Over 2 meetings held in March 2023 (Madrid, Spain) and March 2024 (Lisbon, Portugal), the Intercepting Blood Cancers (IBC) Workshop brought together ~75 experts in hematologic malignancies, including clinicians, clinical scientists, translational laboratory researchers, epidemiologists, representatives from the United States Food and Drug Administration (FDA), National Cancer Institute, and patient group representatives from the Leukemia and Lymphoma Society (LLS). The primary aims of these workshops were to: (1) describe current knowledge of blood cancer precursors and how these might foster early clinical intervention; (2) discuss ongoing clinical studies and any available data from these on interception modalities for early-stage blood cancers; (3) share knowledge and clinical insights between blood cancer disciplines and therapy areas, and (4) plan for publication and dissemination of consensus findings from discussions across each of the key topic tracks. These included: (A) lymphoma, chronic lymphocytic leukemia (CLL) and monoclonal B-cell lymphocytosis (MBL); (B) Multiple myeloma, smoldering myeloma and monoclonal gammopathy of unknown significance (MGUS); and (C) Clonal hematopoiesis of indeterminate potential, clonal cytopenia of undetermined significance, Myelodysplastic syndromes and acute myeloid leukemia.
Here, we highlight the key discussion points and international expert panel consensus from one of the key topic tracks: MBL/CLL. Similar summary publications for the remaining two key topics of MGUS/myeloma and myeloid precursor conditions will be reported separately. We focus this review on four broad themes that were discussed at the meetings, incorporating data from several key presentations and related discussions (Table 1): the biology of MBL, clinical implications of MBL, progression of MBL and transformation from indolent CLL to aggressive disease, and opportunities for early interception in early stage, asymptomatic CLL. We provide consensus recommendations based on the presentations and discussions during the IBC Workshops, while also drawing attention to important areas of unanswered questions requiring additional investigation.
Table 1 Highlighted IBC 2023 and 2024 presentations.Overview of the biology of MBL
MBL has historically been defined as a monoclonal population of B lymphocytes with a CLL phenotype comprising <5 × 109/liter in the peripheral blood, persisting for at least 3 months, without other features of a B-cell lymphoproliferative disorder, such as lymphadenopathy, organomegaly, cytopenias, or extramedullary involvement [1]. The delineating threshold for high-count versus low-count MBL has traditionally been defined as greater than or less than 0.5 × 109 monoclonal B-cells/liter in the peripheral blood [2]. The Genetic Epidemiology of CLL (GEC) consortium and the Mayo Clinic have produced two seminal studies on the epidemiology of MBL. In the GEC cohort, 1045 relatives from 310 families with two or more members with CLL were screened for MBL, and 22% were identified to have MBL [3]. Notably, when considering only individuals with low-count MBL, the 5-year cumulative incidence was 5.7%, with a rate of progression to CLL (i.e., to presence of >5 × 109/l monoclonal B cells) of ~1.1% per year. In the Mayo Clinic MBL Biobank cohort, over 10,000 individuals aged 40 and older were screened, with 17% identified as having MBL and the 5-year cumulative incidence of lymphoid cancer was 2.7% [4].
Recent genomic analyses have also identified that inherited variants likely play a role in the onset of MBL and its progression to CLL. A polygenic risk score (PRS) integrating 41 CLL susceptibility single nucleotide polymorphisms (SNPs) from the largest genome wide association study (GWAS) of CLL was found to associate with an ~2.5-fold increased risk of CLL, as well as with an odds ratio of 1.75 and 2.14 for risk of low-count and high-count MBL, respectively [5,6,7]. As reviewed at the meeting (Slager, IBC 2023), a subset of the identified CLL susceptibility SNPs may be associated with the initial development of the malignant B-cell clone, while another subset may be associated with subsequent MBL progression [7]. Further delineation of these subsets may help to better predict risk of both MBL development and progression, both of which may have important clinical implications.
