The approach used for the elaboration of this mapping review followed four steps. The first step included the formulation of the clinical questions. This was based on the previous experience of the working group that elaborated clinical practice guidelines for the management of ostomies [2]. The working group decided to focus the aim of the review on a topic that was not previously extensively investigated: the management of surgical complications of ileostomy and colostomy.
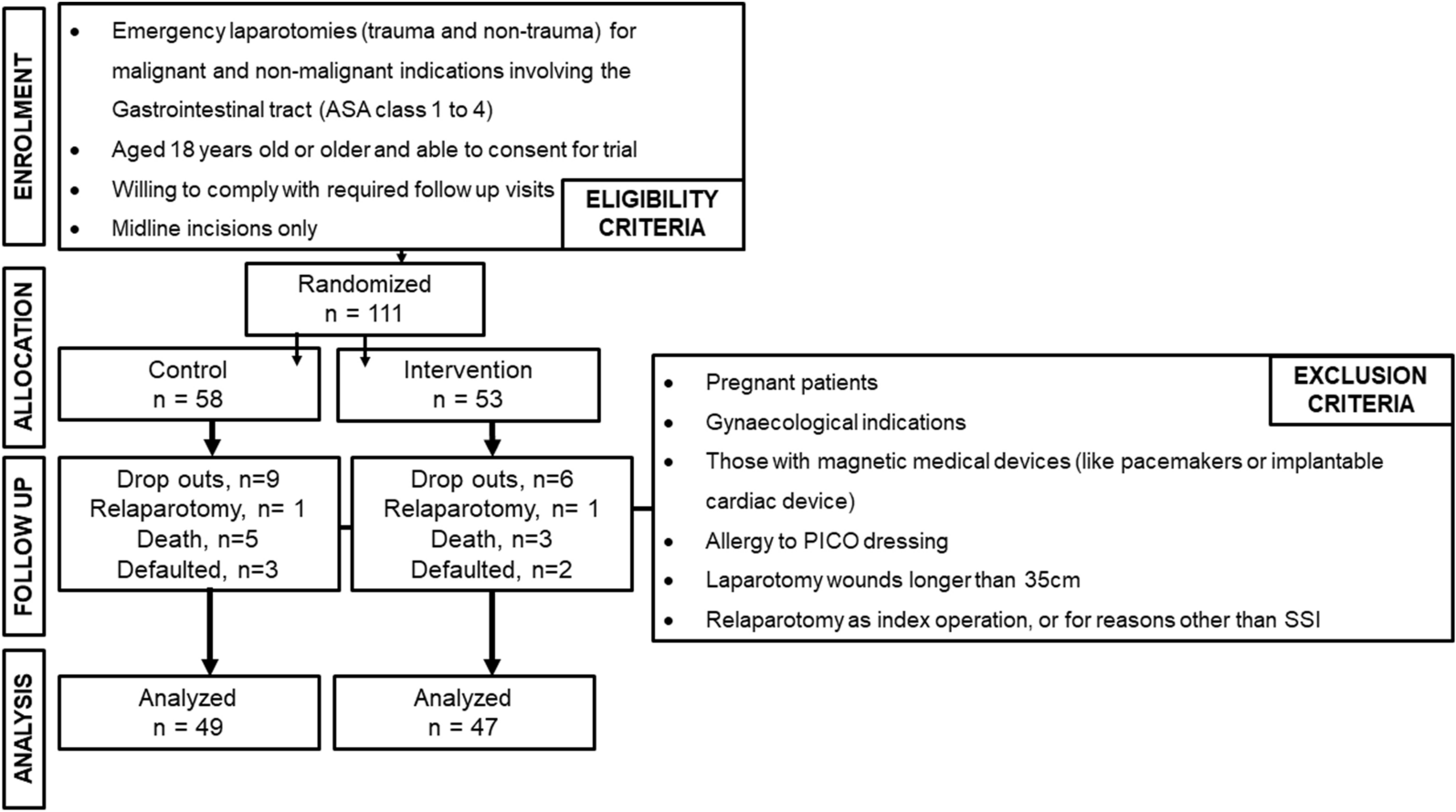
The second step was the research of relevant evidence, performed by literature search of studies from January 2011 to December 2021, with no language restriction, on this topic. After careful literature evaluation, the research group focused the study on the most frequent stoma complications needing surgical treatment, also in emergency setting: stoma necrosis, mucocutaneous separation, stoma retraction, stoma prolapse, parastomal hernia, stoma stenosis, and stoma bleeding [12]. Another important complication is dehydration with possible electrolyte abnormalities, especially in patients with ileostomy. Its management is often clinical and only in selected cases surgical resolution with early closure is possible [13]. This complication has not been evaluated in the present review, and it should need a separate study. The research was performed on PubMed, EMBASE, and Cochrane database of systematic reviews, and Scopus, and included every type of article. Exclusion criteria were studies reporting on pediatric patients (< 18 years of age), studies reporting on gastro-/oesophago- or duodenostomies as well as urostomies, studies with unclear work-up, and studies focused only on the prevention of stoma complications.
