
Remember me
Anemia after allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a common complication, which is characterized by hemoglobin levels below the normal range, accompanied by possible symptoms such as fatigue, weakness, and dizziness. Anemia after allo-HSCT includes immune or non-immune factors [1]. Autoimmunity or alloimmunity due to blood group incompatibility often causes acute hemolysis, delayed engraftment, passenger lymphocyte syndrome, autoimmune hemolytic anemia, and pure red cell aplastic anemia (PRCA) [1]. For patients with immune anemia, corticosteroids, immunoglobulin, cyclophosphamide, azathioprine, rituximab, splenectomy, plasma exchange, erythropoietin or thrombopoietin mimetics are common therapeutic options [2]. However, infection is the most concerning complication of these immunosuppressive treatments. Therefore, it is important to detect an effective treatment for such patients.
Luspatercept is a specific activin receptor fusion protein that reduces SMAD2 and SMAD3 signaling by binding specific transforming growth factor β (TGF-β) superfamily ligands, thereby allowing erythrocyte maturation through late-stage erythroblast differentiation [3]. Based on the clinical trial data, luspatercept is the first and only FDA-approved red blood cell maturation agent to help patients reduce the red blood cell infusion burden, primarily in adult patients with low-moderate-risk myelodysplastic syndrome (MDS) with ring sideroblasts (RS) or SF3B1 mutation or myelodysplastic/myeloproliferative neoplasms with RS and thrombocytosis who were not eligible for erythropoiesis-stimulating agents or patients required regular red blood cell transfusions of beta-thalassemia. The results of an open-label phase 2 study (NCT03194542) indicated that luspatercept was also effective in treating anemia associated with myelofibrosis [4]. We conducted a retrospective study to report the efficacy and safety of luspatercept in 16 patients with anemia following allo-HSCT.
The clinical characteristics of the patients were shown in Table 1, including 13 secondary poor graft function (PGF) (81.3%), 2 PRCA (12.5%), and 1 primary PGF (6.2%). The underlying diseases were acute myelocytic leukemia (n = 6), severe aplastic anemia (n = 4), acute lymphoblastic leukemia (n = 3), myelodysplastic syndrome (n = 2), and T lymphoblastic leukemia (n = 1), respectively. The median age of the patients was 29 years (range 5–65 years). The disease status before allo-HSCT was complete response (37.5%), partial response (43.8%), and non-response (18.7%). Four patients received HLA-matched sibling donors, 4 matched unrelated donors, and 8 haploidentical donors. The blood types of 5 (31.2%) patients were matched between the donors and recipients, whereas those of 11 patients were mismatched. Patients received a median of 7.3(2.68–15.29) × 106/kg CD34+ cells. All patients obtained neutrophil engraftment with full donor chimerism, at a median of 13 days (range from 10 to 18 days) after allo-HSCT. Fifteen (93.8%) of 16 patients obtained platelet engraftment at a median time of 12 days (ranging from 9 to 27 days) after allo-HSCT.
Table 1 Baseline characteristics variables associated with luspatercept.The efficacy of luspatercept treatment was shown in Table S1. Luspatercept was initiated on a median of 134.5(39–543) days following allo-HSCT. The median number of times used by luspatercept was 1.5(1–2). The mean hemoglobin level was 58.9 (43–71) g/L vs. 82.9 (55–114) g/L before and after the first dose of luspatercept treatment (p < 0.0001; Fig. 1A). Thirteen patients (81.3%) achieved erythroid response after luspatercept treatment (Fig. S1). The median days from luspatercept treatment to erythroid response was 7(4–14). Among the 13 responders, 4(30.8%) patients remained transfusion-independent until the last follow-up, and 1 patient’s hemoglobin decreased again due to viral infection at 2 months of erythroid response.
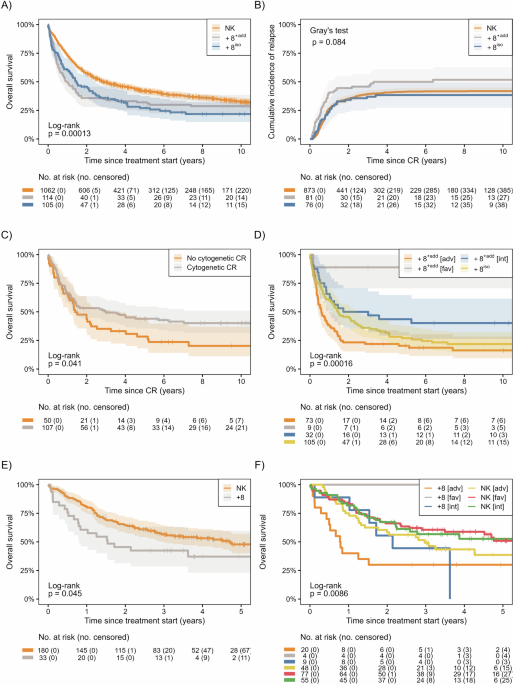
Fig. 1: Blood cell counts before and after luspatercept treatment.
The analysis included all 16 patients. A Mean hemoglobin level was 58.9 (43–71) g/L vs. 82.9 (55–114) g/L (p < 0.0001). B Mean neutrophil count was 1.7 (0.35–6.1) × 109/L vs. 2.2 (0.39–4.76) × 109/L (p = 0.26). C Median platelet count was 22.5 (3–141) × 109/L vs. 37 (5–178) × 109/L (p = 0.13).