Most large, research biobanks around the world lack screening flow cytometry data to enable detection and investigation of MBL, but contain genetic and rich phenotypic data for hundreds of thousands of individuals [8, 9]. Chromosomal alterations associated with CLL—data for which already exist in such biobanks [10,11,12,13]—are highly specific for the presence of a circulating B-cell clone, as presented in a study at the meeting (Sekar, IBC 2024). Incorporating chromosomal alteration data with additional types of readily available data, such as absolute lymphocyte count, may enable detection of high-count MBL in large biobanks without the need for flow cytometry [14]. Such an approach could enable large-scale studies of high-count MBL to comprehensively understand its causes and consequences beyond what has been possible in smaller studies that have relied on traditional flow cytometry-based analyses. Further work will be necessary to evaluate the feasibility of such an approach for individuals with low-count MBL.
The interplay of infectious and environmental exposures may additionally contribute to MBL pathophysiology, as reflected by geographical variations in incidence and MBL phenotype (Rawstron, IBC 2023), though data on the potential connection between preceding infection and MBL development is mixed [15]. In a cross-sectional study of hospital-based populations in the United Kingdom and rural Uganda, the overall prevalence of MBL was higher in the Ugandan cohort than the United Kingdom cohort (14% versus 8%), and notably a higher prevalence of an atypical CD5-negative immunophenotype MBL was observed in Ugandan participants [16]. This phenotypic heterogeneity raises the possibility of fundamental differences in the pathogenesis of MBL in different geographical settings, which will require further elucidation. The interplay between the MBL clone and antigen stimulation, including foreign, geographically-specific antigens has been further emphasized by the identification of monoclonal population together with the evidence of increased prescription of specific antimicrobials up to two decades prior to diagnosis of CLL [17, 18]. Additionally, it was noted that patients with high-count MBL or early stage CLL who have a non-malignant B cell count of <20/µL have a decreased overall survival compared to those with a non-malignant B cell count above this threshold (Rawstron, IBC 2024), pointing to a potentially relevant role of immune dysfunction in the overall outcome of individuals with MBL. This widely available and easy to test prognostic marker could potentially be incorporated into clinical risk stratification after further validation.
With regard to the etiology of MBL, two complementary studies were presented, which both suggested molecular harbingers for the eventual development of MBL or CLL that can arise in some cases many years before diagnosis. In one study, the B-cell receptor (BcR) immunoglobulin heavy chain (IGH) gene repertoire was sequenced in blood samples from 124 patients with CLL compared to 118 matched controls, with some samples taken as long as 22 years before diagnosis [19]. Prior to the development of lymphocytosis, skewing of the BcR IGH gene repertoire was observed for most individuals, irrespective of the clonotypic IGH variable (IGHV) gene somatic hypermutation status. In some cases, signatures of higher risk immunogenetic clonotypes could be detected up to 16 years before a diagnosis of CLL (Langerak, IBC 2024). In another study, peripheral blood from 191 siblings of CLL patients was analyzed by flow cytometry, and detected 0.2-480 clonal CLL-phenotype cells per microliter (median: 37/μL) in 34 of the siblings (17.8%) [20]. Additional genotyping was performed by SNP array, as well as by whole exome, and targeted panel sequencing. Between CLL patients and MBL siblings, CLL risk alleles were found with high and similar prevalence, respectively; however, copy number variations were often subclonal in MBL cells, suggesting that they may be acquired subsequently during subclinical clonal expansion (Veelken, IBC 2024) [20]. Overall, these two studies suggest that a preclinical phase of CLL may arise many years before eventual diagnosis, and additionally they support a stepwise model of CLL pathogenesis, in which autonomous BcR signaling leads initially to clonal expansion of CD5 + B cells, with subsequent progressive disease to eventual CLL following additional pathogenic mutations.
Indolent to aggressive transition
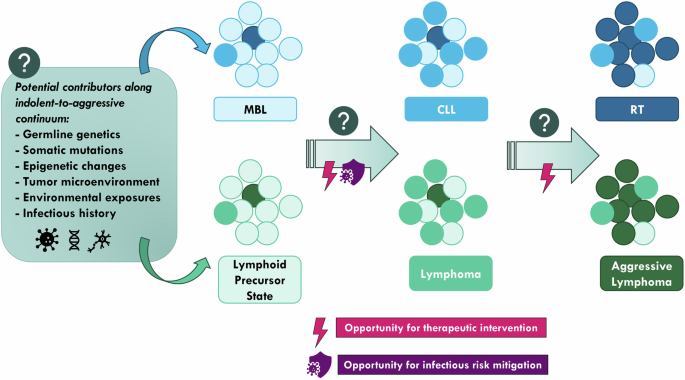
An important aim of the scientific investigation into the biology of precursor malignant states centers on achieving the eventual goal of being able to intercept the process of indolent disease transforming to a more aggressive one. Key transition points reviewed included progression of MBL to CLL as well as CLL to Richter Transformation (RT).
