
Remember me
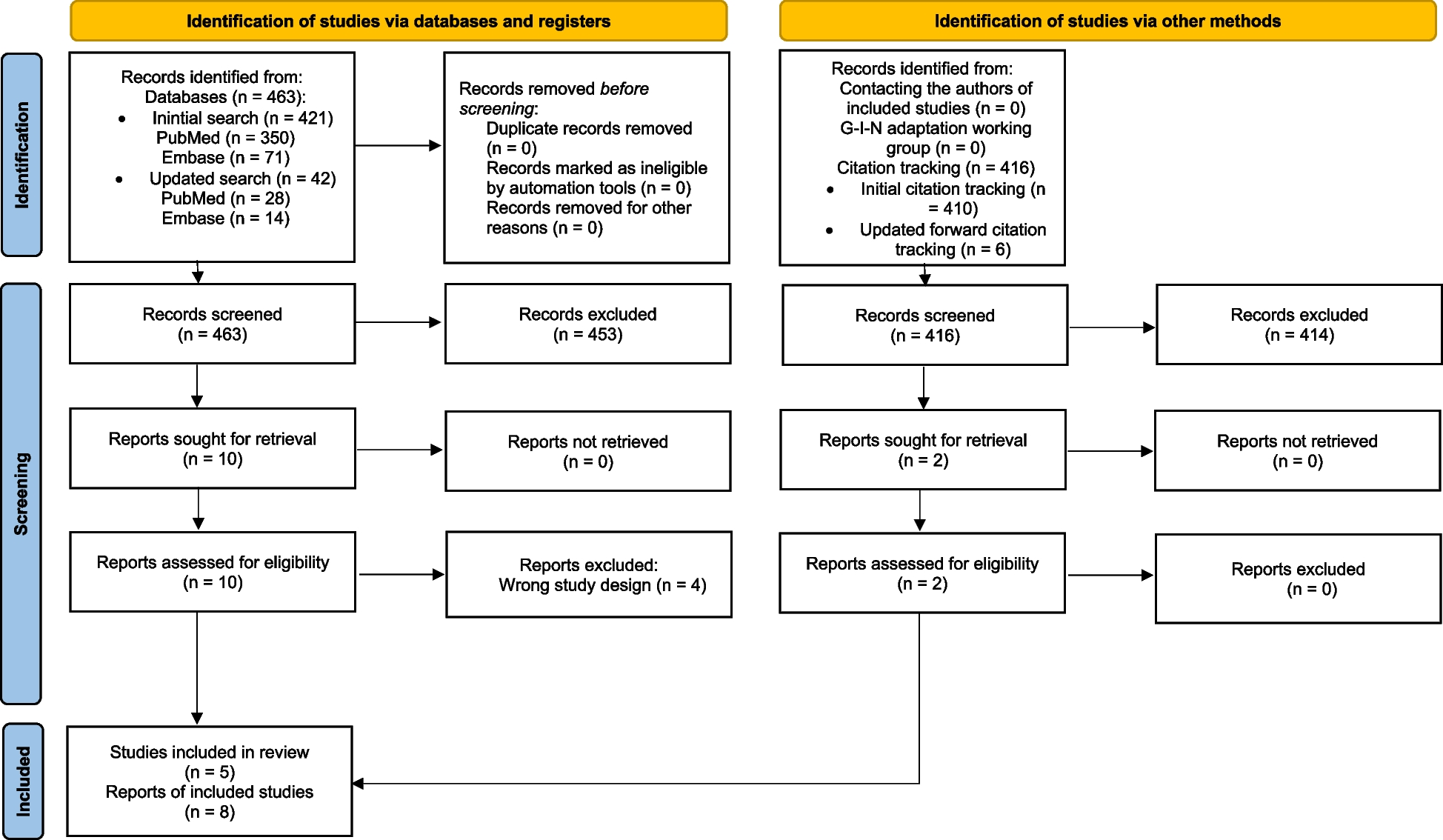
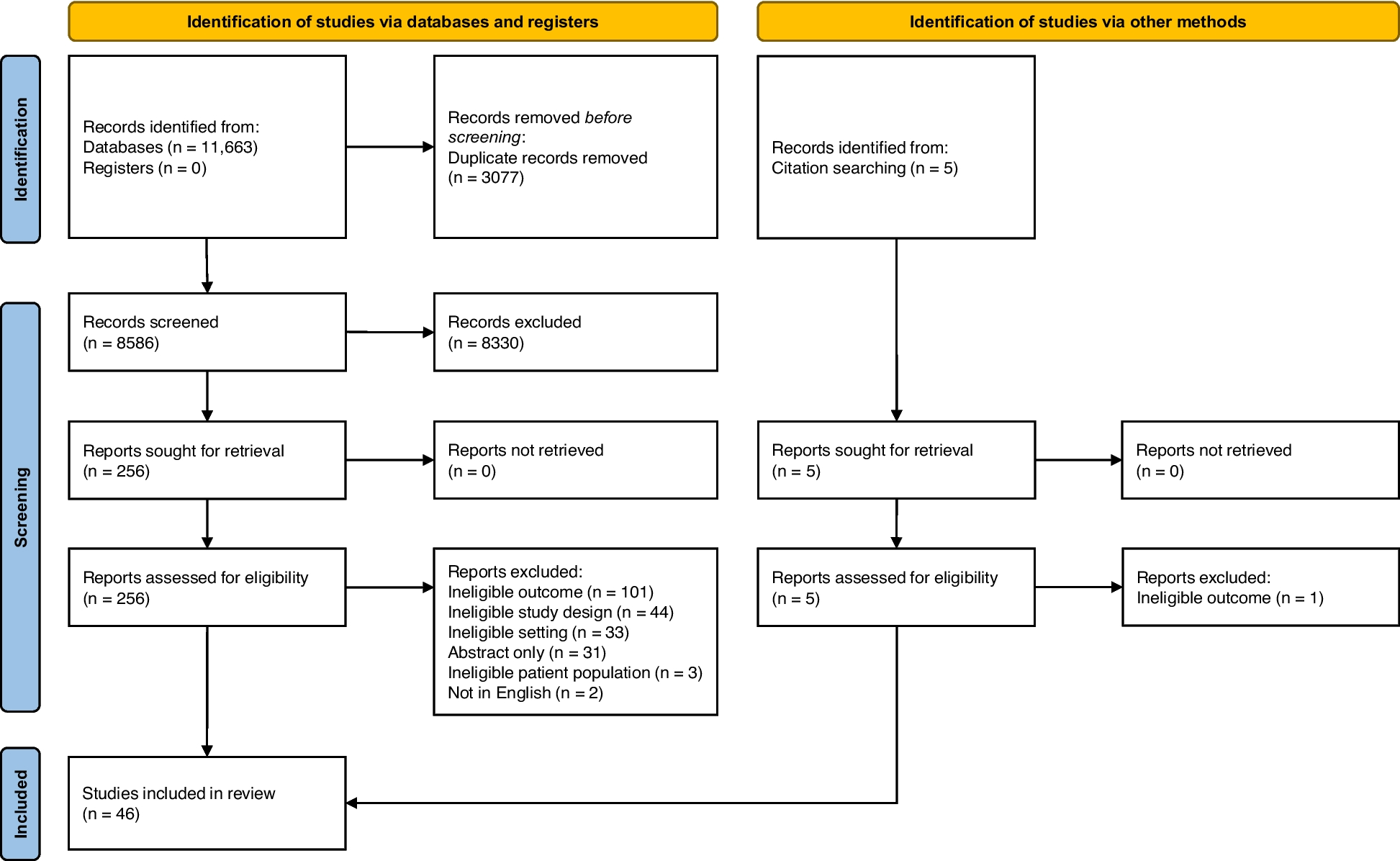
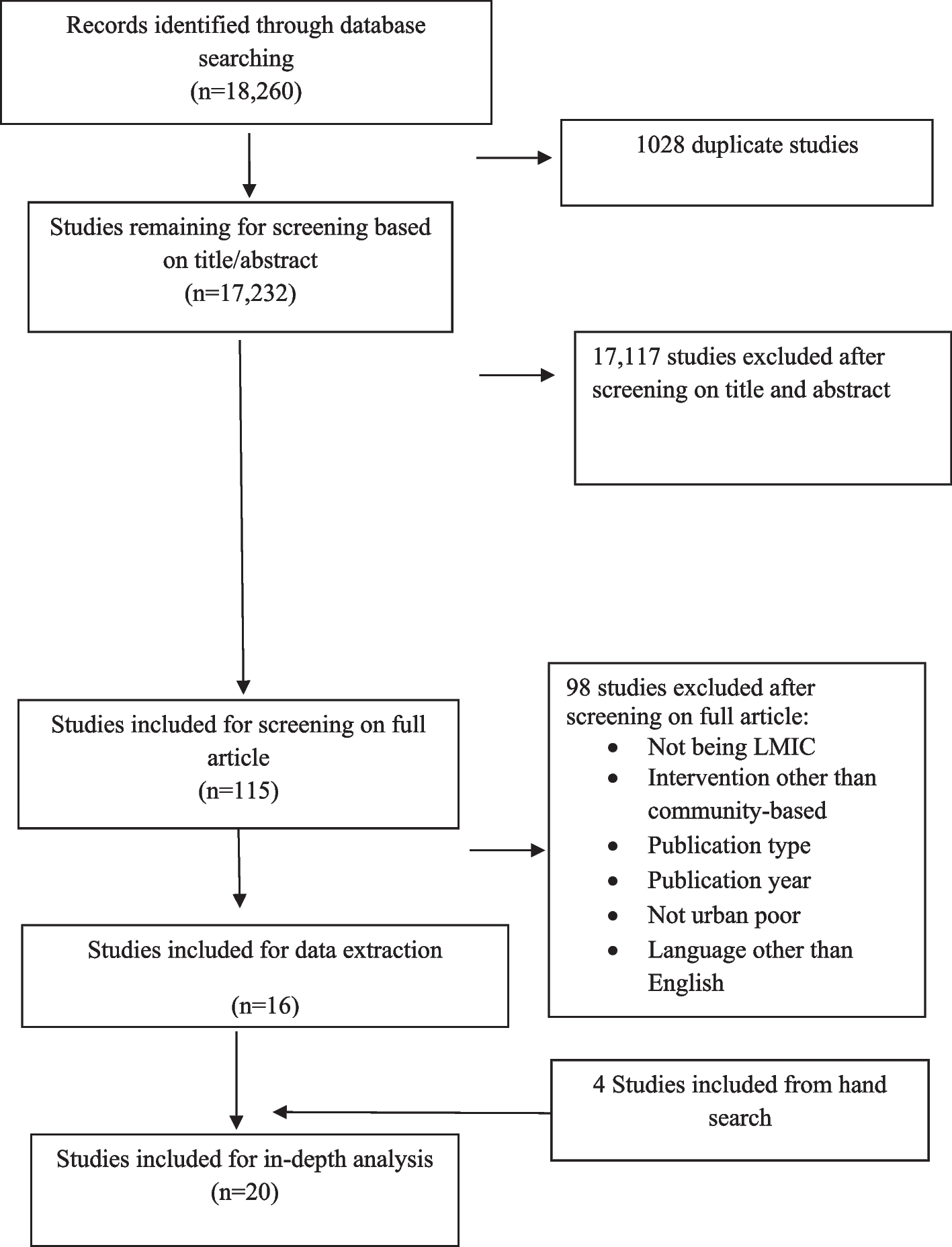
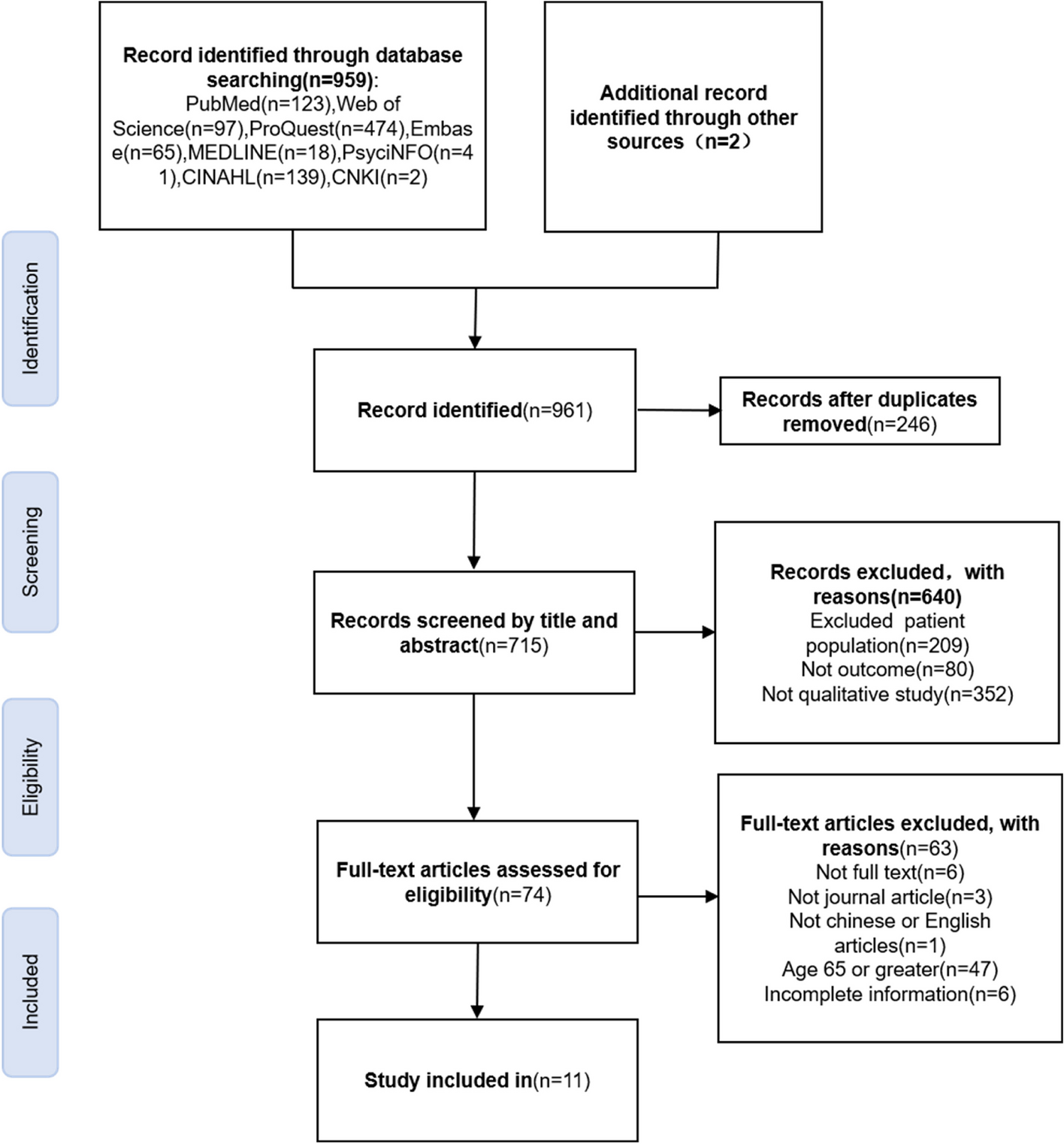
For this systematic review, a total of 18,260 published articles were selected and 1028 duplicate articles were removed, providing 17,232 titles and abstracts for review. After applying the inclusion and exclusion criteria, a total of 115 studies were considered for full-text screening. Among them, 98 articles were excluded and 16 were included. References were checked for all included articles and an additional four articles were included after citation tracking. Finally, a total of 20 articles were considered for the systematic review. Figure 1 provides a detailed “flow diagram” for the study selection process.
Characteristics of included studiesThe primary studies included in this review were sourced from 11 different countries and published in peer-reviewed journals between 2011 and 2021. The geographical distribution of the studies shows that Bangladesh was the most frequently represented country (n = 5) followed by Pakistan (n = 3) and India (n = 3) (Fig. 2). By regional distribution, South Asia was the common setting (12 studies out of 20). Regarding study design, most of the studies were RCT (n = 9) and CRT (n = 6) (Table 1). Few articles were quasi-experimental (n = 3) and cohort (n = 2), while two articles did not specify their study design. The predominant disease was tuberculosis (n = 7) followed by diarrhea (n = 6), dengue (n = 3), and influenza (n = 2). Other diseases such as hepatitis B and C, Haemophilus influenza, diarrhea, and ARIs have one article each (Table 1).
