
Remember me
Cytogenetic aberrations remain a cornerstone of AML classification, prognostication, and treatment allocation [1, 2]. Trisomy 8 (+8) is a common numerical cytogenetic aberration found in approximately 10–15% of AML cases, either as the sole cytogenetic abnormality, in combination with other recurrent aberrations, or as part of a complex karyotype [2, 3]. Currently, +8 without favorable or adverse defining abnormalities is categorized as intermediate-risk according to European LeukemiaNet 2022 risk classification (ELN2022) [1], despite conflicting results regarding the prognostic impact [4,5,6,7,8].
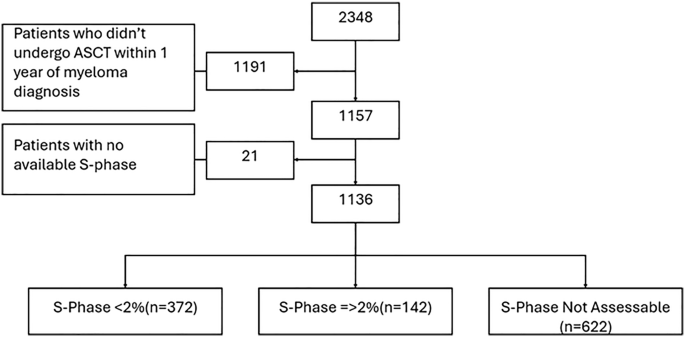
We investigated the outcomes and prognostic impact of adult patients (≥18 years) with AML (≥20% blasts in either bone marrow or peripheral blood) with +8 compared with normal karyotype (NK) who were treated with first line intensive chemotherapy between 2000 and 2022 utilizing the Danish Acute Leukemia Registry (DNLR) (see the Supplementary material) [9]. Trisomy 8 was subdivided into either isolated +8 (+8iso) or +8 with additional chromosomal aberrations (+8+add), and the additional abnormalities were classified according to the ELN2022 into favorable, intermediate, or adverse [1]. For a subset of patients, targeted deep next-generation sequencing data were available (see the supplementary material). This subset was used to explore differences in somatic mutations and assess the prognostic impact of +8 while adjusting for ELN2022 risk score [1]. The primary outcome was overall survival (OS) and secondary outcomes were early death (ED) rate (within 30 days from diagnosis), complete remission (CR) rate (within two induction cycles), relapse-free-survival (RFS), cumulative incidence of relapse (CIR), and point estimates for 1- and 5-year OS and CIR (see supplemental for statistical analysis). The study was approved in accordance with Danish legislation (ID-number: 2021-197 and 2021-011009).
Among 2,058 patients treated with intensive chemotherapy and with available karyotype data, 219 had +8, corresponding to 10.6% (Fig. S1); of these 105/219 (47.9%) had +8iso whereas 114/219 (52.1%) had +8+add. Co-occurring cytogenetic aberrations are given in Fig. S2. The NK AML comparison cohort included a total of 1,062 patients. Stratified baseline characteristics at diagnosis are given in Table S3.
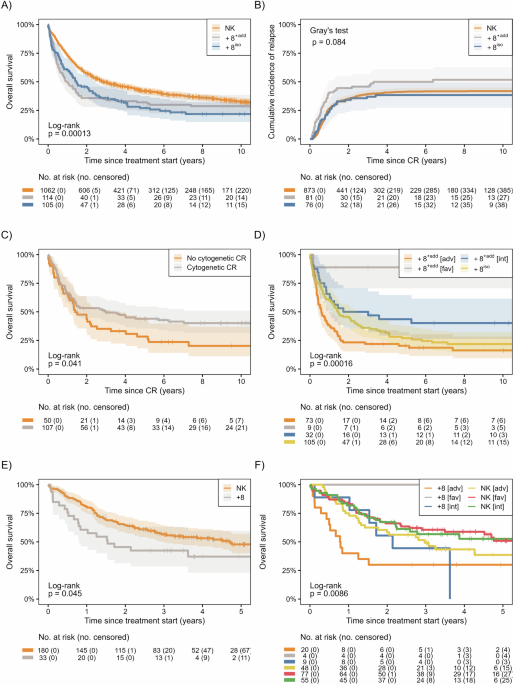
The crude rate of ED and CR for strata are given in Table S4. +8iso and +8+add had numerically lower CR rates and higher ED rates compared with NK. With a median follow-up of 10.0 years (IQR, 6.0 to 15.1), the median OS for NK was 34.4 months (95% CI, 29.7–42.9) compared to 17.6 months (95% CI, 13.4–29.3) for +8iso and 11.7 months (95% CI, 7.6 to 18.5) for +8+add (Fig. 1A). In the fully adjusted cox model for OS, both +8iso and +8+add were associated with an increased HR of 1.51 (95% CI, 1.19–1.92) and 1.59 (95% CI, 1.26–2.00), respectively, compared to NK (Table S5). The estimated difference in adjusted standardized 5-year OS were –12.9% (95% CI, –23.7 to –2.0) and –14.7% (95% CI, –21.7 to –7.0) for +8iso and +8+add, respectively, compared with NK (Table S4). In a crude age-stratified analysis, +8 was consistently