One important distinction within MBL is that low-count MBL is, in fact, immunogenetically distinct from either high-count MBL or CLL, which may be reflective of distinct antigenic pressures (Stamatopoulos, IBC 2023). In a study characterizing BcR IG stereotypes in individuals with or without low-count MBL, it was found that in patients with low-count MBL, the major CLL BcR IG stereotypes were expressed at low frequencies and did not mirror the trends seen in patients with CLL [21]. Furthermore, there was an absence of BcR IG stereotypes similar to those of CLL subsets associated with aggressive disease. At the same time, in a recent analysis of selected patients from the European Prospective Investigation Into Cancer and Nutrition (EPIC) cohort, it was reported that dominant BcR IG clonotypes belonging to major stereotyped subsets associated with poor prognosis could be identified up to 16 years before diagnosis in individuals who were healthy at enrollment and later developed CLL [19]. (The EPIC cohort of patients was a prospective cohort of over 50,000 patients from 10 European countries initially assembled to investigate the association of fruit, vegetable, and fiber consumption with cancer development). Taken together, these findings raise important questions regarding the heterogeneity of low-count MBL, how certain individuals with low-count MBL may progress to high-count MBL, and then eventually CLL, and the important role that the BcR and microenvironmental interactions may play in that pathologic progression.
While CLL often has a relatively indolent disease course, about 5–10% of patients will develop transformation to an aggressive lymphoma, termed RT, which unfortunately carries a very poor prognosis, with median survival only in the range of 6–12 months [22]. Recent research has propelled an increasing understanding of the complex interplay between genetic, epigenetic, immunologic, and tumor microenvironmental factors contributing to RT, but many unanswered questions remain [23]. Comprehensive genomic characterization of paired CLL and RT samples has revealed important insights into clonal relation and key RT subtypes [24], and lays the foundation for the application of cell-free DNA analysis as a potential tool for early diagnosis and monitoring of RT (Parry, IBC 2024). In another recent study, genome-wide sequencing of serial samples from patients with CLL collected prior to the diagnosis of RT and at the time of RT diagnosis resulted in the remarkable finding of “early seeding”—the malignant RT clone was identified in very early timepoint samples, up to 19 years before the time of diagnosis in one case [25]. This principle of early seeding may have important implications. If early seeding can be identified in clinical practice, it could lead to early diagnosis of RT/or RT-potential even before clinical manifestations arise, presenting an opportunity for early therapeutic intervention.
One such potential intervention avenue arising from results of these studies is to thwart oxidative phosphorylation, as higher levels have been associated with RT development (Martin-Subero, IBC 2023). Effectively targeting oxidative phosphorylation with electron transport chain inhibitors has proven to be challenging, but as the field of cancer therapeutic agents continues to evolve, such therapeutic strategies could eventually be leveraged, and additional preclinical work has demonstrated concomitant targeting of MYC and oxidative phosphorylation in RT [26]. Successful early intervention could potentially thwart the development of RT and lead to improved outcomes for patients, although the latency of nearly two decades in at least some cases implies some individuals may succumb to other health conditions before clinical transformation occurs. If such a therapeutic paradigm is eventually established, the question then arises regarding what interventions would be optimal. Investigation would require thoughtfully designed clinical trials, taking into account the potential heterogeneity of prior CLL-directed treatments a patient may have received. An intriguing question was additionally discussed: if a RT clone is identified during initial observation, does the presence of that RT clone alone warrant treatment in a patient who does not otherwise meet iwCLL treatment criteria? Could such treatment trigger or even catalyze subsequent transformation through selective pressure? While there is still much to be elucidated regarding the pathophysiology of transformation of CLL to RT, advancements in comprehensive assays are enabling an increased understanding of this area of particularly unmet clinical need, which may, in turn, pave the way for more effective interventions.
