
Remember me
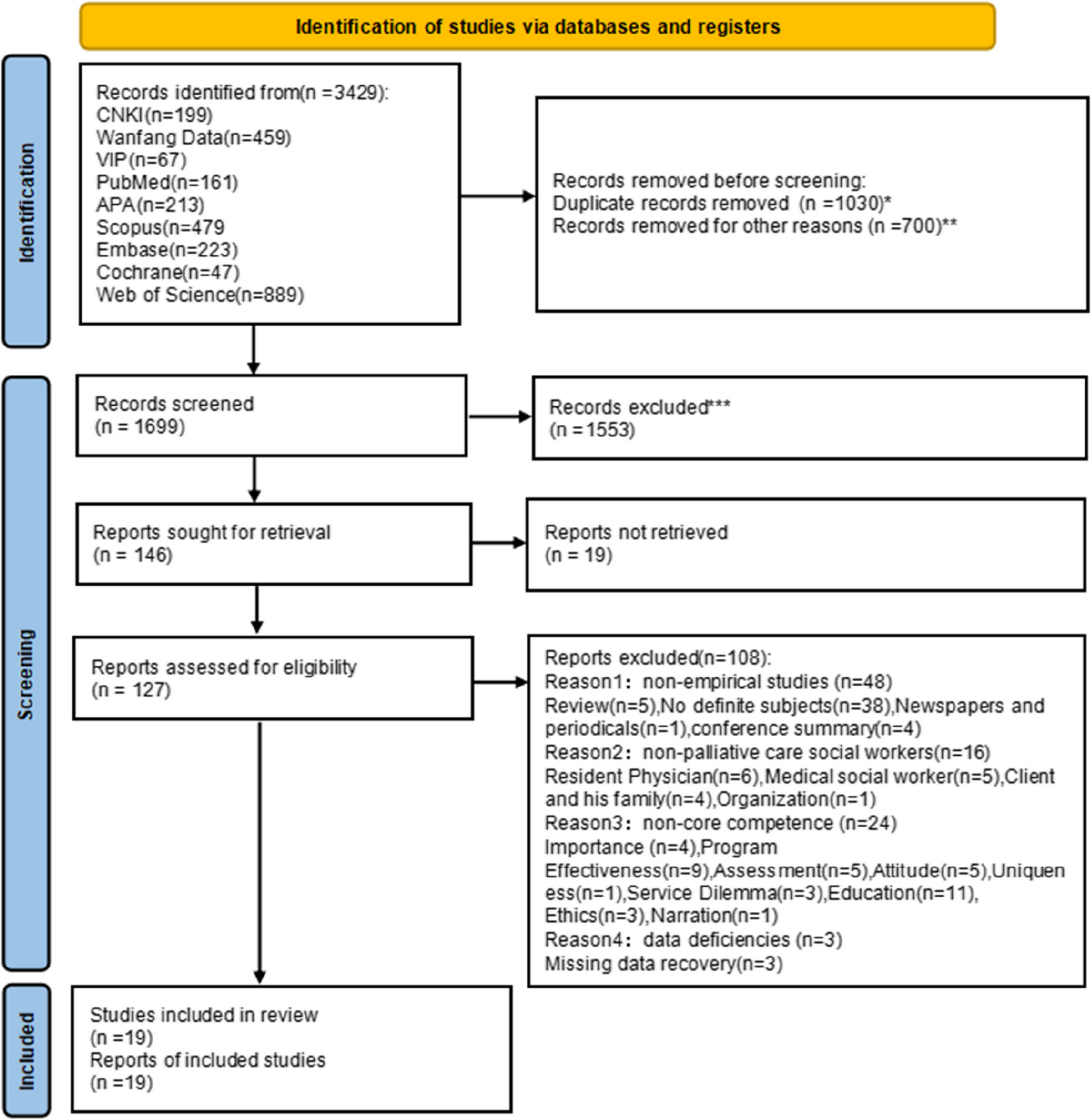
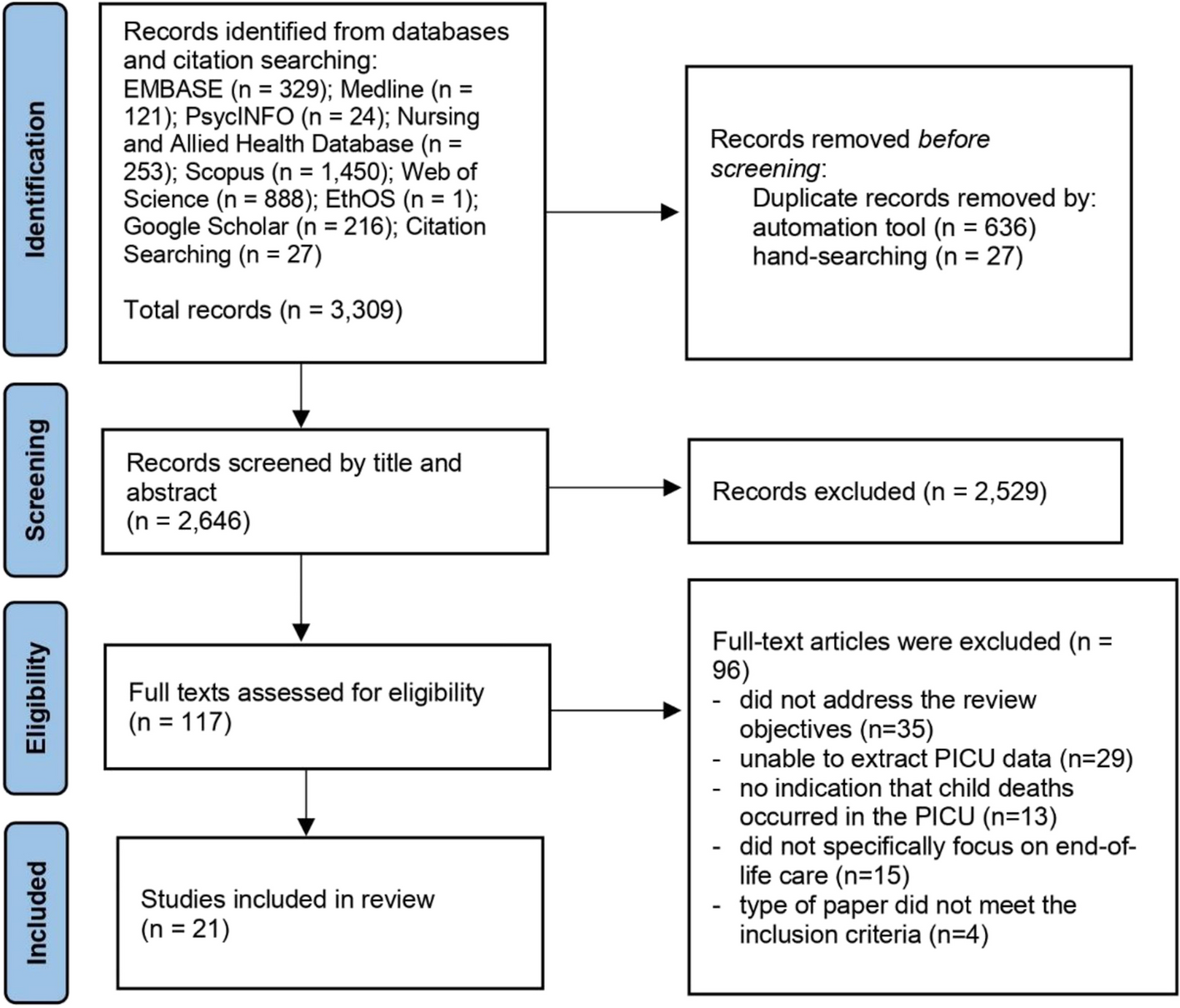
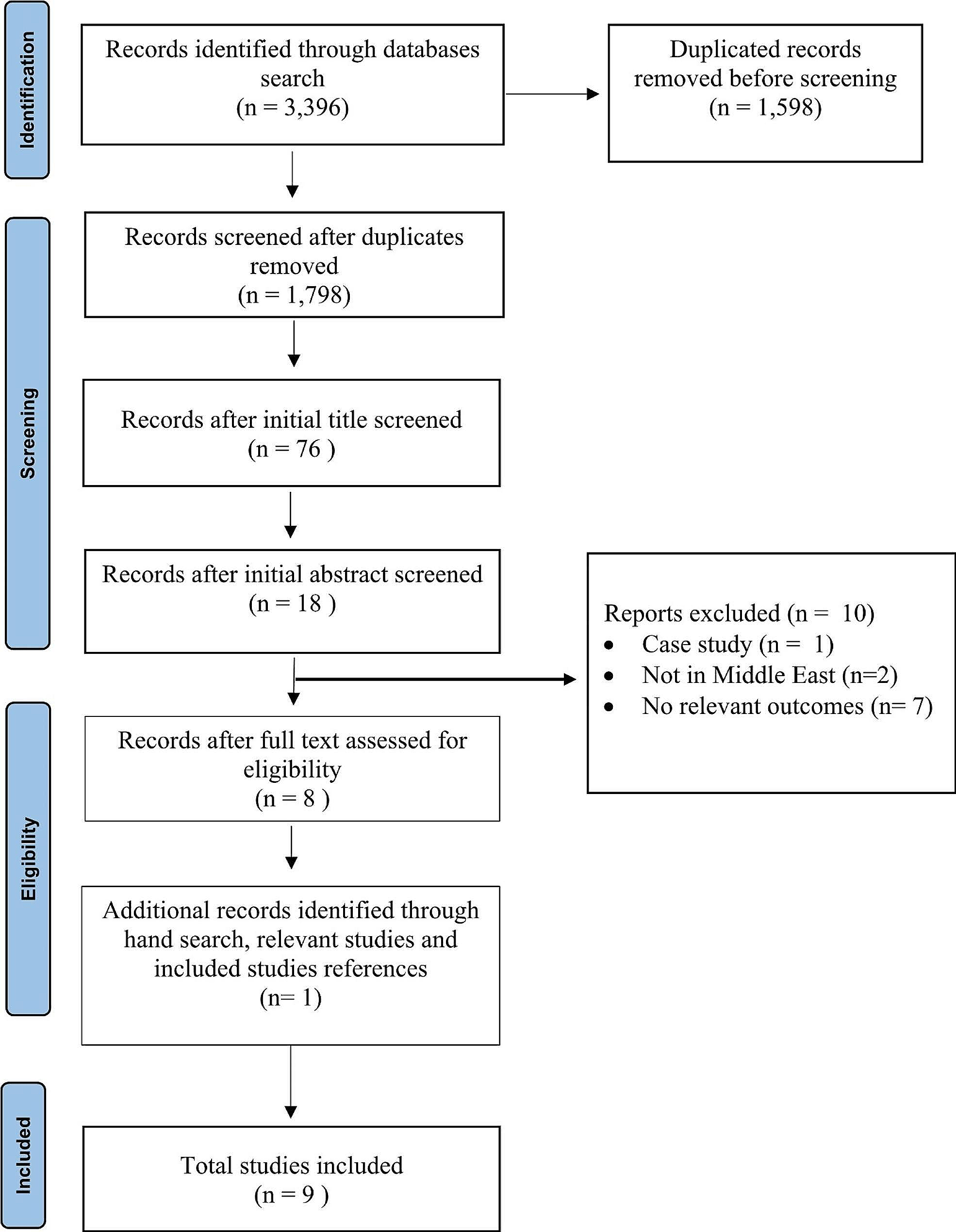

This qualitative systematic review aimed to explore the perspectives of healthcare practitioners providing palliative care to patients from culturally diverse backgrounds. Wakefield’s guide to searching and reviewing literature [28] guided and supported and the review is reported as per the PRISMA checklist (Supplementary file 1) and PRISMA flowchart [29] (Fig. 1).
Fig. 1 Search sources and strategies
Search sources and strategiesSearches were conducted within five electronic databases: PsycINFO, CINAHL, Academic Search Complete, Medline and Cochrane Library. The search strategy was based on the PICo framework (Population [healthcare practitioners], Phenomenon of Interest [perspectives] and Context [patients from culturally diverse background receiving palliative care]). The following terms were included in the search string strategy; first, for population ‘healthcare practitioners’, for phenomenon of interest ‘perspectives’ and for context ‘palliative care’ ‘culturally diverse’. All terms were joined utilizing the Boolean operators (“OR” within each search string and “AND” to combine - Table 1).
Table 1 Search terms used in database searchesCriteria for considering studies in this review were set as follows:
Inclusion criteriaPrimary research published in peer-reviewed journals.
Papers written in English or translation available.
Papers published between 01 January 2012 and 01 March 2022.
Papers referring to the adult population over the age of 18 years.
Studies which contain each of three elements: palliative intent to care, healthcare practitioners’ views or experiences and patients with culturally diverse background.
Qualitative research design.
Exclusion criteriaSecondary research – e.g., discussions, editorials, opinion papers, conference proceedings.
Literature reviews - e.g., systematic, scoping, rapid, narrative, expert, integrative.
Studies which focus primarily on advance directives and enrolment or access to hospice programmes.
Non-qualitative methodologies.
Studies where it is not possible to extract the views of the healthcare practitioner.
