
Remember me
Accumulating evidence suggests that blinatumomab (a CD3-CD19 bispecific T-cell engager antibody) and chimeric antigen receptor (CAR)-T cell therapy have ushered in a new era in cancer therapeutics, notably in the treatment of B-cell acute lymphoblastic leukemia (B-ALL) [1, 2]. The therapeutic landscape of blinatumomab has expanded in B-ALL, with blinatumomab increasingly appearing in earlier lines of therapy, thereby increasing the number of patients exposed to blinatumomab [3,4,5]. Both blinatumomab and CAR-T cells can trigger the immune system to fight cancer, with blinatumomab connecting immune cells and tumor cells, while CAR-T cells antagonize and destroy tumor cells through engineered receptors. Since these two treatments have similar mechanisms of action, issues regarding resistance to immune killing and T-cell exhaustion following blinatumomab also arise. Currently, the effect of sequential therapy with blinatumomab and CAR-T treatment on adult B-ALL remains unclear. This study investigated the role of prior blinatumomab on the efficacy and safety of CD19-targeted CAR-T cell therapy in patients with relapsed/refractory (R/R) B-ALL.
We pooled retrospective data on B-ALL patients diagnosed and treated with blinatumomab and CAR-T cell therapy between January 2018 and December 2023. Focusing on adult R/R B-ALL patients without a history of chronic myeloid leukemia, the primary objective was defined as the efficacy and safety of the CAR-T treatment, as measured by the complete response rate (CRR), overall response rate (ORR), and adverse events (AEs). The safety endpoint included the evaluation of treatment-emergent adverse events, graded for severity based on the National Cancer Institute Common Terminology Criteria for Adverse Events Version 5.0. Secondary endpoints included overall survival (OS) and relapse-free survival (RFS) after CAR T-cell infusion following blinatumomab. The study protocol was approved by relevant institutional review boards and conducted following principles defined by the Declaration of Helsinki.
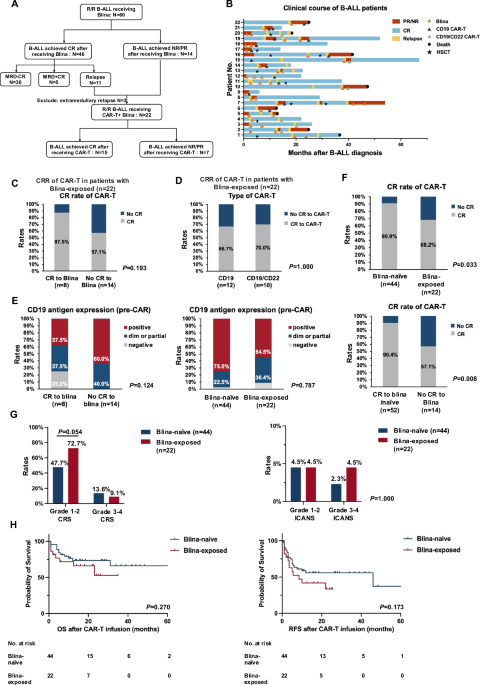
A total of 22 patients received CAR-T cell therapy after blinatumomab treatment (Fig. 1A). Ten patients were treated with CD19/CD22 dual-target CAR-T cell therapy, and 12 patients received CD19 CAR-T cell treatment (Fig. 1B). Baseline characteristics are present in Table 1. Ten of the 22 patients were male, with a male-to-female ratio of approximately 1:1. Median age at B-ALL diagnosis was 43.5 years (ranging from 18 to 62), and only 1 was over 60 years old. The most common gene alterations were TP53 mutation (14.0%) and E2A-PBX1 fusion (14.0%), each found in 3 patients, respectively (Figure S1). At least one mutation or fusion gene was identified in 19 patients (86.4%). Among the 22 patients, the ORR and CRR achieved after previous blinatumomab treatment were 76.6% and 73.3%, respectively. After receiving blinatumomab, 11 patients (50.0%) experienced cytokine release syndrome (CRS), including 2 patients (9.1%) with grade 3-4 CRS. In terms of immune effector cell-associated neurotoxicity syndrome (ICANS), only 2 patients (9.1%) developed grade 1-2 ICANS, and no grade 3-4 occurred. The median duration from the last blinatumomab dose to CAR-T cell infusion was 51.5 days (range 13-211).
Fig. 1: Characteristics of blinatumomab-naïve and blinatumomab-exposed patients.
A Flow chart of B-ALL patients. B Clinical course of B-ALL patients. C CRR of CAR-T cell therapy in patients with blinatumomab-exposed based on the prior response to blina. D CRR of CAR-T cell therapy in patients with blinatumomab-exposed based on the type of CAR-T. E Pre-CAR CD19 expression between blinatumomab-naïve and blinatumomab-exposed patients. F CRR of CAR-T cell therapy in patients with blinatumomab or not. G AEs of CAR-T cell therapy in blinatumomab-naïve and blinatumomab-exposed patients. H OS and RFS in blinatumomab-naïve and blinatumomab-exposed patients. blina blinatumomab, CRR complete remission rate, B-ALL B-cell acute lymphoblastic leukemia, CAR-T chimeric antigen receptor T, AEs adverse events, OS overall survival, RFS relapse-free survival.