Fig. 2
Geographical distribution of the included studies (n = 20)
Table 1 Characteristics of the included studies by region, intervention type, disease, study design, and sample sizeQuality of the reviewStudy quality and the risk of bias in included studies were assessed systematically following a checklist adopted and modified from the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions and Effective Public Health Practice Project (EPHPP) checklist [33]. Robust methods were adopted to minimize error and bias. A comprehensive systematic search of major electronic databases to identify studies. In addition, references of included studies were checked. Randomized control trials and quasi-experimental trials were considered to capture all varieties of interventions. More than half of the included studies were of high quality (13 studies), 6 studies were of medium quality, and only one study was of low quality. However, the review has several limitations that potentially influenced its findings. Most of the interventions were complex, incorporating multiple components. It was difficult to indicate the effectiveness of any specific component in driving significant changes in the outcomes.
Effective community-based interventionsA range of CBIs focusing on different diseases were found in our review. These include health education [34,35,36,37], socio-economic support [38, 39], behavior change communication [40], water, sanitation and hygiene (WASH) interventions [41,42,43,44,45], e- and m-health [46], social mobilization [47], community-based screening [48,49,50,51], and community-based vector control [52, 53]. This review identified multi-prong approaches and strategies to tackle specific diseases. In the subsequent section, we detailed the effective interventions identified from the review targeting selected infectious diseases (Table 2).
Table 2 Characteristics of the intervention studies included in the systematic reviewHealth educationAcross the reviewed studies, providing health education was identified as the most prevalent community-based intervention [34,35,36,37]. In different studies, health education was reported as an effective intervention to address different types of diseases rather than any particular disease. Kusuma et al. (2016) conducted a quasi-experimental study in the slum population in Delhi, India, to assess the effect of health education on dengue prevention [34]. Health education on dengue transmission and preventive measures was provided through the dissemination of materials such as pamphlets, posters, banners, and audio message recordings. Findings showed a significant increase in awareness that dengue was caused by mosquitoes (20%, p < 0.0001). The use of mosquito repellents/coils and wearing clothes covering full and bed net was increased after receiving this educational intervention by ~ 20%, 11%, and 6% respectively (p < 0.0001). Health education along with counseling by trained community health workers (CHWs) also improved treatment adherence (15%) in contrast to the control group. Utilization of CHW’s most effective in urban setup [OR − 2.65 (95% CI 2.02 − 3.48; p < 0.001)], combining the use of CHWs and treatment adherence had a strong positive association [OR − 8.02 (95% CI 5.43 − 11.88, p < 0.001)] [3].
Kaewchana et al. conducted an RCT where health education was provided to control influenza and its consequences as well [36]. This educational intervention was repeatedly provided to the household individual on handwashing technique and conveying messages such as “Why to wash,” “when to wash,” “how to wash,” and “how handwashing is linked to influenza transmission.” This intervention was able to increase the frequency of handwashing in the intervention group (p < 0.001). In addition, findings showed that in comparison to pre-education and 90 days post-education in the intervention group, the frequency was increased from 4.1 (SD = 2.7) to 5.6 (SD = 3.5). Intervention in handwashing techniques made significant improvement in the duration of handwashing (p < 0.001). It was self-reported by the participants that the frequency of their handwashing increased after using their hands to cover their mouth and nose when coughing, sneezing, and blowing their nose and after touching any other surfaces that were presumed secretion-contaminated (p < 0.001). These findings were identified as the strengths of educational approaches [36]. Health education intervention implemented for mothers of children less than 6 months to increase their knowledge about immunization (through pictorial cards containing messages about the importance of immunization, retaining vaccine card, and logistic information by CHWs) showed a significant improvement of 39% (adjusted RR = 1.39; 95% CI 1.06─1.81) in DPT-3/hepatitis B vaccine completion rates in the intervention group [37].
Socio-economic supportTargeting the TB patients and their households, a socio-economic support was implemented in Peru through several components to tackle TB [38, 39]. To enhance the uptake of TB care and prevention services, home visits, community mobilization workshops, and psychosocial support were integrated within the national TB control program to reduce the burden. Considering poverty as another barrier to the success of TB controlling program poverty-reduction interventions (food and cash transfers, microcredits, microloans, etc.) were also delivered, which engaged 77% of the participants in these interventions. The socio-economic intervention showed a marked increase in TB screening (from 82 to 96%), successful TB treatment completion (from 91 to 97%), and completion of preventive therapy (from 27 to 87%; all p < 0.0001) [38].