The third step included literature evaluation. When available, the most recent guidelines, systematic reviews and meta-analysis, were considered as the best evidence for their extensive literature review, including additional resources retrieved from references in analyzed articles. Then, randomized clinical trials were also considered, and, if not available, other study types, including non-randomized studies, quasi-experimental studies, cohort studies, case–control studies, descriptive studies, expert consensus, and expert opinions, were evaluated for extraction of relevant data on each specific topic. Two authors independently screened all titles and abstracts of papers identified by the search strategies for relevance. They only excluded clearly irrelevant reports at this stage. We obtained full copies of all potentially relevant papers. Afterward, the two review authors independently screened the full texts, identified relevant studies, and assessed eligibility of studies for inclusion. They resolved disagreements on the eligibility of studies by discussion and consensus, or if necessary, by consulting a third review author.
In the last step, the authors elaborated summary of the best available evidence regarding the topics of the study each of which was classified according to: definition, incidence, classification, and treatment.
Manuscript was finally reviewed and revised by an international panel from MISSTO and the World Society of Emergency Surgery (WSES).
Detailed study protocol methods and results are available in the appendix (Additional file 1).
Stoma complications
1.
Stoma necrosis
Definition, epidemiology, and classification
Necrosis of the stoma is a significant early complication that results from an inadequate blood supply, and it is divided into superficial (necrosis of the bowel mucosa) and deep (necrosis beyond the mucosa of the bowel) [14].
Definitive diagnosis between congestion and necrosis is crucial and time demanding: newly constructed stoma appears edematous and cyanotic in the immediate postoperative period but as postoperative edema decreases, the stoma usually shrinks [15]. The causes of necrosis are associated with the surgical technique in stoma creation, including tension on the mesentery, ligation of the primary blood vessel, excessive dissection of the peristomal mesentery and constriction in the abdominal wall due to excessively small opening in the fascia, abdominal wall mesh, or skin [1, 13, 16].
The overall incidence of stoma necrosis ranges between 1.6% up to 20% [13, 14, 17,18,19,20,21].
Stoma necrosis usually occurs during the few days after surgery but can present in the first postoperative months. A retrospective study on 144 patients observed end-colostomy necrosis on the ward in 14 of 80 patients (17.5%) and in 3 of 66 patients (4.5%) at 3 months [22].
Specific risk factors for stoma necrosis include emergent operations, colostomies, obesity, the use of a rod for lateral ostomy, and surgery performed by non-colorectal surgeons [4, 15, 22]. The obese patient is seven times more likely to experience stoma necrosis than the non-obese patient. Stoma necrosis is much less common for loop: in an observational study on 84 patients with lateral ileostomy the incidence of necrosis was 2.3% [16].
End-colostomies are at risk of necrosis: in a retrospective study exploring complications in standard abdominoperineal resection vs extra-elevator resection for rectal cancer, the incidence of colostomy necrosis was 35% in patients operated on in the prone jackknife position, significantly higher than in patients operated with standard procedure (13 of 38 vs. 3 of 32, p < 0.05) [23].