Table 1 Clinical characteristics of blinatumomab-naïve and blinatumomab-exposed patients.Among these 22 patients, 8 (36.4%) achieved CR after blinatumomab treatment, and 14 (63.6%) achieved partial response/nonresponse (PR/NR). There was no significant difference in response to CAR-T cell therapy regardless of patient’s previous response to blinatumomab [87.5% vs. 57.1% (p = 0.193)] (Fig. 1C). The different targets (CD19 vs. CD19/CD22) of CAR-T cells showed no impact on the CRR of CAR-T cell therapy [66.7% vs. 70.0% (p = 1.000)] (Fig. 1D). Also, there was no significant difference in survival between the two groups receiving CD19 or CD19/CD22 CAR-T cells (Figure S2). Focusing on pre-CAR CD19 antigen expression, the rate of CD19-negative expression was relatively higher in patients who relapsed after achieving CR following blinatumomab treatment compared to those who achieved PR/NR [25.0% vs. 0% (p = 0.124)] (Fig. 1E). These two patients with CD19-negative expression received CD19/CD22 CAR-T cell therapy, and one of them obtained CR. At a median follow-up of 18.0 months, median OS was not reached, and median RFS was 8.5 months (95% CI: 1.6-15.4). The estimated 1-year OS and RFS were 71.9% (95% CI: 55.9%–93.9%) and 41.9% (95% CI: 25.0%–70.2%), respectively.
Based on 13 baseline clinical characteristics, we selected 44 patients who received CAR-T treatment from 250 patients and created a blinatumomab-naïve control group through 1:2 PSM analysis to compare them. Baseline data between these two groups remain balanced and comparable (Table 1). Efficacy results differed significantly when considering the CRR between the blinatumomab-naïve and blinatumomab-exposed groups [90.9% vs. 68.2% (p = 0.033)] (Fig. 1F). When the 66 patients were reclassified into the blinatumomab responder/naïve group and the blinatumomab non-responder group, the CRR was significantly higher in the blinatumomab responder/naïve group [(90.4% vs. 57.1%), p = 0.008] (Fig. 1F). Based on pre-CAR CD19 antigen expression, a relatively higher rate of CD19 dim/partial expression was observed in blinatumomab-exposed patients compared to blinatumomab-naive patients [36.4% vs. 22.5% (p = 0.787)] (Fig. 1E). In comparison to blinatumomab-naïve patients, the early expansion in CAR-T cell copies was less favorable in blinatumomab-exposed individuals, while there was no difference in the percentage of CD3 + , CD4 +, and CD8+ lymphocytes before and after CAR-T treatment (Figure S3).
Regarding CRS, the incidence of grade 1-2 CRS after CAR-T cell infusion was relatively higher in the blinatumomab-exposed cohort [72.7% vs. 47.7% (p = 0.054)], whereas the incidence of grade 3-4 CRS was not significantly different (Fig. 1G). Peak levels of cytokines, including tumor necrosis factor-α, interferon-γ, and interleukin-6, were significantly increased in blinatumomab-treated individuals (Figure S4). Irrespective of grade 1–2 or grade 3–4, no difference was found between the two groups in ICANS (p = 1.000) (Fig. 1G). Patients who received blinatumomab had a higher incidence of grade 3–4 neutropenia and thrombocytopenia after CAR-T cell infusion (Table S1). Other AEs, such as infection, acute pancreatitis, hemorrhage, or laboratory abnormalities like increased blood bilirubin and increased aminotransferases did not differ significantly between the two groups. Survival analysis showed no difference in OS or RFS between blinatumomab-exposed and blinatumomab-naïve patients (Fig. 1H). Besides, other factors, such as hematopoietic stem cell transplantation (HSCT), did not significantly affect the survival outcomes (Figure S5).
In this pooled analysis, we discovered that in patients who had previously received blinatumomab treatment, CAR-T cell therapy remained effective, but the efficacy was reduced compared with blinatumomab-naive patients. The possible reason for the impaired efficacy may be the downregulation of CD19 expression and T-cell dysfunction [6,7,8,9]. Consistent with our findings, studies have shown that prior blinatumomab treatment resulted in higher rates of remission failure due to antigen escape [10]. However, based on the lack of significant differences in CD19 expression between blinatumomab-naïve and blinatumomab-exposed groups, our results suggest that the emergence of CD19 escape may be a contributory factor, but not the primary mechanism. Regarding our limited number of patients, larger studies are needed to investigate whether CD19/CD22 CAR-T cells are more beneficial in patients with CD19 antigen loss. Based on the safety profile, the incidence of CRS and ICANS was comparable, and no serious AEs were observed.
In line with previous research in pediatric B-ALL [11], blinatumomab-exposed patients experienced extramedullary involvement more frequently and more frequently underwent a prior HSCT compared with blinatumomab-naïve patients. Other studies have also demonstrated that patients who have received prior blinatumomab or inotuzumab ozogamicin before CAR-T treatment do not appear to achieve higher remission rates than those who have not [12, 13]. A possible reason for these results may be that patients who require further treatment after receiving blinatumomab are more likely to relapse or be refractory, needing additional strategies to achieve long-term cure in high-risk patients. Although CR rates were higher in blinatumomab-naïve patients, OS and RFS were similar between the two groups. An analysis explaining the comparable results was that the sample size was small and insufficient to achieve statistical differences. It was also possible that the differences in outcomes between the two groups narrowed after salvage therapy such as subsequent HSCT or antibody-drug conjugates. Other limitations of this study include the relatively short interval between blinatumomab and CAR-T therapy, and these findings may not apply to the current use of blinatumomab. In summary, determining the optimal sequencing of these immunotherapies is important to help patients regain disease remission and create opportunities for subsequent transplantation or maintenance therapy. Our findings suggest that the subsequent CD19-targeted therapy after blinatumomab could provide therapeutic benefits to patients with R/R B-ALL.
Comments (0)