Wingfield et al. [39] reported social and economic support through regular household visits, participatory community meetings, education on TB transmission, treatment and preventive therapy, formation of a TB support club, and conditional cash transfer which yielded a treatment success rate of 64% for the intervention group compared to 53% for the control group. Furthermore, the cure rate was higher in the intervention group at 53%, as opposed to 37% in the control group. The rate of preventive therapy completion was 20% in the intervention group, compared to 12% in the control group, with an OR of 1.9 (95% CI 1.1–3.2). The intervention notably increased the initiation of preventive therapy in contacts younger than 5 years (aOR 2.2; 95% CI 1.1–4.2) and among the poorest tertile (aOR 2.2; 95% CI 1.1–4.1), highlighting its effectiveness in these specific subgroups. This multifaceted social support was designed to inform, empower, and reduce TB stigma within the community, while economic support was directly targeted at individual patients [39].
Behavior change interventionsBehavior change intervention was applied in a cluster randomized control trial conducted among children of 24 primary schools in Dhaka, Bangladesh, to prevent influenza, as they are commonly linked to influenza transmission. To promote handwashing practice in low-resource settings where water is scares, hand sanitizer was provided instead of water and soap to intervention schools which were regularly filled by field staff during the intervention period. Besides, hand and respiratory hygiene education was delivered through trained selected teachers regarding proper ways to cover during coughing and sneezing and the use of hand sanitizer at five key times during the day. Each of the enrolled students was provided a plastic ruler containing messages on handwashing with soap and respiratory hygiene etiquette. In addition, a video clip previously developed by icddr,b scientists based on respiratory hygiene practice was delivered during behavior change communication sessions to the students. At the end of the intervention, coughing and sneezing in the open air among the students at intervention schools decreased to 37% (DID = − 63%; 95% CI = 98%, − 27%). Around 18% lower incidence of influenza-like illness (ILI) per 1000 student-weeks was identified among the students of intervention school than that of control school adjusted incidence rate ratio (AIRR): 0.8, 95% CI 0.5─1.3, p value < 0.05)]. Around 53% of lower incidence of laboratory-confirmed influenza per 1000 student-weeks was identified among students of intervention school than that of control school [incidence rate ratio (IRR): 0.5, 95% CI = 0.3, 0.8; p value < 0.01)] [40]. In another study, behavior change intervention along with vaccination was applied and compared with other only vaccinated and control group (no intervention) to assess the effectiveness of OCV vaccine in reducing the incidence of severe dehydrating cholera among high-risk people of age above 1 year and except pregnant women during 2 years after vaccination. In this cluster randomized study, a BCC was applied along with vaccination to encourage handwashing and treatment of drinking water with chlorine by trained CHWs to promote the use of a liquid chlorine-based treatment for household drinking water, each drinking water station included a chlorine dispenser. Overall protective effectiveness was 37% (95% CI lower bound 18%; p < 0.01) in the vaccination group and 45% (95% CI lower bound 24%; p < 0.001) in the vaccination and BCC group [41].
Water sanitation and hygiene (WASH) interventionsFour out of 20 studies [42,43,44,45] reported WASH interventions aimed at reducing the incidence of diarrheal diseases and acute respiratory infections (ARI) in different settings. In Bangladesh, oral cholera vaccine (OCV) and WASH interventions provided protection against severe dehydrating cholera in the vaccination plus BCC group (45%; 95% CI 13–55; p < 0.001) [42]. Najnin et al. [42] assessed the impact of handwashing and water purification on oral cholera vaccination (OCV) in Bangladesh and found a reduction in diarrhea-associated hospitalization rates in the vaccine-plus-BCC group (4.1/1000 person-years; 95% CI 3.4–5.0) compared to the vaccine-only (4.7/1000 person-years; 95% CI 4.1–5.6), and control groups over a period of 2 years (4.7/1000 person-years; 95% CI 3.9–5.8) [42]. Lindquist et al. [43] evaluated the efficacy of household-level hollow fiber filters and BCC on WASH. A significant reduction in diarrheal disease in children under five using the filters was shown by diarrheal prevalence ratios of 0.21 (95% CI 0.15–0.30) for the filter arm and 0.27 (95% CI 0.22–0.34) for the filter and WASH BCC arm [43]. Effects of a handwashing intervention on health outcomes and school absenteeism in Indian urban communities showed a relative risk reduction in diarrhea RRR-21.3 and ARIs (ARI-19.9) among children with a reduction in the number of days of school absences [44]. Pickering et al. [45] evaluated the effect of a water storage tank compatible with dosing devices at shared water points in urban Bangladesh which reported a reduction in diarrheal prevalence and hospital visits for gastrointestinal illnesses among children under five (control − 4%, intervention − 3.7%) [45].