associated with inferior OS (all p ≤ 0.05) in the three age strata (<50 years, 50–70 years, and ≥70 years, Fig. S3). RFS analyses showed similar patterns; in the fully adjusted Cox model, HRs for RFS were 1.31 (95% CI, 0.99–1.74) for +8iso and 1.40 (95% CI, 1.07–1.83) for +8+add, compared with NK (Fig. S4A and Table S5). For CIR the adjusted standardized differences in 5-year CIR for +8iso were −1.5% (95% CI, -13.4 to 10.3) and for +8+add 9.9% (95% CI, 0.0–21.8), compared with NK (Fig. 1B and Table S4). Among +8 patients, 157/219 (71.7%) patients achieved CR following two induction cycles, and among these, 107/157 (68.2%) achieved cytogenetic CR (cytCR). For patients achieving cytCR the fully adjusted HR for death was 0.61 (95% CI, 0.49–0.95) compared to patients not achieving cytCR (Fig. 1C and Table S6). Similarly, the RFS for patients not achieving cytCR was numerically shorter with an adjusted HR of 0.68 (95% CI, 0.45–1.03) (Table S6 and Fig. S4C).
Fig. 1: Outcomes for AML patients with +8 and NK (n = 1281).
A Crude overall survival for +8iso, +8+add, and NK, B Crude cumulative incidence of relapse for +8iso, +8+add, and NK, C Crude overall survival for +8 achieving CR stratified by the achievement of cytogenetic CR and no cytogenetic CR, D Crude overall survival for +8iso and for strata of +8+add based on the risk of the additional cytogenetic alterations (favorable, intermediate, or adverse), E Crude overall survival for subset of patients with available mutational data stratified by NK and +8 (n = 213), F Crude overall survival for +8 and NK stratified by European LeukemiaNet 2022 risk category. NB: please note the difference in time axis for panel E, F due to shorter follow-up. Shaded areas denoted 95% CIs. +8iso isolated trisomy 8, +8+add trisomy 8 with additional cytogenetic aberrations, CR complete remission, NK normal karyotype, [adv] adverse cytogenetic risk, [int] intermediate cytogenetic risk, [fav] favorable cytogenetic risk.
The crude OS according to additional cytogenetic alterations are given in Fig. 1D. In a multivariate model for OS with +8iso as reference, the fully adjusted HRs for OS were 0.09 (95% CI, 0.01 to 0.65) for +8+add with favorable cytogenetic risk, 0.58 (95% CI, 0.34 to 0.98) for +8+add with intermediate cytogenetic risk and 1.20 (95% CI, 0.83–1.75) for +8+add with adverse cytogenetic risk (Table S7).
Overall, allogeneic hematopoietic stem cell transplant (HSCT) as consolidation to first line therapy was performed for 22.3% of NK, 18.1% of +8iso, and 20.2% of +8+add. Most patients were in CR at the time of HSCT, however, 18 patients (6.5%) were transplanted in non-CR and were excluded from RFS and CIR analyses. Outcomes for OS, RFS, and CIR are given in Table S8, Table S9, and Fig. S5. In the fully adjusted model, the HRs for death for +8iso and +8+add were 0.98 (95% CI, 0.44–2.16) and 1.52 (95% CI, 0.83–2.77), respectively, compared with NK (Table S8). The adjusted HRs for RFS were 0.80 (95% CI, 0.34–1.88) and 1.67 (95% CI, 0.93–3.07) for +8iso and +8+add, compared with NK. Additionally, the adjusted 5-year standardized CIR difference was –4.9% (95% CI, –25.6 to 15.8) and 25.9% (95% CI, 3.6–48.1) for +8iso and +8+add, respectively (Table S9).