Clinical implications of MBL
Consequences of precursor conditions are not limited to progression to frank malignancy. Perhaps best characterized for MBL is the associated immune impairment, which has important clinical implications. Comprehensive characterization of the immune repertoire demonstrated differences even in circulating T cells and NK cells in patients with low-count MBL, and an increased prevalence of infections [27, 28]. A separate cohort study had demonstrated that the risk of serious infection was greater in patients with MBL versus those without, and this risk applied even to individuals with low-count MBL [29]. This immune impairment became even more apparent during the COVID-19 pandemic, where a strong association between low-count MBL and more severe COVID-19 infections was observed [30, 31]. In one study, the prevalence of low-count MBL was detected in 29% of patients with COVID-19, compared to only 14% in the general population, with an even higher prevalence in patients admitted to the hospital and those critically ill [30]. Interestingly, immune characterization studies revealed that in patients with active COVID-19 infection, anti-SARS-CoV-2 antibody levels and blood circulating plasma cell counts demonstrated a delayed peak compared to patients without MBL, with decreased numbers of pre-germinal center B cells observed, but interestingly with significantly greater SARS-CoV-2 antibody levels, at least transiently (Orfao, IBC 2023) [32].
Overall, the precise mechanisms of immune dysregulation in MBL still remain poorly understood, and an increased understanding could be leveraged for potential interventions to reverse the immune impairment. Although vaccine responsiveness may be impaired, the importance of vaccinations for such individuals cannot be understated. Additional impacts of a diagnosis of a precursor malignant condition include an increased risk of secondary malignancies [33], mental health challenges, and financial burden; further research is needed to better characterize these sequelae of MBL (Rawstron, IBC 2023). These considerations become even more relevant when considering the potential for inherited susceptibility to MBL/CLL and the implications such an established diagnosis could have for individuals. Indeed, a PRS including multiple SNPs led to about a 2.5-fold increased risk of CLL in the Mayo Clinic database, distinct from low-count MBL, where this PRS led to only a 1.75-fold increased risk of developing low-count MBL (Slager, IBC 2024) [7].
Opportunities for therapeutic intervention in early CLLCurrent lack of early intervention strategies in CLL
Despite major advances in the treatment of CLL in the past decade, “watch-and-wait” remains the standard of care for MBL and asymptomatic patients with CLL. The 2018 International Workshop on CLL (iwCLL) Guidelines recommend withholding treatment until patients develop significant CLL-related symptoms or organ dysfunction such as persistent B symptoms, progressive cytopenias, or symptomatic lymphadenopathy or hepatosplenomegaly [34]. However, even in the absence of classic treatment indications, patients with CLL often experience complications of the disease which can fall into 4 major domains: (1) increased frequency and severity of infections [27, 35, 36], with infections being the major cause of death for patients with CLL [37]; (2) hampered immune response to vaccinations [38, 39]; (3) increased incidence of second primary cancer [40,41,42], with worse second primary cancer outcomes [43]; and (4) impaired psychosocial well-being [44]. Specifically, patients in the low-risk category of CLL International Prognostic Index (CLL-IPI) are twice as likely to die from infection or second cancers (6%) than CLL progression (3%) [35]. These data highlight immune failure as a key clinical challenge in CLL and call for an intervention strategy that can alter the natural history of the disease and immunosuppressive effects of CLL.
Prior early intervention trials in CLL
All randomized phase 3 trials investigating early intervention in CLL have thus far failed to demonstrate a survival benefit compared to ongoing observation [45,46,47,48,49,50]. Both chemotherapy and chemoimmunotherapy approaches have been studied, including chlorambucil [46], fludarabine [47], and the combination regimen of fludarabine, cyclophosphamide, and rituximab (FCR) [48]. The CLL12 study was the first to examine early intervention with a targeted therapy in CLL. In this trial, 363 patients who did not meet iwCLL treatment criteria but did have markers of increased genetic risk of their CLL were randomized to the Bruton’s tyrosine kinase inhibitor ibrutinib versus placebo [49]. This study enrolled relatively young (median age of 64 years) and fit CLL patients early in the disease course (median 9 months from CLL diagnosis to randomization). In the initial publication, with a median follow-up of 31 months, the number of deaths was too few to compare survival between the study arms. As expected, early treatment with ibrutinib prolonged event-free survival defined by disease progression, initiation of next CLL-directed therapy, or deaths. However, adverse events frequently occurred during treatment with ibrutinib, which included cardiac arrhythmia (22% any grade [G], 8% G3+), hypertension (10% any G, 1% G3+), and bleeding (34% any G, 4% G3+). One third (36%) of patients eventually stopped ibrutinib early, mostly due to toxicity (82%). Updated analysis of CLL12 was presented with a median observation time of 69.3 months which demonstrated no difference in overall survival between the two arms (Langerbeins, IBC 2023) [50, 51]. As such, the consensus of the group remained that early intervention in CLL, even with a targeted therapy like ibrutinib, is not supported by current data and bears further investigation before potentially becoming a standard of care.