e- and m-health interventionKazi et al. [46] conducted a study in Pakistan to examine the effectiveness of SMS reminders on the uptake of routine immunizations in urban squatter settlements. The study targeted infants under 2 weeks of age, whose caregivers had mobile phone access and could read SMS text messages. The intervention group showed a higher rate of immunization coverage for the first dose of the pentavalent vaccine (DPT-Hep-B-Hib) at 6 weeks compared to the control group (intervention arm, 96.0% vs. control arm, 86.4%; p < 0.05) [46].
Social mobilizationIn 2013, Khan et al. conducted a RCT in the high-risk cholera-endemic urban areas of Dhaka, Bangladesh, to assess the feasibility and impact of a large OCV program aimed at reducing cholera incidence. The program involved social mobilization strategies, including interpersonal communication by field workers, advocacy meetings, and targeted mobile messages to ensure high vaccine coverage among the susceptible urban population. To further boost coverage, mop-up activities were conducted, involving house-to-house visits targeting those who missed the second dose. The study found that vaccine coverage was 81% among children, and coverage among females was significantly higher than in males (77% vs. 66%, p < 0.001) [47].
Community-based screeningA quasi-experimental study was undertaken to increase TB case detection by adopting an integrated intervention which included arranging chest camps for active case detection at the clinics of private non-NTP general practitioners (GPs) and using a light-emitting diode (LED) microscope with fluorescence microscopy. Local GPs received 3 days of training regarding diagnosis, recording, and reporting of TB in the provincial TB control program and were encouraged to refer TB presumptive cases to temporary laboratories in a nearby GP clinic. Promotional activities were assumed prior to the chest camps such as announcing through loudspeakers about the camps and free general medicine including displaying posters and banners in Urdu and in the local Sindhi language. To attract the local community, health fairs were arranged that included street theatre, fun shows, and stalls. This integrated intervention is evident that the proportion of smear-positive results was significantly higher among those from engaged private providers than among those referred from camps (OR 1.54, 95%CI 1.42–1.66). During the project, the total number of smear-positive TB notifications increased over the intervention period from 5158 to 8275 [48].
Another study was conducted among the slum population of two cities, Hyderabad and Bengaluru, India, through USAID-funded Tuberculosis Health Action Learning Initiative (THALI) to support them in gaining access to TB services. To increase awareness among the slum population, THALI trained 112 CHWs and placed them in urban slums to visit and conduct activities in the slums fortnightly. They referred symptomatic TB cases to the nearest center for sputum testing and also visited households with positive cases. They also supported TB patients and families with counseling, contact screening, monitoring treatment adherence, weight follow-up during visits, and social scheme linkages. Their counseling also covered relevant behavior change (smoking and alcohol consumption) and referring the TB patients to a doctor for management of adverse effects or side effects management and co-morbidities. These community-based activities through the CHWs showed an increase in TB detection rate in Bengaluru from 5.5 to 52.0 per 100,000 during the period, while in Hyderabad, it was 35.4 initially and increased up to 118.9 per 100,000 persons. The treatment success rate was 87.1% through the intervention. Weight (OR 1.60, p < 0.05), the total number of follow-up visits (OR 10.73, p < 0.001), TB awareness counseling (OR 2.75, p < 0.001), adherence counseling (OR 3.34, p < 0.001), nutritional counseling/support (OR 2.43, p < 0.001), and family level counseling (OR 1.90, p < 0.05) were intriguing factors for the successful treatment outcome [48].
