
Remember me
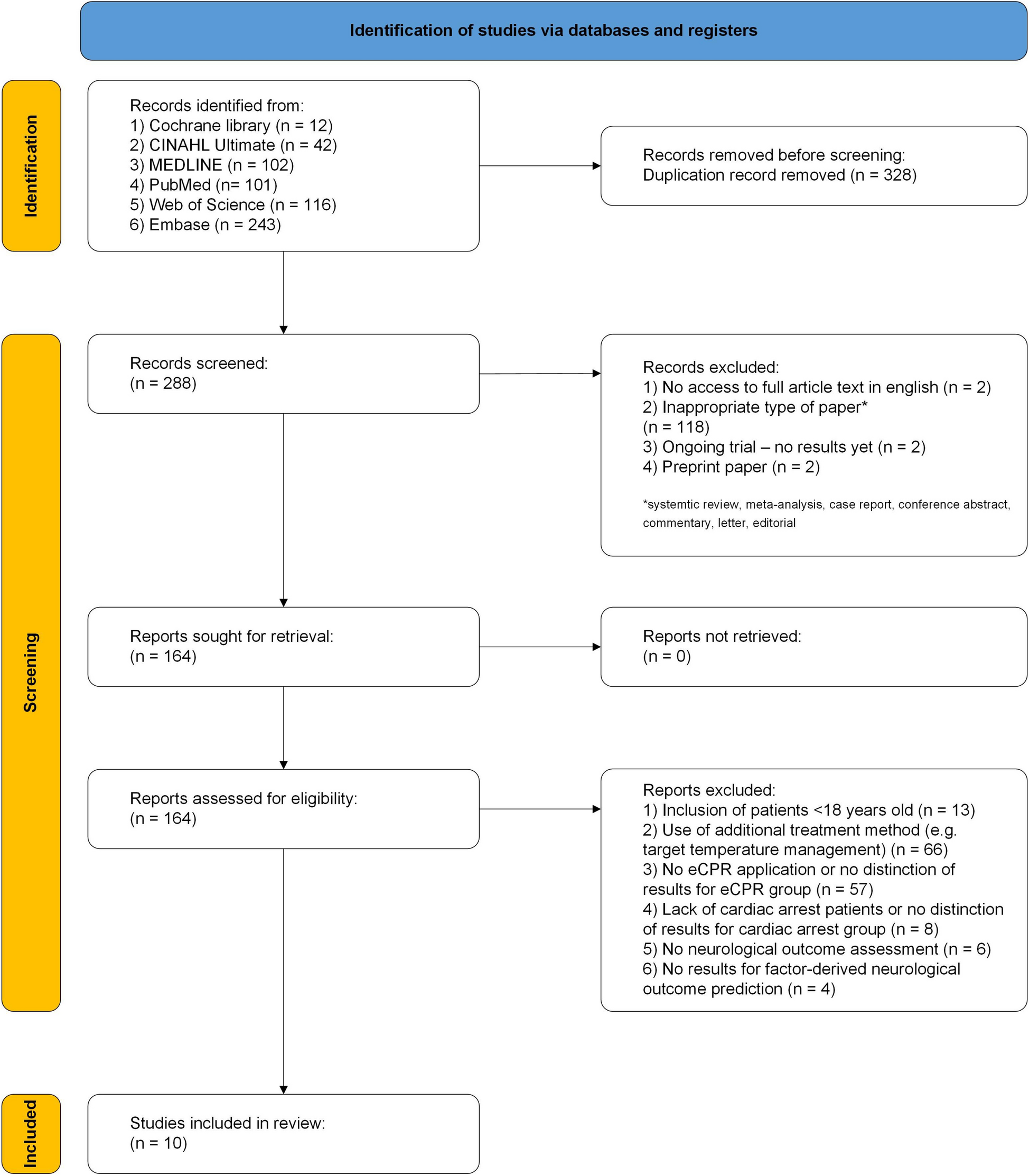
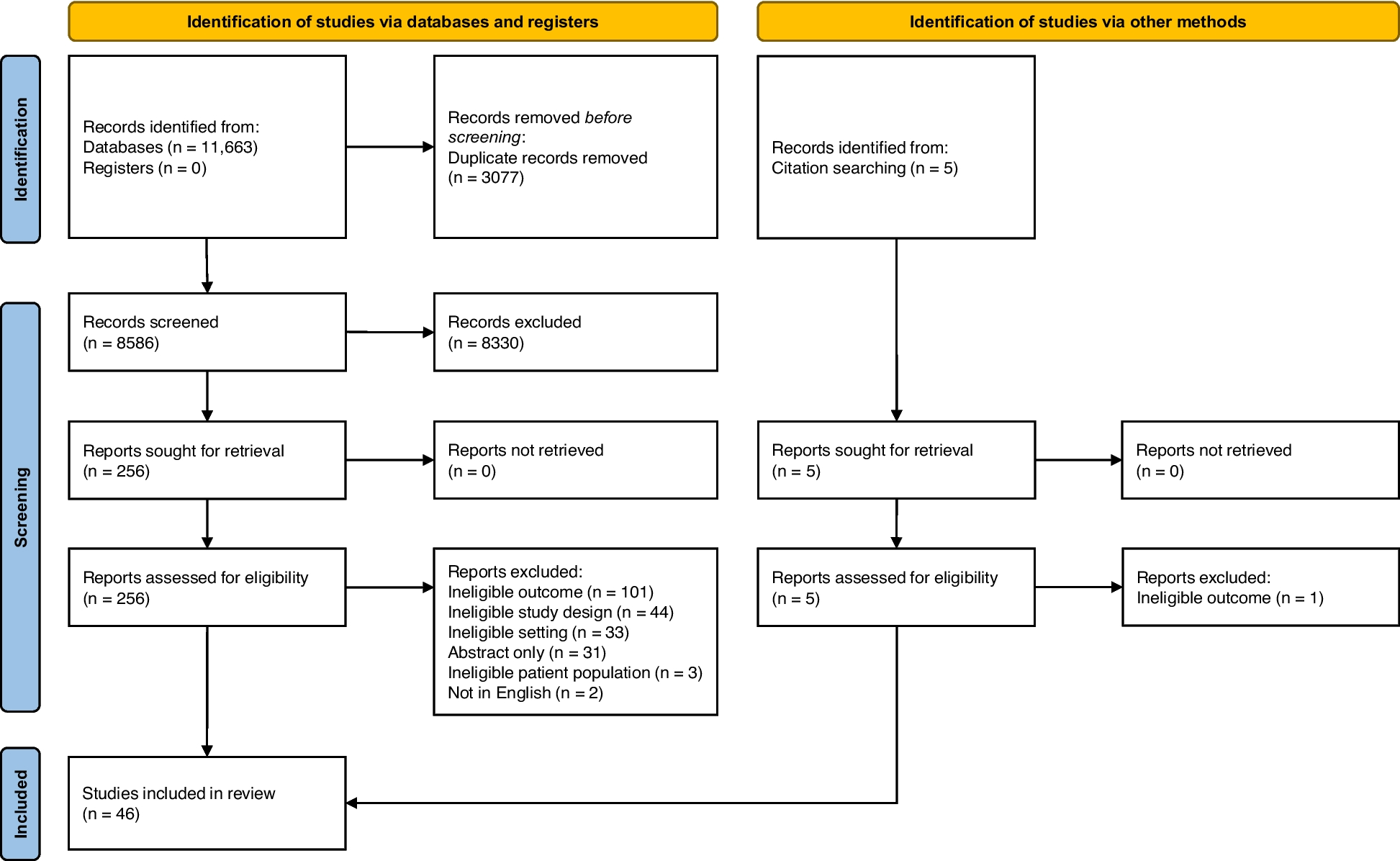
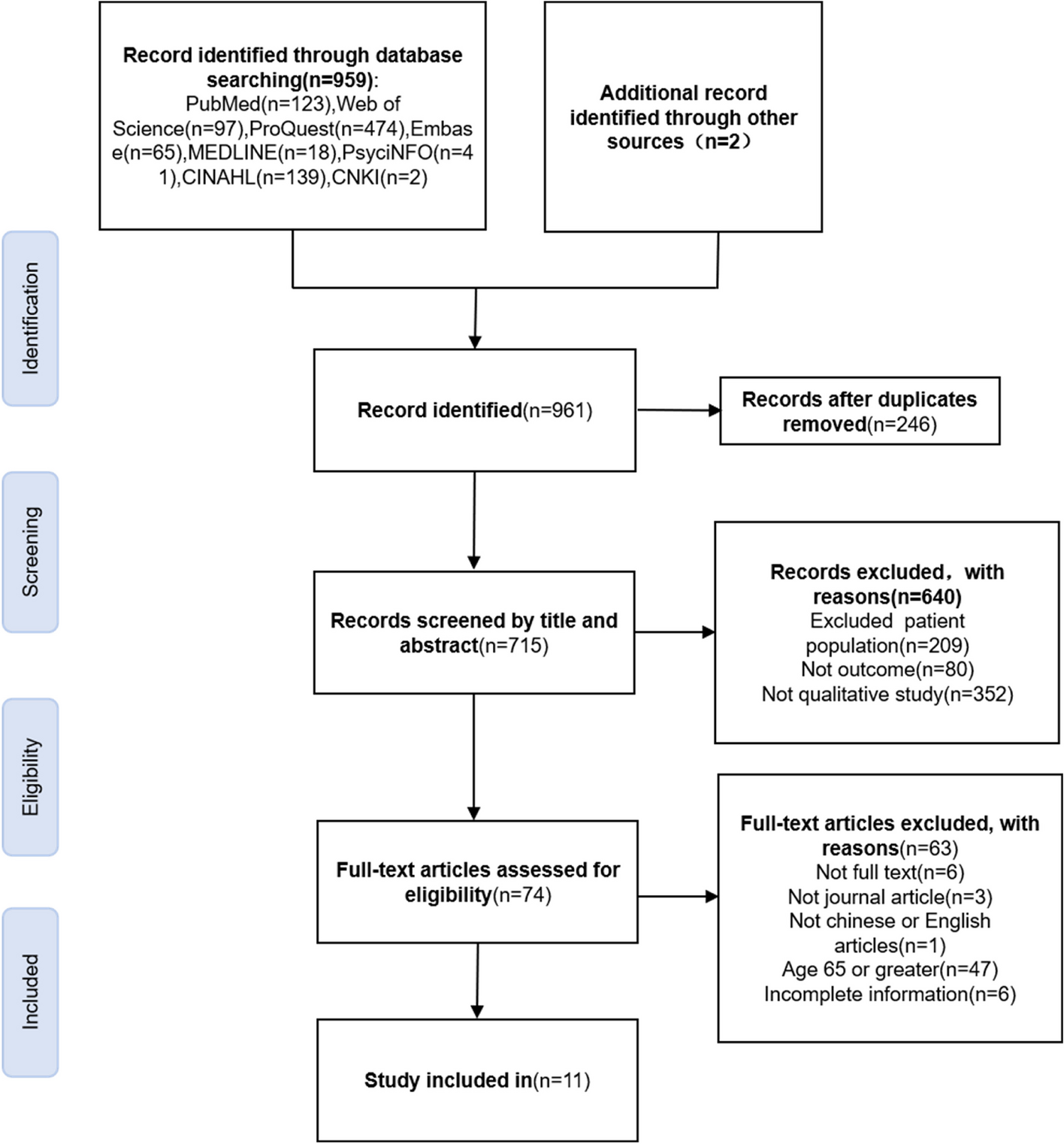
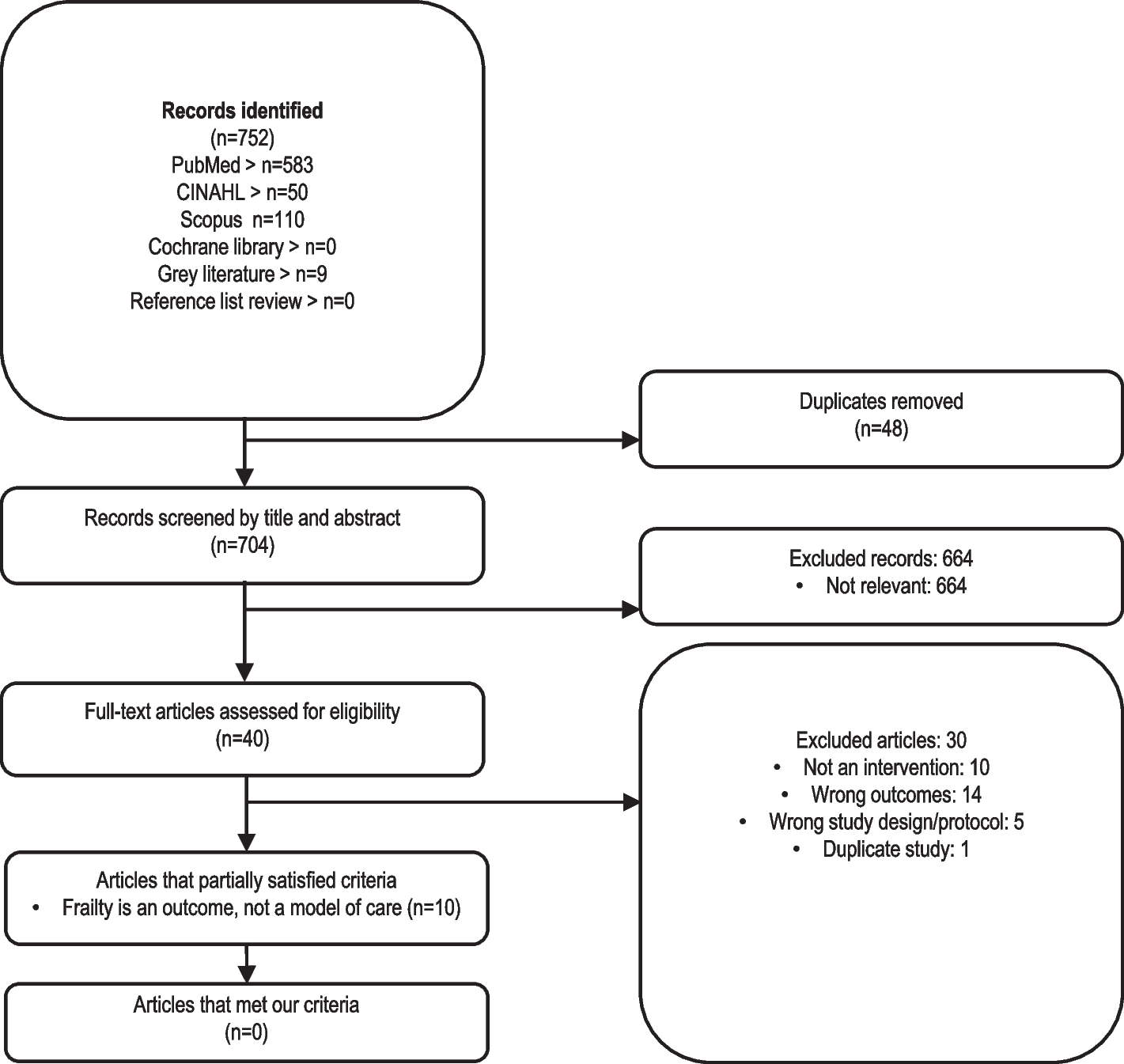
The searches yielded 3026 records. After 321 duplicates were removed, 2705 records remained to be screened. We excluded 2541 records on title and abstract screening. We assessed 164 full‐text articles for eligibility and excluded 127 full‐text articles. Twenty-five original studies met our inclusion criteria (Fig. 1). Additional file 3 presents the list of excluded studies, and Additional file 4 describes the twelve ongoing studies.