In total, 213 patients (33 with +8 [15.1%] including +8iso and +8+add, and 180 NK AML [11.2%]) had available information on leukemia-associated somatic mutations (Table S10). Generally, +8 had a lower proportion of favorable risk AML compared to NK (12.1% vs 42.8%) and a higher proportion of adverse risk AML (60.6% vs 26.7%). Mutations in RUNX1, IDH2, TP53 (with variant allele frequency >10%) were enriched in +8, whereas NPM1, bZIP in-frame CEBPA, and FLT3-ITD were more common in NK (Fig. 2A–C). With a median follow-up of 4.1 years (IQR: 3.2–5.4), the median OS for patients with NK was 56.4 months (95% CI, 35.6 to not reached) compared to 18.5 months (95% CI, 9.5 to not reached) for patients with +8, and a similar pattern was seen for RFS (Table S5 and Fig. 1E). In a fully adjusted multivariable model adjusting for ELN2022 risk, the HR for OS was 1.70 (95% CI, 1.00–2.89) and 1.64 (95% CI, 0.88–3.05) for RFS for +8, compared with NK (Table S5 and Fig. 1F).
Fig. 2: Mutational characteristics of the subset of patients with available mutational data (n = 213).
A Circos plot for NK showing co-mutational landscape, B Circos plot for +8 showing co-mutational landscape, C Oncoplot for the subset of patients showing mutational frequencies and European LeukemiaNet 2022 (ELN2022) risk categories among +8 and NK, D Barplot showing differences in mutational frequency in selected genes between NK and +8. CEBPAm CEBPA mutated, CEBPA bZIPinf in-frame mutations within the bZIP domain of CEBPA, FLT3-ITD internal tandem duplication mutation in the FLT3-gene, FLT3-TKD tyrosine kinase domain mutation of the FLT3-gene, VAF variant allele frequency.
Traditionally, +8 has been classified as an intermediate cytogenetic risk feature, a designation initially established by Grimwade et al. [2]. However, we found that both +8iso and +8+add conferred a negative 5-year OS in the magnitude of approximately 13.5% compared with NK, reflective of a classical intermediate cytogenetic risk group. This finding was confirmed in an analysis of a subset of patients with available mutational data and remained after controlling for ELN2022 risk score. The poorer OS observed was attributed to a numerically lower CR rate and higher ED-rate among all patients with +8, and for patients +8+add, an increased CIR. The inferior survival for +8iso was mitigated by HSCT, whereas +8+add was still associated with inferior survival and higher CIR compared with NK.
Trisomy 8 is a common pan-myeloid cytogenetic aberration and is distributed across different genomic classes of AML and is included in the International Consensus Classification as a myelodysplasia-related cytogenetic abnormality, though this does not per se imply an unfavorable prognosis in ELN2022 [3, 10]. In our dataset, +8 was not found to cluster more frequently with antecedent myelodysplastic syndrome compared with NK. This contrasts with previous reports from two large cohorts but is possibly explained by variations in the age composition of the cohorts [11, 12]. The prognostic significance of +8 is not fully understood, especially in contemporary cohorts with genetic information. In the landmark study by Grimwade et al., +8 was significantly associated with poorer overall survival in a multivariable model. However, +8 was excluded as an adverse risk aberration in the final prognostic scoring model based on a comparison with the intermediate-risk category [2]. Although the authors do not explicitly explain this, one possible reason could be the interaction between age and the impact of +8 observed in our study, previously underestimated when restricting to individuals <60 years old [2].
The inferior outcomes of +8 have previously been ascribed co-existing somatic mutations and not an independent effect of +8. This includes higher proportions of pathogenic variants in genes associated with adverse prognosis [4, 5, 10, 13, 14]. The present study challenges this perspective as we found that +8 has an independent and negative prognostic impact in intensively treated patients. To our knowledge, no previous study has investigated the independent prognostic impact of +8 accounting for genetic risk. Specifically, our subgroup analysis shows that the inferior OS for patients with +8 remained statistically and clinically significant after adjusting for ELN2022 risk group, with an 80% increased risk of death among +8 compared with NK.
In conclusion, AML with +8 represents a cytogenetic subgroup with significant prognostic implications, particularly when additional abnormalities are present. The findings challenge its traditional classification as an intermediate-risk feature and emphasize the need for revised risk stratification frameworks that incorporate its heterogeneity.
Comments (0)