In Cambodia, a study assessed the feasibility and effectiveness of community-based active case finding (ACF) for TB in disadvantaged urban areas which reported a high initiation of treatment (95%), a successful treatment outcome (81%), a cure rate (69%), and a completion rate (12%) over a period of 51 days [50]. Rocinha, Brazil’s largest urban slum, implemented capacity building of the laypersons as CHWs to supervise TB treatment, launching a campaign to find out active cases of TB, home visits for screening symptomatic individuals, and educational activities to enhance TB control. This multi-prong intervention resulted in an increased treatment success rate (from 67.6 to 83.2%). Furthermore, the TB case rate declined by an average of 39 cases per 100,000 population every 6 months in the post-intervention period [51].
Community-based vector controlIn Venezuela, a community-based vector control intervention was implemented to prevent and control dengue in urban informal settings [52, 53]. A CRT was conducted to evaluate the effectiveness of long-lasting insecticide-treated materials (ITMs), such as curtains and jars, for controlling Aedes aegypti, the primary vector for dengue. The results showed a significant impact, with an incidence rate ratio of 0.98, suggesting a slight reduction in dengue incidence due to the intervention [52].
The Camino Verde (Green Way), a pesticide-free evidence-based community mobilization, was added to the conventional dengue control program in the intervention sites to test whether it enhances effectiveness in dengue prevention in Nicaragua and Mexico. In this cluster, randomized control trial intervention sites followed a protocol to engage communities through a variety of events based on local vector reservoirs and community resources like puppet shows and basketball tournaments, clean-up campaigns focused on unoccupied and public premises, and introduction of fish into water storage containers for 1 year. These intervention sites participated in a community discussion of baseline evidence engaging the community leaders which helped to motivate community involvement during and beyond the study. Communities opted for a series of activities to raise awareness and share basic knowledge on the mosquito life cycle and how to interrupt it through volunteer visits at households and schools. This multi-country community-based study showed community mobilization to be an effective intervention for dengue vector control as household evidence of recent dengue virus infection among 3–9-year-old children was reduced (relative risk reduction (RRR) − 29.5, (95% CI − 3.8, − 55.3), p < 0.05), past self-reported dengue illness decreases (RRR) − 24.7, 95% CI − 1.8, − 51.2), p < 0.05), house infested with larvae or pupae (RRR − 44.1, 95% CI − 13.6, − 74.7), p < 0.001), containers with larvae or pupae (RRR 36.7, 95% CI − 24.5, − 44.8), p < 0.001), and the number of pupae (RRR 51.7, 95% CI − 36.2, − 76.1), p < 0.001) [40].
Effectiveness of intervention for specific infectious diseasesThis systematic review finds different types of community-based interventions for specific diseases, e.g., TB, dengue, diarrhea, influenza, and ARI. In this section, we have reported disease-wise intervention and their effectiveness (Table 3).
Table 3 Summary of the effective community-based intervention for prevention and control of infectious diseases in LMICsTuberculosisTable 3 outlines various interventions for TB and their components along with their effectiveness. For health education, the interventions included health education by community health workers (CHWs), supervision of directly observed treatment (DOTs), and follow-up home visits, leading to increased adherence to treatment [35, 36, 39]. Socio-economic support involved income generation activities, community mobilization workshops, psychological counseling, poverty reduction activities, and forming TB support groups, which resulted in improved household contact TB screening, successful TB treatment completion, rapid MDR-TB testing uptake, and increased preventive therapy initiation [38, 39]. Community-based screening included follow-up visits with counseling, social scheme provision during communication phases, household and symptomatic case screening through door-to-door visits, and facilitating TB screening by home collection and transport, resulting in increased case detection, treatment success, and treatment initiation rates [48,49,50].
DiarrheaThe interventions for diarrhea focus on BCC and WASH. Behavior change interventions include BCC for increased handwashing, distribution of soapy water and soap, interpersonal counseling on handwashing and water treatment, and establishing social norms for hygiene, resulting in reduced diarrhea prevalence, improved (OCV) coverage, and decreased hospitalization rates [41,42,43,44]. WASH interventions included setting up free handwashing stations, providing household-level hollow fiber filters, and establishing water storage tanks with dosing devices for water purification, leading to improved OCV coverage, reduced diarrhea prevalence, and fewer hospital visits for diarrhea [41, 43, 45] (Table 3).
DengueThe same table shows that health
Comments (0)