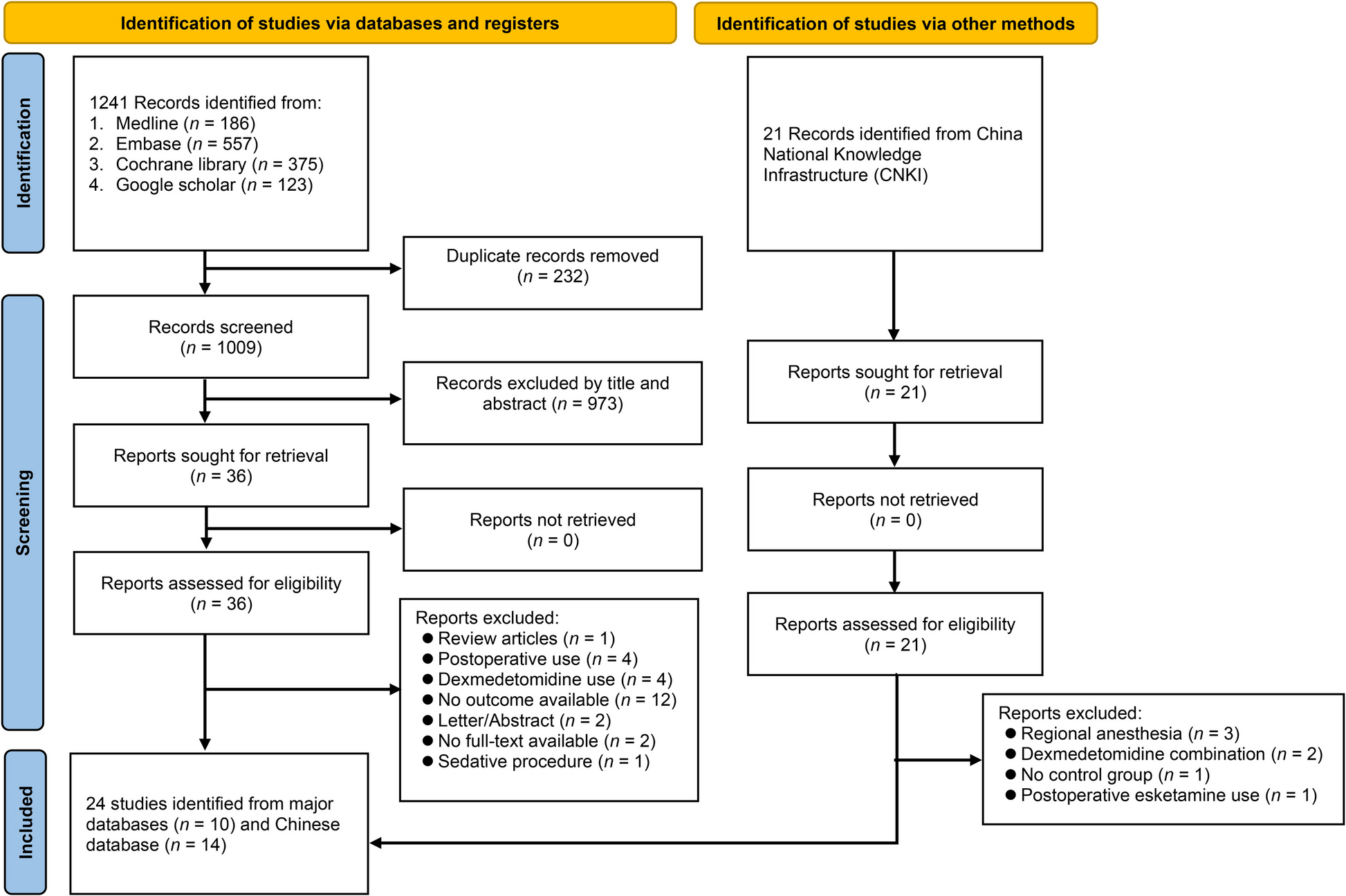
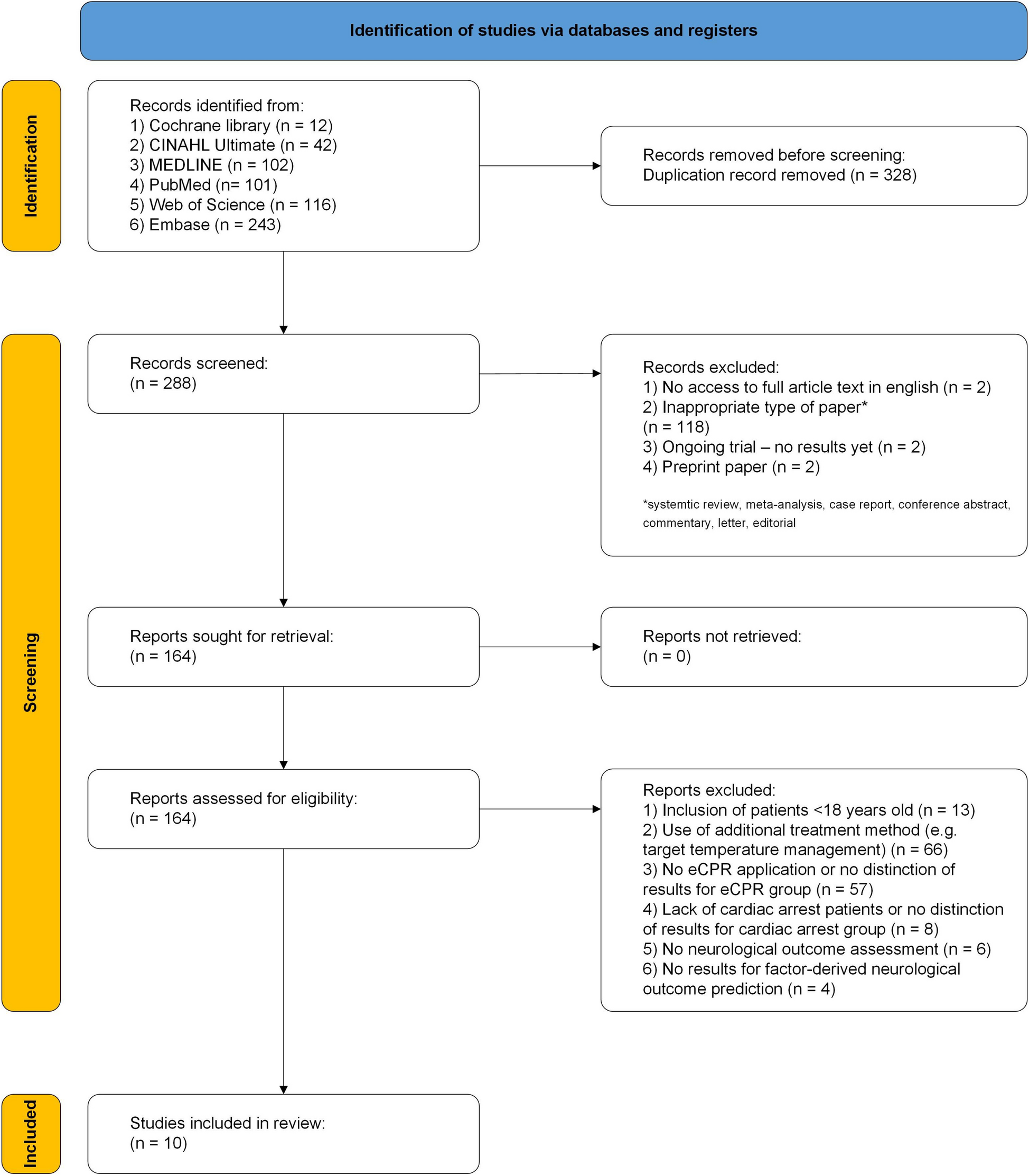
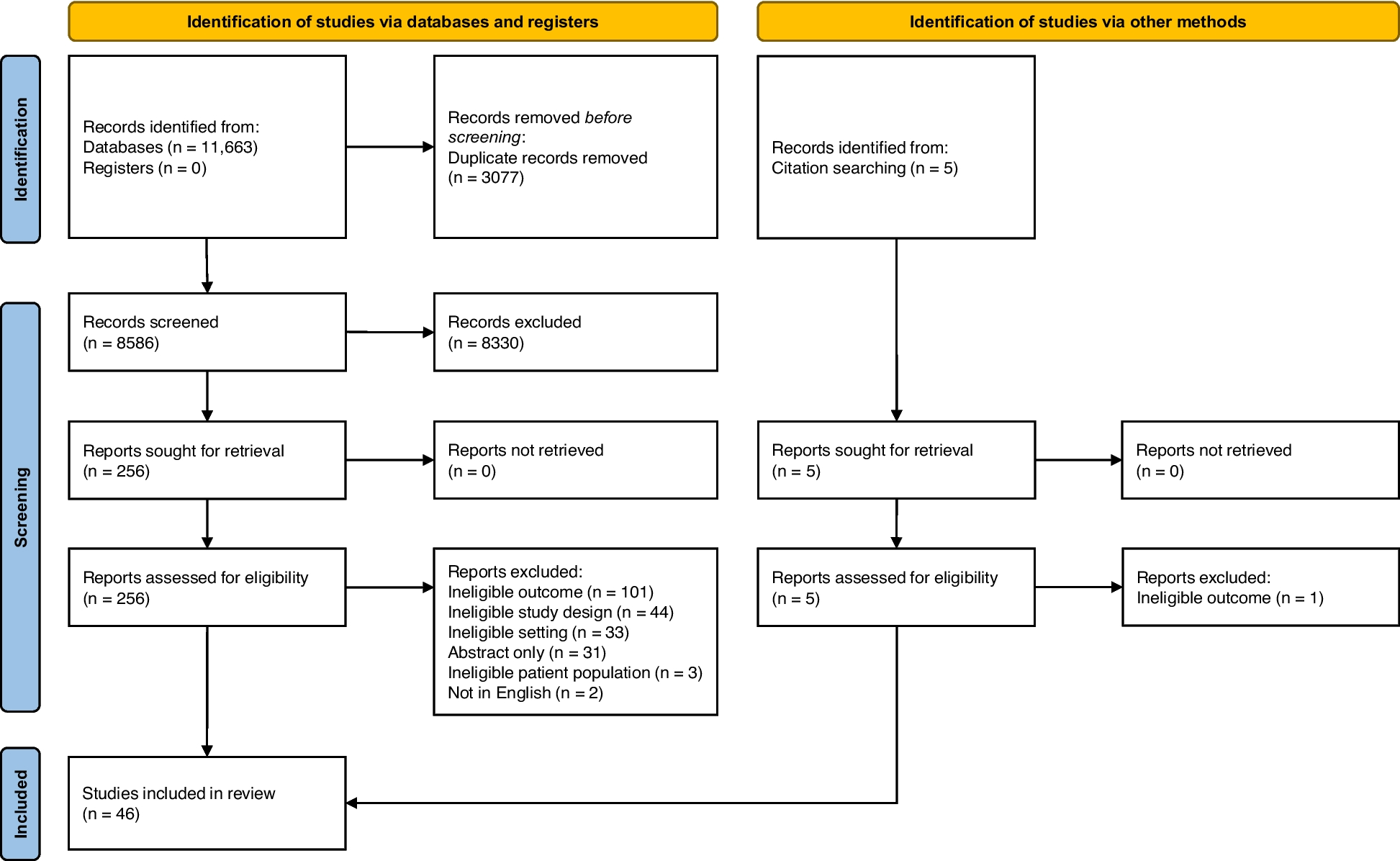
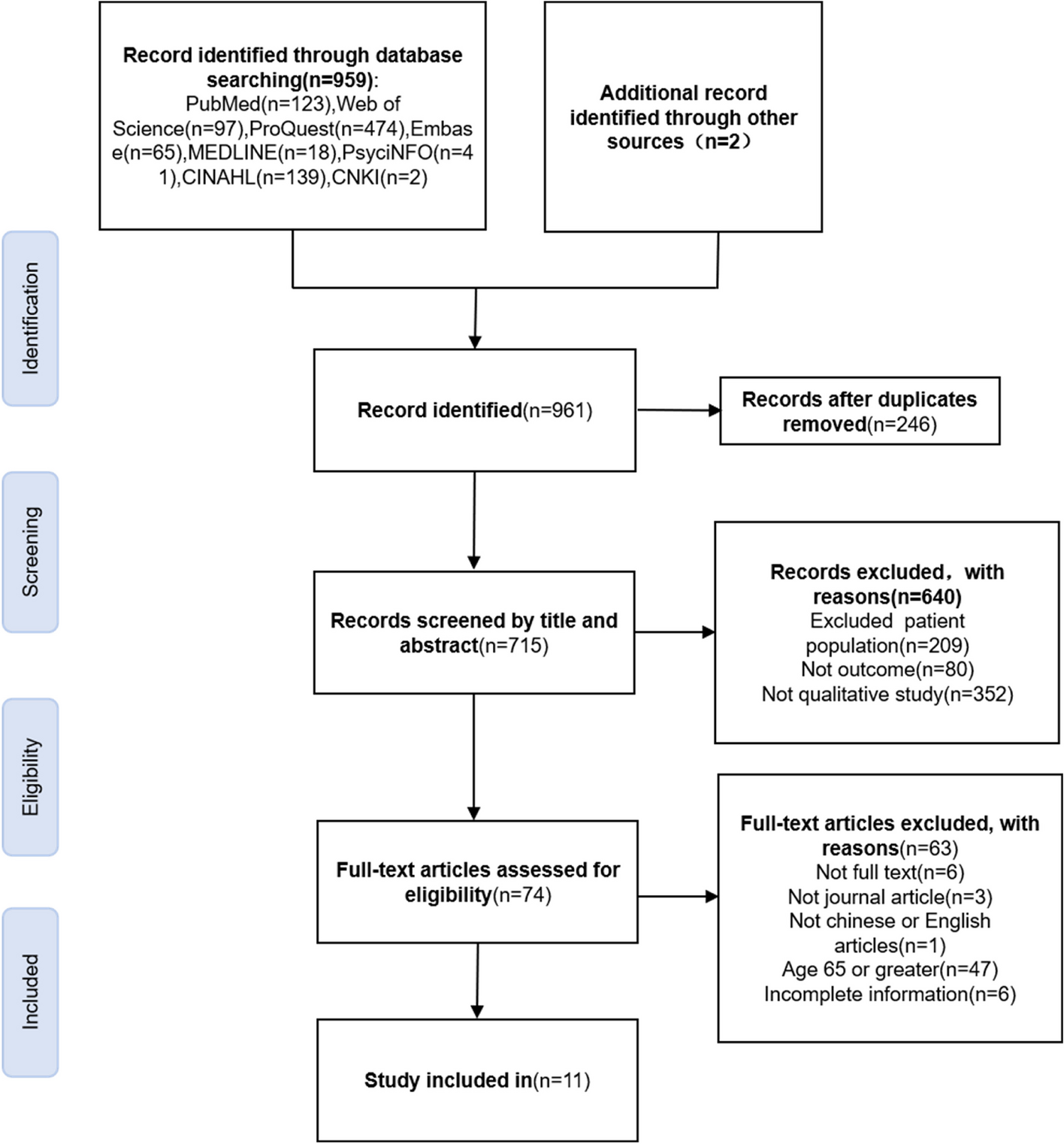
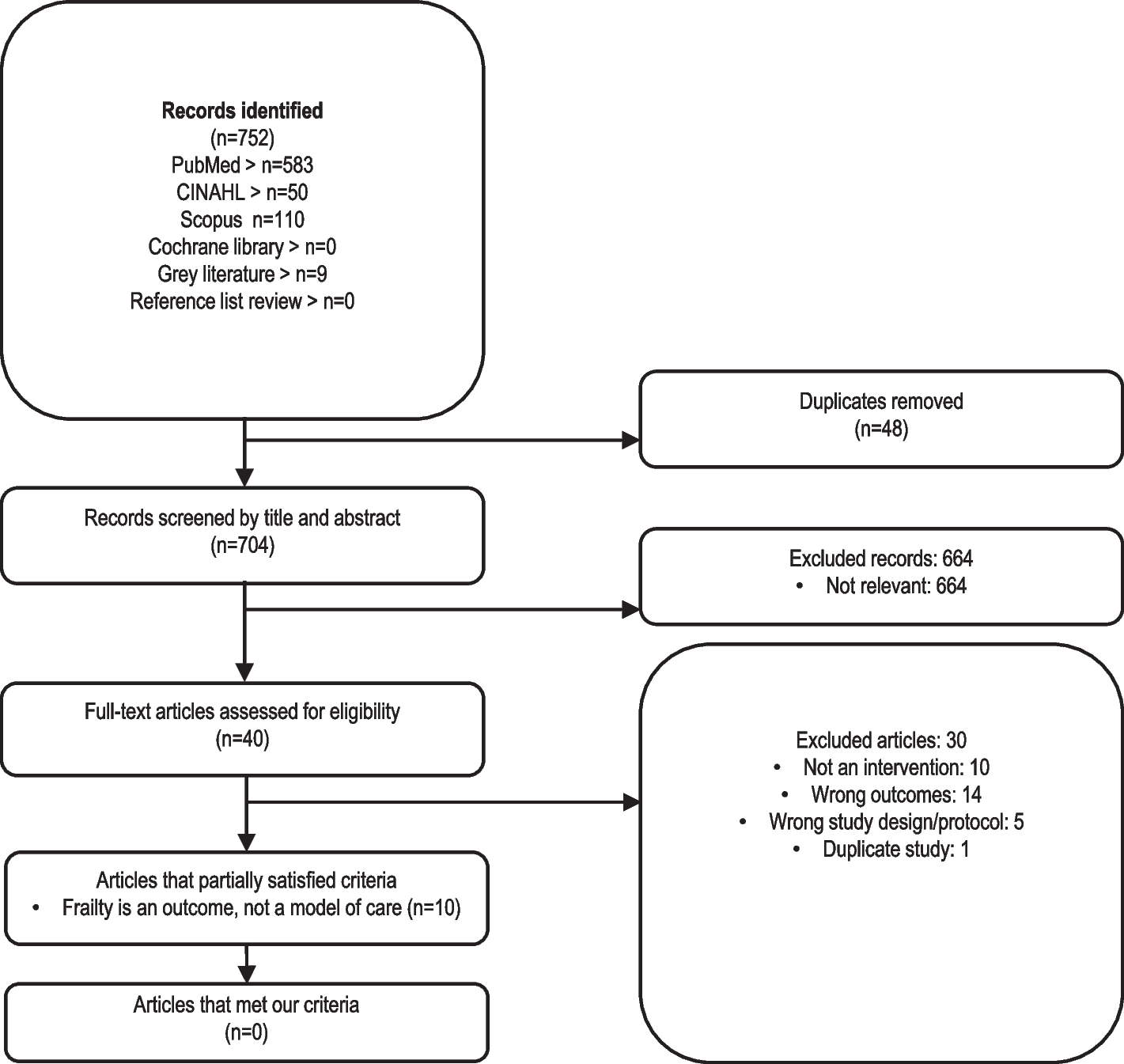
A total of 11,663 abstracts were initially identified from the database searches (Fig. 1). After deduplication, 8586 studies underwent title and abstract screening, 256 underwent full-text screening review and 43 were found to be relevant. Studies were excluded after full-text screening for the following reasons: ineligible outcomes (n = 101), ineligible study