Intracutaneous suturing of the ileostomy was not found to be superior to transcutaneous suturing with regard to stomal complications, including necrosis (1.8% vs 3.6%), in the ISI trial [24].
The placement of a rod in constructing lateral ostomy (using a dedicated plastic rod or a part of drain or catheter) is often correlated to local necrosis [25]. Two RCT’s study reported a higher incidence of necrosis in participants managed by rods [17, 19]. In contrast, a prospective cohort study reported a higher mean incidence of stoma necrosis, but the difference was not statistically significant [18]. Another systematic review on 1004 patients concluded that there was a higher rate of stoma necrosis (rod 7% vs no rod 1.15% OR 5.58; 95% CI 1.85–16.84) in the rod group [26] (Table 2).
Table 2 Summary of treatments for stoma necrosisNon-operative management
The decision to proceed with stoma revision depends on the level of stoma necrosis in the abdominal wall [1]. The extent of ischemic changes in the mucosa can be effectively assessed using flexible (pediatric) endoscopy through the stoma site or using a proctoscope or a clear test tube or a combination of standard video bronchoscope inserted into a clear plastic blood collection tube [13, 15, 27].
If the necrosis is superficial, there is no need for revision [15]. Gentle debridement and conservative management can safely be considered, although this management strategy can ultimately result in longer-term complications such as retraction or stenosis [13]. If the length of necrosis is more than 1 or 2 cm, early revision could be considered to prevent future stenosis stoma revision, although it is important to note that stoma revision is technically much easier when early intense inflammatory adhesions and bowel and mesentery edema have subsided [15].
A cross-sectional quantitative study with narrative-type components was recently used to identify optimal interventions for selected complications, including necrosis, based on ostomy nurse expertise. Respondents reported that the management of stomal necrosis would include the use of a transparent, two-piece pouching system to allow stoma access, use of a lubricated clear test tube to check level of necrosis, and referral for debridement of necrotic tissue as necessary. Use of a nitroglycerine patch or peristomal ointment was noted as not evidence-based [28].
In selected cases, it is possible to treat superficial necrosis with negative pressure wound therapy (NPWT) by isolating the stoma and treating the peristomal wound area [29].
As with all stomal complications, necrosis results in delayed hospital discharge, increased community stoma care, and delay in the initiation of adjuvant chemotherapy for colorectal cancer patients [21].
Ostomy nurse telephone follow-up is effective to enhance postoperative adjustment of early discharged colostomy patients even in case of necrosis diagnosed at the baseline [30].
Surgical management
If the necrosis extends below the fascia, an immediate surgery is required with resection of the ischemic bowel. The extent of the bowel resection depends upon the extent of necrosis and ischemia and ultimately on the ability of the bowel conduit to reach the skin level. The surgeon must be prepared to create a new stoma at a new site [15] or, if indicated, to close the stoma. Intense inflammatory adhesions, together with bowel and mesentery edema, can make stoma revision or closing difficult during the first few postoperative weeks.
2.
Mucocutaneous separation
Definition, epidemiology, and classification
Mucocutaneous separation (MCS) is defined as a partial (partial MCS) or circumferential (complete MCS) detachment of the mucosa from the peristomal skin at various levels of deep (superficial, if it involves only epidermidis; deep, if it involves dermis and subcutaneous layers) with or without an associated abscess [1, 31, 32].
MCS is reported as the most frequent ostomy-related complication with an incidence higher than 15% [33, 34]. In a large prospective study on 1,427 stoma patients, the rate of overall ostomy-related complications was 38.8% and the most frequent complication was MCS with a rate of 18.6% [33]. This rate of MCS incidence was confirmed in another large study (retrospective) on 462 stoma patients in which the rate of MCS was 19.5%.
The presence of an ileostomy seems to represent a risk factor for the occurrence of a MCS; in this type of stoma, the risk of MCS is described in a range between 8.5% and 20.5% [33, 35, 36], higher than MCS colostomy rate (3–4%) [37]. In the group of ileostomies, the rate of MCS seems to be influenced also by the height of the distal limb of the stoma from the skin. In a large retrospective multicenter study on 4137 patients with ileostomy, the rate of MCS was higher in the group with a height of the distal limb < 1 cm (11.2 vs 2.9% with a height of distal limb > 1 cm) [32].