The mean neutrophil count was 1.7 (0.35–6.1) × 109/L vs. 2.2 (0.39–4.76) × 109/L before and after luspatercept treatment (p = 0.26; Fig. 1B). At baseline, 6 patients had neutrophils <1 × 109/L, and 4 achieved hematologic improvement- neutrophil. The median platelet count was 22.5 (3–141) × 109/L vs. 37 (5–178) × 109/L before and after luspatercept treatment (p = 0.13; Fig. 1C). At baseline, 14 patients had platelets <100 × 109/L, and 4 achieved hematologic improvement-platelet.
At baseline, hypoplasia of bone marrow (BM) appeared in 6 patients (37.5%), of whom including 1 non-responder and 5 responders. There were 13 patients with an increased ratio of orthochromatic erythroblasts, including 3 non-responders and 10 responders. In two responders, the ratio of orthochromatic erythroblasts decreased. There was no significant difference in the ratio of polychromatic and orthochromatic erythroblasts in BM before and after luspatercept (Fig. S2).
During luspatercept treatment, one patient experienced fatigue, one with palpitation, and the other with limb edema. The above symptoms were consistent with grade 1 toxicity and resolved spontaneously within 1 week. No patient developed obvious diarrhea, asthenia, nausea, dizziness, back pain, or other grade 2–4 toxicities. The median follow-up time was 325 (202–758) days after allo-HSCT. By then, only one responder had died from enteric adenovirus infection combined with transplant-associated thrombotic vascular disease. The overall survival rate for all patients was 93.8%.
The optimal treatment strategy for PRCA post-HSCT remains unclear. Treatment options currently reported in the literature include high-dose steroids, eltrombopag, ibrutinib, mesenchymal stem cells, erythropoietin, plasma exchange, immunoadsorption, donor lymphocyte infusion, rituximab, bortezomib, or daratumumab therapy, and the gradual reduction or discontinuation of immunosuppression [5,6,7]. Current treatments that benefit patients for PGF include infusion of CD34-selected stem cells, eltrombopag, mesenchymal stem cells, n-acetylcysteine, anti-thymocyte globulin, and emapalumab [8]. However, the efficacy of luspatercept in treating anemia in PRCA and PGF remains unclear. Luspatercept has been studied in clinical trials in healthy postmenopausal women, β-thalassemia, MDS with RS, and primary myelofibrosis [3, 4]. These studies have shown that luspatercept has a good safety profile and can effectively increase hemoglobin levels.
Moreover, studies have shown that luspatercept was also a promising treatment method for diamond-blackfan and congenital sideroblastic anemia [9, 10]. Since ineffective erythropoiesis or dyserythropoiesis is a feature of various anemia, applying luspatercept in other anemia should be further explored, making it a new tool for treating anemia. Therefore, we explored the use of luspatercept in anemia after allo-HSCT. In our study, patients received one or two doses luspatercept at a dose of 0.8–1 mg/kg. We observed that 81.3% of patients achieved erythroid response after luspatercept treatment. Four patients remained transfusion-independent until the last follow-up. In clinical trials, luspatercept was administered subcutaneously every 3 weeks at doses ranging from 0.125 to 1.75 mg/kg. The MEDALIST trial reported a hematologic improvement–erythroid rate of 53% and a red blood cell transfusion independence rate of 38% in transfusion-dependent MDS-RS patients during weeks 1–24 of treatment [11]. In the BELIEVE trial, luspatercept enabled 11% of patients to achieve transfusion independence at any 8-week interval [12]. Therefore, the effect of luspatercept in patients with anemia after allo-HSCT is not worse than that in MDS-RS and β-thalassemia. The median time from luspatercept to erythroid response was 7(4–14) days, comparable to the 14 days reported in the PACE study [3]. The median time from luspatercept to the first response was within the first treatment cycle (12.0–24.5 days) in the BELIEVE trial [12]. We observed that the duration of erythroid response in 4(30.8%) patients was longer than 5 months. In the BELIEVE trial, among patients whose transfusion burden was reduced by at least 33% or at least 50% from baseline over any 12-week interval, the median longest duration of response for luspatercept was 104 days or 98 days, respectively [12]. Common adverse events of luspatercept include fatigue, headache, dizziness, diarrhea, asthenia, nausea hypertension, hyperuricemia, myalgia, arthralgia, and pneumonia [3, 12]. In our study, the incidence of adverse events to luspatercept was 18.8%, mainly fatigue, palpitation, and limb edema, which were tolerable.
In MEDALIST trials, luspatercept resulted in a mean increase in platelet and neutrophil counts from baseline in most patients. Moreover, elevated neutrophil and platelet counts were safe because they were elevated to the upper limit of normal. It was also found that the elevation of neutrophils and platelets was not dose-dependent [13]. Our study also observed hematologic improvement in neutrophils and platelets. The possible mechanism was related to luspatercept’s role in the proliferation of hematopoietic stem cells and progenitors by regulating extracellular matrix structure or directly inhibiting TGF-β signaling [13].
Luspatercept enabled erythroid maturation through erythroblast differentiation at a late stage [3]. In the MDS mouse model, hemoglobin and reticulocyte count rapidly and robustly increased dose-dependent on luspatercept, and the proportion of erythroid in the BM normalized [14]. One study found that patients responding to luspatercept showed a higher late to early erythroid cell baseline ratio, which increased with therapy, indicating that the terminal differentiation disorder was not completely alleviated [15]. Our study showed no statistically significant difference in the proportion of polychromatic and orthochromatic erythroblasts in the BM before and after luspatercept. Therefore, further studies are needed to investigate whether higher doses of luspatercept and longer therapy times improve hemoglobin recovery in patients with a reduced ratio of polychromatic and orthochromatic erythroblasts.
Limitations of our study were the retrospective design and the small number of cases. However, our research demonstrates that luspatercept is an efficacious treatment option for patients with anemia after allo-HSCT, causing only mild adverse events.
Comments (0)