design (n = 44), ineligible setting (n = 33), abstract-only study (n = 31), ineligible patient population (n = 3) and full text not in English (n = 2). Five additional studies were identified through citation searching; however, one was excluded due to an ineligible outcome. This report is focused on a total of 46 Canadian studies (Additional file 3) examining unmet primary healthcare needs.
Fig. 1 Description of the included studies
Description of the included studiesA detailed description of the included studies is presented in Table 1. Of the included studies, 32 focused on unmet needs in general healthcare [13, 17,18,19,20, 27, 36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61], and 11 focused on unmet needs in mental healthcare [12, 21, 22, 26, 62,63,64,65,66,67,68]. Three studies focused on unmet needs in both general and mental healthcare [69,70,71]. Two of the included studies were longitudinal in design [36, 63] while the rest were cross-sectional. The studies were conducted between 1998 and 2023, where sample sizes ranged from 320 in a community-based study conducted in Edmonton, Alberta [22] to over 400,000 in a study that pooled multiple national-level population-based surveys [42]. There were differences in the data sources used across the included studies. The most common data sources were the Canadian Community Health Survey (CCHS, n = 26), the Health and Housing in Transition study (HHiT, n = 3), and the Canadian Longitudinal Study on Aging (CLSA, n = 2). The remaining sources were used in one study each. The minimum average age within the study was 38.2 years, and the maximum average age was 67.7 years. Sex distribution varied vastly with female participants making up 12.4% to 100% of study participants. All provinces and territories of Canada were included in 5 studies, 20 included all provinces but not the territories, 6 were conducted in Ontario, 4 in Quebec, 4 in British Columbia, 3 in Ontario and British Columbia, 1 in Alberta, 1 in Ontario and New Brunswick, and 1 in Nova Scotia, New Brunswick, Prince Edward Island, and Newfoundland and Labrador. One study included participants from Ontario, Manitoba, Newfoundland and Labrador, Alberta, New Brunswick, Nova Scotia, and the Northwest Territories.