Conditions that increase the tension on the stoma or favor stoma necrosis increase the risk of MCS [10, 38,39,40]. In this context, as recently reported by a Chinese systematic review and meta-analysis, a demonstrated risk factor for the occurrence of a MCS is stoma support rods, which seems to double the risk of MCS if compared with ostomy created without using rod. An alternative option to standard rods, without significantly increasing the rate of MCS, is skin bridge which seems to be associated with a rate of MCS significantly lower than traditional rods [41].
Factors hindering the healing process such as infectious, malnutrition, diabetes mellitus, and chronic immunosuppressive therapy such steroids significantly increase the risk of MCS [38, 40, 42].
For stomas created in an IBD setting, the use of immunosuppressive drugs (such as vedolizumab) in the preoperative period seems to significantly (sixfold) increase the risk of MCS if compared to stoma patients who did not receive vedolizumab preoperatively, also including patients preoperatively treated with anti-TNF therapy [31, 43] (Table 3).
Table 3 Summary of treatments for mucocutaneous separation (MCS)Non-operative management
The conservative management of MCS is possible for superficial or small deep MCS. The conservative management of superficial MCS include several actions such as irrigation with isotonic saline solutions, covering of the area with absorbent or insulating products, and a more frequent replacement of the stoma device. The concomitant presence of infection, malnutrition, or other systemic causes of MCS need a correction with the help of a specialist, even when superficial, circumferential MCS needs close observation to prevent progression to deep MCS. In the presence of deep MCS, it may be effective to fill the gap using alginate or gelling fiber and cover it with a solid hydrocolloid or the pouch’s skin barrier [1, 38, 44]. In mildly symptomatic patients, a convex appliance may be useful to decrease bowel leakage [45]. If infection occurs, an antimicrobial dressing may be useful in addition to systemic antibiotic therapy [44].
Surgical management
Surgical management of MCS became necessary in deep MCS and in superficial MCS after failure of conservative treatment. Stoma revision by local repair, with partial mobilization of the proximal bowel, can be attempted, but the definitive treatment is stoma reversal, when possible, or stoma relocation by a laparotomy in a site and on a loop which secures an adequate bowel length and blood supply [11]. With this assumption, a new local approach based on the placement of a Dracon vascular prothesis was described by Feres et al. [45]. This technique consists of anastomosing a segment of approximately 5 cm of DVP at the edge of an intestinal fistula with an absorbable monofilament 4–0 thread in a continuous way, with anchors placed at the beginning and half of the suture. Theoretically, the healing process should promote the adhesion of the prosthesis to the stoma, preventing the escape of secretions to the peristomal skin, and the collection bag is properly attached to receive the effluent [45].
3.
Stoma retraction
Definition, epidemiology, and classification
Stoma retraction (SR) is commonly defined as a condition in which the stoma mucosa is more than 0,5 cm below the skin level; the term retraction usually also includes conditions in which the stoma pulls the surrounding skin inward (due to excessive bowel tension) or in which the stoma is within a skin fold (especially in a sitting position) [32, 46]. To establish a condition of SR, it is necessary to respect two criteria: dimensional (stoma must be 0.5 cm or more below the skin surface) and temporal (it appears within 6 weeks from stoma creation) [14, 47,48,49]. Temporal criteria were also used to classify the SR in early (within 30 days from surgery) and late (beyond 30 days after surgery) [48].
A large retrospective analysis on 462 ostomy patients reported a 3.2% incidence of SR, the second most frequent stoma-related complication after mucocutaneous separation [34].