Ongoing early intervention trials in CLL
Can alternative therapy improve the outcome of early, asymptomatic CLL while minimizing toxicity? Ongoing research efforts are exploring whether a second-generation BTK inhibitor with a relatively favorable safety profile might improve the benefit:risk ratio relative to what was observed with ibrutinib in CLL12. At the meeting, an ongoing phase 2 study at the Mayo Clinic was reviewed, which is studying a selective BTK inhibitor, acalabrutinib, with or without obinutuzumab in patients with CLL who do not meet the iwCLL treatment criteria (NCT03516617) (Parikh, IBC 2024). This study uses the CLL-IPI, which incorporates the following 5 variables—age, Rai stage, deletion 17p and/or TP53 mutational status, IGHV gene mutational status, and serum β2-microglobulin level—to direct patients into the randomization. Patients with a high or very high risk CLL-IPI score are assigned to one of the two interventional arms, which both consist of at least 2 years of acalabrutinib-based therapy. Patients who achieve undetectable minimal residual disease with complete response will discontinue therapy, whereas patients still with residual disease will continue on therapy.
Increasingly, the CLL field is evolving toward time-limited therapeutic approaches utilizing the oral B cell lymphoma/leukemia-2 inhibitor venetoclax as a backbone of various combination regimens. The phase 3 EVOLVE-CLL (S1925) study is a large, randomized trial being conducted by the U.S. Intergroup Cooperative groups targeted at newly diagnosed CLL patients with CLL-IPI score of 4 or higher and testing early versus deferred intervention with 1-year of venetoclax and obinutuzumab (NCT04269902) (Stephens, IBC 2023). The primary endpoint of the study is overall survival, with a planned sample size of 247 patients. Another time-limited venetoclax-based early intervention study is the randomized, phase 2 PreVent-ACaLL trial in Denmark, Sweden, and the Netherlands, which employs an even shorter duration of therapy with 12 weeks of acalabrutinib and venetoclax (NCT03868722). Other notable components of this study include its primary endpoint, which is infection-free survival rather than conventional efficacy endpoints, and the application of an innovative machine learning-based model (CLL-TIM) [52] for the selection of eligible patients with increased risk of infection and need for CLL treatment (Niemann, IBC 2024). The CLL-TIM model has also been deployed as an open-source decision support tool, adjoined to the EPIC-based electronic health record system of Eastern Denmark, providing a practice-based guideline for deployment of data-driven decision support tools in hematology [53].
Advances in genomic sequencing and analytic pipelines for neoantigen discovery have facilitated the development of individualized cancer vaccines, leading to the successful completion of early intervention studies in melanoma using peptide- [54] or mRNA-based [55] cancer vaccines. However, the qualitative and quantitative defects in CLL host immunity pose unique challenges in applying a vaccination strategy [56], raising the need for multiple vaccine doses [39, 57] and additional immunomodulation to maximize the effectiveness of the vaccine [58, 59]. An ongoing phase 1 study of a neoantigen peptide vaccine in asymptomatic CLL targets patients with a high risk of disease progression, as defined by having an unmutated IGHV gene mutation status, was presented (NCT03219450) (Ahn, IBC 2023 and 2024). The study is comprised of three non-randomized treatment arms to explore the activity of a personalized neoantigen peptide vaccine and the role of additional immunomodulation in generating vaccine responses; the arms are as follows: arm (1) vaccine only; arm (2) vaccine with low-dose cyclophosphamide (to inhibit regulatory T cell-mediated immune suppression); arm (3) vaccine with cyclophosphamide and pembrolizumab (to augment anti-CLL tumor immunity through PD-1 checkpoint blockade).

Comments (0)