Table 1 Detailed description of included studiesAll included studies defined unmet need as the perceived need for healthcare by study participants that were not received. The recall period for assessing unmet needs ranged from 6 to 12 months; however, it was not specified in three studies [43, 44, 60]. Twenty studies (43%) utilized Andersen’s Behavioral Model of Health Services Use [72], a model that asserts that an individual’s use of the healthcare system is partly determined by factors that predispose and enable them to seek or avoid care and their need for healthcare services, to inform their selection of predictors of unmet need [17, 21, 27, 38, 39, 43, 45, 46, 50, 51, 53, 54, 57, 58, 60, 62, 65, 68,69,70].
FindingsThe five studies that included participants from all provinces and territories in Canada focused on general unmet healthcare needs (Table 1). The proportion of participants reporting unmet needs in these studies ranged from 10.4 [58] to 12.8% [49] as each study used data from different study periods. The 20 studies that reported the rate of unmet needs across all 10 provinces (but not the territories) differed in the data sources they used and study periods they covered. The level of unmet need for general healthcare in these studies ranged from 6.6 [19] to 25.2% [47], while the level of unmet need for mental healthcare ranged from 2.4 [66] to 50.3% [66].
Sixteen studies reported the rate of unmet need for general healthcare at the provincial or territorial level. The level of unmet needs ranged from 12.0 to 24.7% in British Columbia [40, 46, 52, 69] 8.0 to 23.6% in Ontario [13, 27, 53, 60], and 18.4% to 52.3% in Quebec [20, 41, 43]. Three studies reported an unmet need proportion of 37.7% in Ontario and British Columbia [18, 36, 71], one reported a proportion of 10.0% in Ontario and New Brunswick [59] and another one reported a proportion of 3.5% across six provinces and the Northwest Territories [57].
Seven studies reported an unmet need for mental healthcare at the provincial level. These were 47.6% in Alberta [22], 39.9% in Quebec [63], 23.5% in Ontario and British Columbia [71], 60.0% in Nova Scotia, New Brunswick, Prince Edward Island, and Newfoundland [68], a range of 4.5% to 68.3% in Ontario [12, 26] and a range of 10.4% to 16.5% in women residing in British Columbia. MacLean et al. (2021) only reported the rate of general unmet needs among veterans and the general population, stratified by sex [37]. Female veterans had higher rates of unmet needs relative to their general population comparators (16.2% vs. 13.4%). Male veterans and their comparators both had an unmet need rate of 9.9%.
A summary of the associations reported in the included studies is presented in Table S1 (Additional file 4). The most frequently investigated factors were sex/gender (n = 36), age (n = 34), education (n = 30), and income (n = 29). A significant proportion of these studies found notable associations between health conditions and unmet needs, including chronic conditions (17/21), specific health conditions (14/15), mental health diagnoses (20/21), and perceived health (22/26). Likewise, 13 out of 15 studies found significant associations between having a primary care provider and unmet needs. Age was the most frequently reported significant variable, with 24 out of 34 studies identifying significant associations. Other variables showing significant associations included province (7/8), education (19/30), income (20/29), substance use (4/6), and social support (8/12). In contrast, variables such as immigration status (10/14) and health insurance (5/7) largely did not show significant associations. For the remaining variables, the studies did not consistently show significant associations in either direction, indicating a lack of a clear trend. The outcomes from each included study are presented in Tables S2, S3, and S4 (Additional file 5).
Geographical factorsNineteen studies evaluated the effect of geographical factors on unmet needs (Table S2). Ten studies examined the difference in unmet needs between urban and rural residents, with seven finding no significant differences [17, 19,
Comments (0)