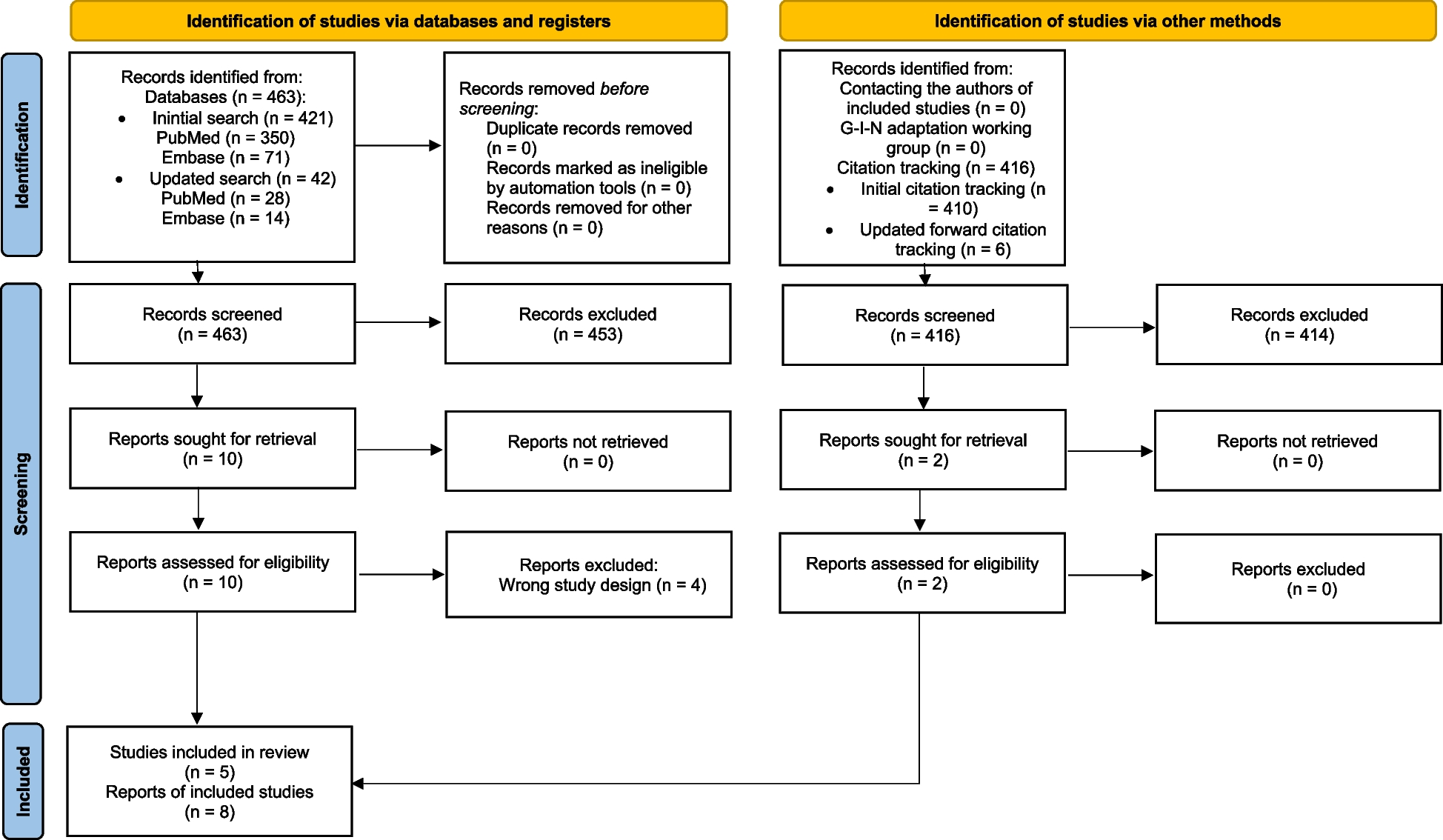
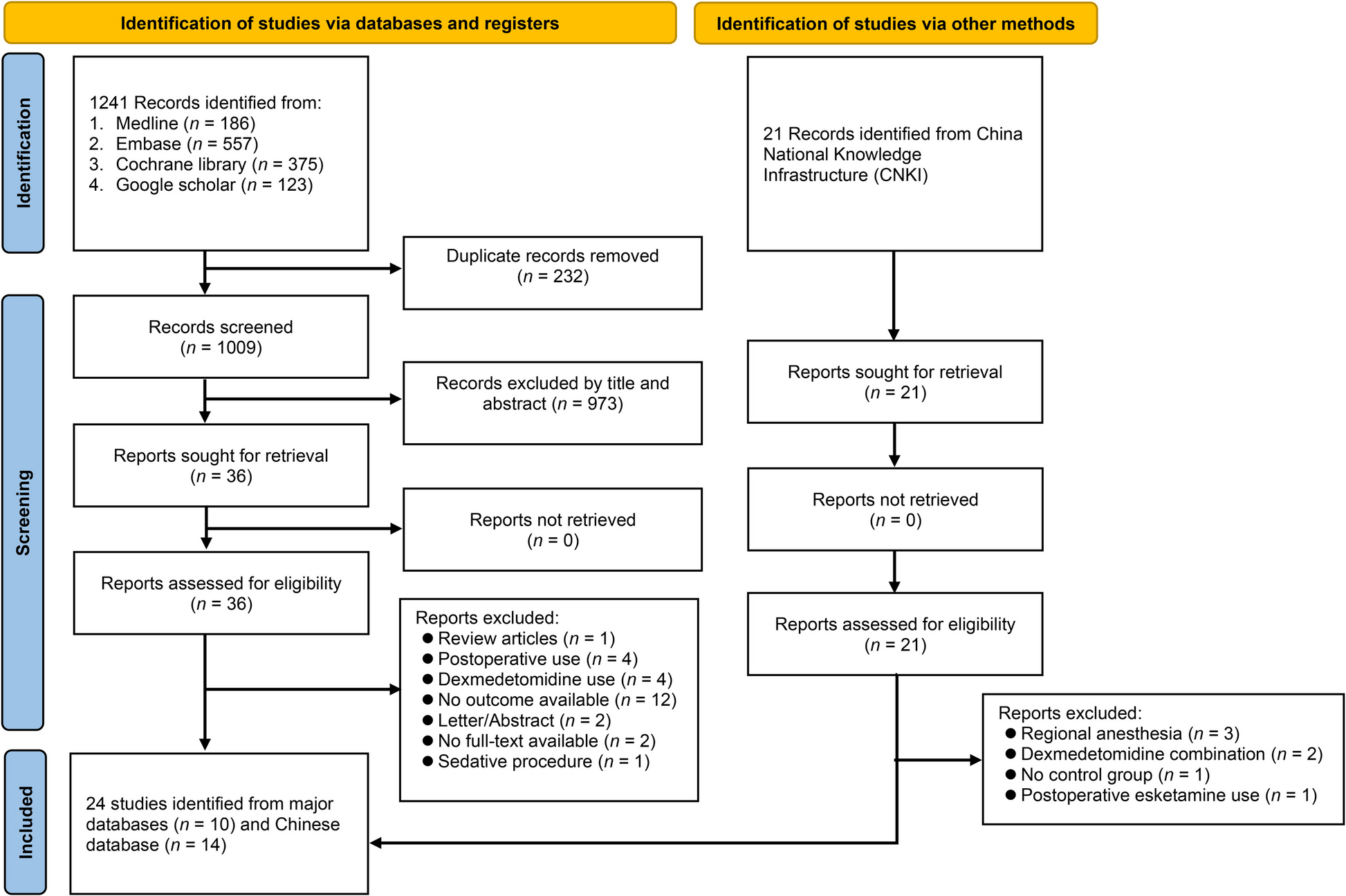
Fig. 1
Study flow diagram for the screening process
Characteristics of the included studiesAll studies used a two-arm parallel design except for Laurienzo 2013 [28]. The studies included 2682 participants (mean age 65 years). The publication year ranged from 2010 to 2022. Colorectal cancer was the most common diagnosis (11 studies, 44%) [13, 29,30,31,32,33,34,35,36,37,38], followed by lung (five studies, 20%) [39,40,41,42,43] and prostate cancer (four studies, 16%) [28, 44,45,46]. Most studies compared