Study selection and data extractionAll search results were exported to Rayyan intelligent systematic review software and duplicates deleted. The remaining titles and abstracts were screened against the inclusion criteria led by the first author (CB) during which the team met to discuss the screening criteria and 20% were doubled screening by the author and the team. All studies remaining were retrieved for full text screening where the authors worked in pairs to reach a final verdict. Reasons for exclusion were noted and reported (Fig. 1). A total of 1954 papers were identified with 411 duplicates leaving 1543 for screening. Title and abstract screening resulted in 1506 been excluded, leaving 37 studies for full-text screening where full-text were read and 17 excluded. Resulting in 20 papers meeting the inclusion criteria for this review. 6 additional papers were found through backward chaining from reference lists of included papers. Data extracted was performed on all 26 papers by the first author (CB) and reviewed by the other authors (BL/OD). The data extraction table (Table 2) developed reports: authors, year, title, country, primary aim, methodology, data collection, sample size, key findings and quality appraisal score [30].
Table 2 Data extraction tableQuality assessment of the included studiesThe Critical Appraisal Skills Programme (CASP) and its supporting user guide were utilized to assess the quality of the 26 included papers. CASP allowed the authors undertake a systematic and rigorous approach through a series of ten questions, prompting the authors to consider three areas when appraising qualitative studies, the validity of the results, the nature of the results and the contribution of the results [30]. The methodological quality of the papers assessed was generally good with CASP scores ranging from 50 to 100% (Supplementary file 2).
Data analysisBraun and Clarke’s six-step thematic analysis inductive approach [31] guided the data analysis process. At first, each paper was thoroughly read to highlight relevant quotes and paragraphs, with open notes made of initial ideas and concepts. Following this quotes and paragraphs with their notes were collated into an entire data set and preliminary open coding conducted to help streamline and converge the data. Here a color-coding system assisted in highlighting patterns across the data and immersion assisted with familiarisation of the data and patterns were noted, reflected upon and discussed. This process enabled the development of broader, more conceptualized themes and the reflection and discussion process allowed for the merging and/or refining and discarding some preliminary themes. Themes were then defined and labelled followed by critically reviewing each theme and coding to assess the accuracy of the coding process leading to verification of theme.
FindingsThrough data analysis four key themes emerged from the literature (communication and connection, the role of the family in death and dying, the role of education in addressing uncertainty and institutional and societal factors) and these are presented. In addition, the characteristics of the studies include in this review are presented in Table 3.
Table 3 Characteristics of the included studiesCommunication and connectionManaging care when the patient does not speak the primary language of the country featured in the majority of studies [3, 34,35,36,37,38, 40,41,42,43, 45,46,47,48,49, 51,52,53, 55,56,57] and was commonly identified as a barrier to the provision of comprehensive care. Practitioners voiced concern that usual methods of providing support or comfort were impaired [34, 36, 48]. Participants in two studies noted that the snatches of conversations [38] and all of those small things that you say all the time [48] that help to build relationships, were missing in the absence of a common language. de Voogd et al. [36] highlights the risk of misinterpretation when statements of wishes are taken literally and viewed through the care providers’ own standpoint without exploration or clarification.
Interpreters were seen as key to addressing communication issues however, difficulties accessing the services of interpreter and variability in quality are noted [33, 37, 38, 45, 46, 48,49,50, 52,53,54,55,56, 56, 57, 57]. Green et al. [38] noted that interpreters tend only to be requested for more formal discussions around issues such as consent. Difficulties also existed when using telephone interpreter services with inadequacies of a relay conversation [37], difficulty with hearing [49] and the missing of non-verbal cues [45, 46] evident. Practitioners reported using interpreters infrequently, citing the need for advance planning and reported that in general, families preferred to interpret for themselves [34, 37, 38, 45]. The use of family interpreters raised concerns regarding the burden it may place on family members and the extent of the information conveyed [34,35,36,37,38, 45, 48, 53, 55, 57]. A number of studies note that practitioners at times felt that families may modify the information they were trying to convey in an attempt to shield the patient [34,35,36, 38, 45, 53, 56]. The utilisation of staff members as interpreters raises some concerns due to the perceived burden [53]. There was evidence of positive efforts made by practitioners to ensure patients could be understood and this was seen as a way of establishing trust [38, 40, 42, 43]. To support understanding, practitioners sometimes used unorthodox methods such as drawing up word lists [36], drawing pictures [49], using sign language [34, 55] and using an app on practitioners’ personal phones [49]. Communication triads involving healthcare practitioners, family members and the patient were utilised with support strategies such as additional time spent establishing relationships with the family [34]. While practitioners rated communication to be either moderate or good [34, 35] concerns existed regarding the content of translated information relayed to the patient as patients sometimes did not understand a particular issue but are reluctant to seek clarification [49]. Communicating in the patients’ preferred language is both an ethical and licencing responsibility [37, 38].
The importance of making connections with patients and families to forge relationships is documented in all studies. A specific emphasis on presence is discussed in a number of studies [36,
Comments (0)