It is not clear if the type of stoma, ileo- or colostomy, influences the rate of SR [47, 50]. In a systematic review and meta-analysis by Rondelli et al., there was no significant difference about the incidence of SR in ileostomy or colostomy patients (respectively 1.6% vs 3.1%) [50]. On the other hand, a prospective study by Robertson et al. reported a significantly higher incidence of SR in colostomy group (22% vs 8% in ileostomy group) during the first 10 postoperative days, but this difference was leveled at 2 years from stoma surgery (13% vs 11%) [47].
The stoma conformation seems to influence the SR rate. The creation of an end ileostomy seems to expose patients to a higher rate of SR. Van der Sluis et al. reported a rate of SR of 10% after creation of an end ileostomy [51], significantly higher than the incidence recorded in other studies analyzing loop ileostomy, which reported a range of 1.3–3% [52, 53]. The differences in terms of SR between end- or loop- stoma configuration were reported also in colostomy patients, where the rate of SR seems to be higher after a loop colostomy (13.9% vs 0.9–4% with end colostomy) [54, 55].
The use of a rod (in loop stomas) does not seem to reduce the rate of SR. In a review of 1131 stoma patients, the rate of SR in the rod group was not significantly lower than the rate recorded in patients without rod (2.3% vs 3.4%) [41, 48].
SR seems to be more frequent in patients with a high body mass index (BMI), due to the difficulty in mobilization and exteriorization of a thickened mesentery [49].
The presence of an inflammatory bowel disease (IBD) represents a risk factor for SR, due to the long-term use of steroid and/or immunosuppressive drugs and to the thickened and fibrosis of the mesentery secondary to the inflammatory disease, especially in Crohn’s disease patients. Indeed, Crohn’s disease is considered a risk factor for SR as reported by the study of Takahashi et al., in which the rate of SR in Crohn’s disease was significantly higher than the rate recorded in ulcerative colitis patients (6.6% vs 2.2%) [56].
Other reported risk factors for SR are excessive tension on the stoma, leading to ischemia and necrosis of the stoma, inadequate mobilization of the bowel, inadequate positioning of the stoma itself, aggressive postoperative fluid resuscitation, long-term steroid use, malnutrition, diabetes, smoking, poor wound healing, and peristomal infection [14, 16, 41, 47, 48, 51, 57].
The occurrence of an early SR (within 30 days from stoma creation) is more frequently due to an inadequate or difficult mobilization of intestinal loop, to large adipose tissue or to a stoma creation in a non-suitable site. High BMI and chronic peristomal dermatitis (with secondary scar tissue) represent the more frequent causes of a late SR [15] (Table 4).
Table 4 Summary of treatments for stoma retractionNon-operative management
If the bowel retraction is limited and superficial (intestinal loop at the skin or at subcutaneous level), a conservative management is possible, but a daily stoma examination is mandatory to guarantee an early diagnosis of a deeper retraction. As reported in the recent Italian guidelines on stoma care, the conservative management of a SR should include the use of a convex or flexible stoma appliance and the use of belt and other accessories (ring or hydrocolloidal strips) to increase the convexity and the adherence on the skin of stoma appliances [11].
Surgical management
Surgical revision of a retracted stoma should be considered in case of: failure of conservative approaches to allow an adequate adhesion of stoma appliances; persistent complications, especially infectious and skin complications, frequently due to a not adequate adhesion of the stoma appliances; deeper stoma retraction and risk of peritoneal contamination by stools [11].
Because the excessive tension of the bowel, primary cause of SR, is the result of an inadequate mobilization of the intestinal loop, the rationale of surgical management of SR is based on the increase in the stoma length by dissection of the bowel [15]. This result can be achieved with a local approach or, if inadequate, by a midline laparotomy. The local repair of SR is a procedure, which is performed through the stoma site and is based on the partial mobilization of the proximal bowel. However, the efficacy of the local repair depends on the level of the retraction and is possible only if the SR is due to superficial factors and not to intra-abdominal factors.
In the context of local repair of a SR, Skærlund et al. described a technique of the retracted stoma by a non-cutting linear stapler, which could be performed also in outpatient setting, and is based both on an intestinal superficial mobilization and on a stoma fixation to the skin. In this technique, the stoma is grasped with two Babcock clamps and everted at approxi





Comments (0)