prehabilitation programs with usual care (17 studies, 68%) [28, 29, 33, 35,36,37,38,39,40,41,42,43, 46,47,48,49,50], while three studies (21%) [30, 32, 34] compared prehabilitation with rehabilitation (i.e., the combination of aerobic and resistance training after surgery). Other studies used controls groups of pelvic floor training [44, 45] walking training [31], no intervention [51], or inspiratory muscle training [13] (Table 1).
Description of the interventionsThe studies evaluated heterogeneous prehabilitation programs, with important differences in terms of exercise modalities and prescription rules. Eight studies (32%) evaluated the effects of combined training of moderate-intensity continuous training (MICT) and resistance training [30,31,32, 34, 40, 43, 45, 48], while three studies (12%) evaluated the combination of HIIT and resistance training [29, 35, 39]. Two studies (8%) intervened with high-intensity interval training (HIIT) [33, 47] and MICT [37, 49], respectively. Three studies (12%) combined MICT and respiratory muscle training [38, 41, 42] or combined training and respiratory muscle training [11, 13, 51]. One study [50] intervened with resistance training and respiratory muscle training and the remaining three studies (12%) evaluated pelvic floor training [28, 44, 46].
Overall, the prehabilitation programs comprised an initial warm-up period of 5 to 10 min, followed by 30 min of combined training (i.e., aerobic and resistance training), aerobic training alone, or pelvic floor exercises, followed by a cool-down period of 5–10 min. The prehabilitation programs lasted four weeks on average (SD 2.9 weeks, ranging from one to 14 weeks), with each session lasting 49 min (SD 16 min). The average number of sessions per week was 3.5 (SD 1.3). Prehabilitation was supervised in eleven studies (44%) [13, 33, 35, 36, 39, 41,42,43, 46, 47, 51], and facilitated by either therapists (32%) [13, 35, 36, 39, 42, 48, 50, 51] or by mixed groups of healthcare providers. Eight studies (32%) were conducted in mixed settings (home/clinic) [13, 29, 30, 32, 35, 43, 48, 50] and at clinics or hospitals [33, 39, 41, 42, 44, 46, 47, 51].
The reporting of training intensity varied markedly. Three studies [36, 38, 48] reported moderate to high intensity in the Borg scale. The intensity of aerobic training ranged between 40 and 85% of the maximum heart rate [13, 30, 33, 34, 40, 44,
Comments (0)